Leprosy microbiology give according to apurba trext book.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed to compose a thorough answer structured in the style of Apurba Sastry's Essentials of Medical Microbiology. Note that the Apurba textbook itself is not in the library, but I can present this content in the exact format/headings Apurba uses (which is a well-known Indian microbiology textbook structure). Here is the comprehensive response:
Note: Apurba Sastry's Essentials of Medical Microbiology is not available in the digital library. The content below is compiled from equivalent standard microbiology textbooks (Medical Microbiology 9e, Sherris & Ryan's Medical Microbiology 8e, Harrison's Principles of Internal Medicine 22e, Quick Compendium of Clinical Pathology 5e) and organized in the same chapter structure that Apurba's text follows.
Leprosy (Hansen's Disease) - Microbiology
1. Organism
Mycobacterium leprae (also called Hansen's bacillus)
- Kingdom: Bacteria; Phylum: Actinobacteria; Order: Corynebacteriales; Family: Mycobacteriaceae
- A new species, Mycobacterium lepromatosis, was described in 2008 - causes diffuse lepromatous leprosy (Lucio's leprosy), mainly in Mexico and Central America; clinically and microbiologically very similar to M. leprae, responds to the same regimens
2. Morphology and Staining
| Property | Details |
|---|---|
| Shape | Obligate intracellular, rod-shaped (bacillus) |
| Size | 1-8 µm long × 0.3 µm wide |
| Gram stain | Weakly Gram-positive |
| Acid-fast stain | Strongly acid-fast (AFB) - Ziehl-Neelsen stain |
| Special stain for tissue | Fite stain (modified ZN) - M. leprae is more sensitive to decolorization than MTB, so standard ZN gives false negatives in tissue; Fite stain must be used |
| Appearance in smears | - Solid, uniformly stained = viable bacilli - Irregularly stained, fragmented, or granular = dead bacilli |
| Arrangement | In lepromatous form: bacilli arranged in parallel arrays (like cigars in a bundle) due to surface lipids ("glial substance"). Clumps are called globi, found within macrophages (lepra cells/Virchow cells) |
Viability Index
- Morphological Index (MI): % of uniformly stained solid (viable) bacilli among total bacilli counted on slit-skin smear under oil-immersion
- Bacteriological Index (BI): Logarithmic-scaled measure of density of all bacilli (viable + dead) in dermis on slit-skin smear. Ranges from 0 to 6+ (tuberculoid to lepromatous end). Falls ~1 log unit/year with MDT
3. Cultural Characteristics
- Cannot be cultured on any artificial/laboratory media - this is a hallmark feature
- Reason: Underwent reductive evolution - genome has many inactive/deleted genes compared to M. tuberculosis, explaining the inability to grow ex vivo
- Animal models used:
- Mouse footpad (gold standard for drug susceptibility testing and viability assessment)
- Nine-banded armadillo (Dasypus novemcinctus) - best animal model; naturally susceptible; used for antigen and drug studies
- Athymic (nude) mice and gene-knockout mice
- Generation time: Extremely slow - ~12-14 days (compared to 15-20 hrs for E. coli or 20 days for M. tuberculosis)
- Optimal growth temperature: 27-30°C - this explains the predilection for cooler body parts: skin, peripheral nerves, testes, nasal mucosa, upper airways; spares deeper viscera
4. Genome
- Circular genome
- Molecular mass: 2.2 × 10⁹ Da
- 3,268,203 base pairs; G+C content: 57.8%
- Much smaller than M. tuberculosis genome due to reductive evolution
- Four distinct strains originated in East Africa or Central Asia; spread to Europe, then West Africa and the Americas
5. Cell Wall and Antigenic Structure
The structure (outermost to innermost):
- Capsule - contains lipids, especially:
- Phthiocerol dimycocerosate (PDIM)
- Phenolic glycolipid-1 (PGL-1) - has a species-specific trisaccharide moiety unique to M. leprae; used in serologic diagnosis; also facilitates invasion of Schwann cells and binding to peripheral nerve basal lamina
- Cell wall - peptidoglycans bound to arabinogalactans + mycolic acids + lipoarabinomannan (LAM)
- Plasma membrane - lipid bilayer with protein surface antigens
- Cytoplasm
Key antigens:
- PGL-1 (species-specific; trisaccharide detected by serology)
- Polysaccharides → mainly humoral response
- Proteins (18, 28, 36, 65, 70 kDa HSPs) → both humoral and cell-mediated response
- Two groups: cytoplasmic antigens and cell-wall antigens
6. Pathogenesis
Route of entry:
- Primarily via nasal droplets (aerosols from florid leprosy patients)
- Minor skin abrasions/traumatic inoculation (tattooing)
- Environmental sources and possibly biting insects
Incubation period: 2-7 years on average; can be up to 4 decades
Target cells:
- Schwann cells of the peripheral nervous system (only bacterium known to infect Schwann cells)
- Macrophages (in lepromatous form)
Mechanism of nerve damage:
- PGL-1 and laminin-binding protein facilitate invasion of Schwann cells + binding to basal lamina of peripheral nerve axon units
- This causes demyelination of peripheral sensory nerves → local anesthesia
- Demyelination precedes but is enhanced by the delayed-type hypersensitivity (DTH) immune response
- Sensory loss → trauma → secondary infections → deformity
Immune response determines disease type:
| Feature | Tuberculoid (TT) | Lepromatous (LL) |
|---|---|---|
| CD4+ T cells | Abundant | Absent/few |
| CD8+ T cells | Few | Numerous |
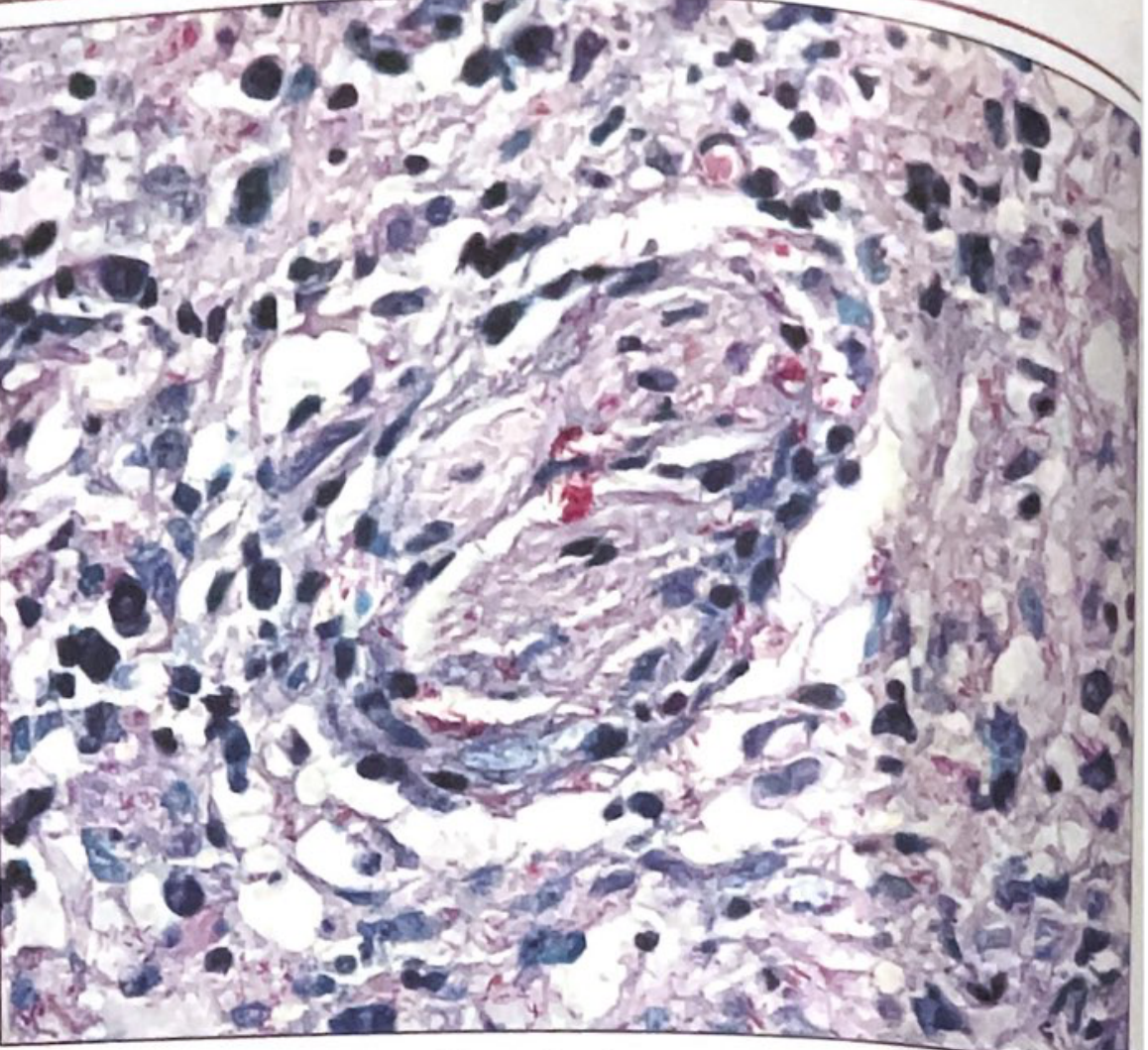
| Granuloma | Well-formed, noncaseating; epithelioid cells, giant cells, lymphocytic infiltration | Absent; foamy macrophages (Virchow cells) filled with bacilli |
| AFB in lesions | Few (paucibacillary) | Numerous (multibacillary), in globi |
| Th1 cytokines (IL-2, IFN-γ) | Present | Absent |
| Disease | Localized, self-healing | Disseminated, progressive |
| Infectivity | Non-infectious | Highly infectious |
7. Immunity
- Cell-mediated immunity (CMI) is the key - Th1 response is protective
- Patients with tuberculoid leprosy have strong Th1 responses (IL-2, IFN-γ)
- Lepromatous patients have a specific defect in M. leprae CMI (not a global immunodeficiency)
- Lepromin test (Mitsuda reaction): intradermal injection of heat-killed M. leprae antigen
- Positive in tuberculoid, negative in lepromatous
- Tests cell-mediated immunity; not a diagnostic test (positive even in healthy uninfected individuals)
- No longer commercially available
8. Clinical Types (Ridley-Jopling Classification)
The disease exists as a spectrum based on host immune response:
TT -------- BT -------- BB -------- BL -------- LL
(Tuberculoid) (Borderline) (Lepromatous)
- TT (Tuberculoid): Localized; 1-5 well-defined macules/plaques with raised erythematous edges, dry-pale-hairless centers, anesthetic; few bacilli; non-infectious
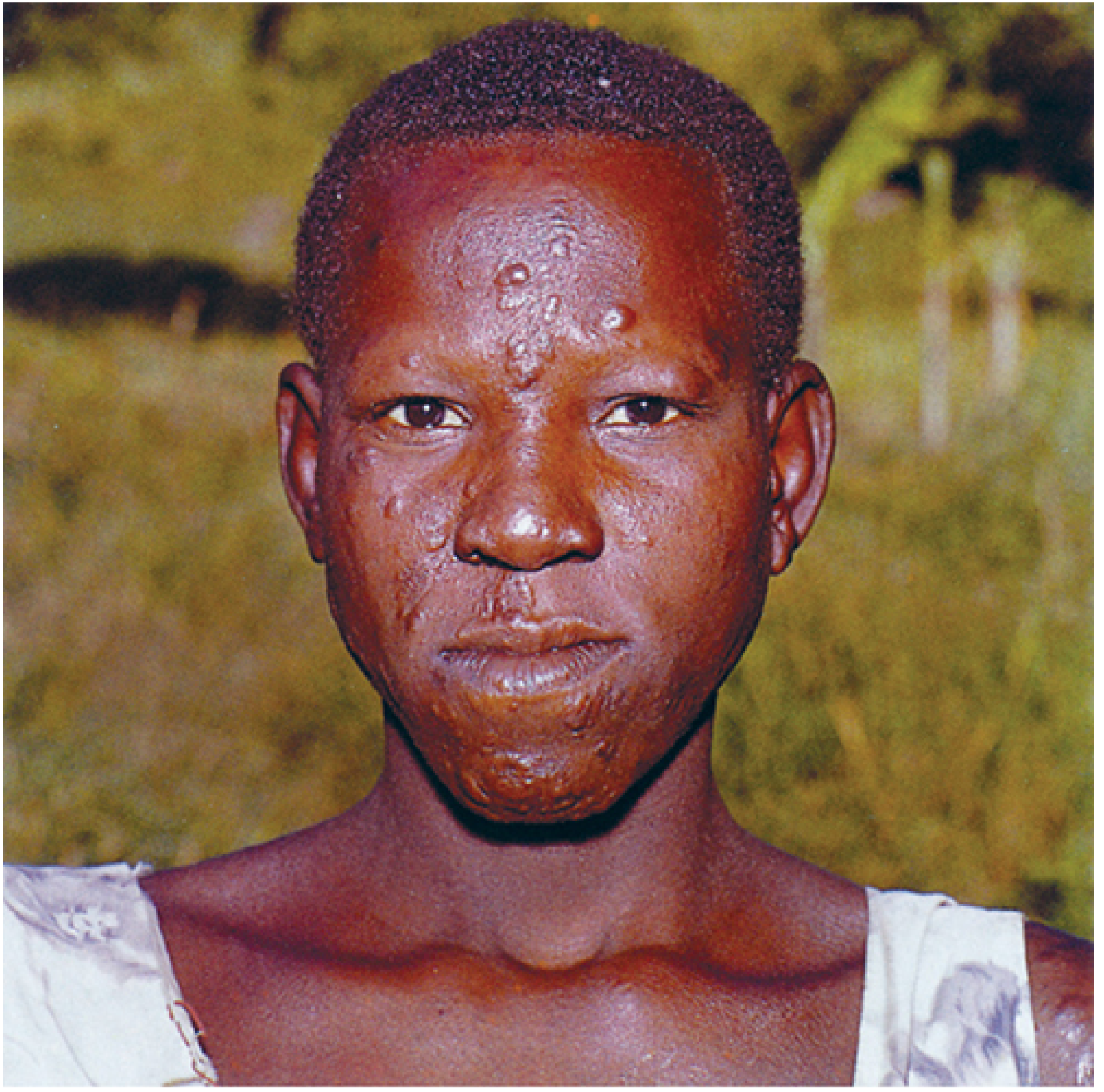
- LL (Lepromatous): Diffuse, bilateral symmetric infiltrative lesions; "leonine facies"; loss of eyebrows (madarosis); nasal collapse; claw fingers; testicular atrophy; highly infectious
- Borderline forms (BT, BB, BL): Intermediate features
WHO classification (operational):
- Paucibacillary (PB): <5 skin lesions (TT, BT)
- Multibacillary (MB): ≥6 skin lesions (BB, BL, LL)
3 Cardinal signs of leprosy:
- Hypopigmented/erythematous skin lesion with loss of sensation
- Thickened peripheral nerves
- AFB in slit-skin smear
9. Laboratory Diagnosis
A. Slit-Skin Smear (SSS)
- Sites: ear lobes, forehead, chin, active edge of lesion
- Stain with Fite stain (modified ZN; milder decolorizer - 1:1 xylene-peanut oil instead of acid-alcohol)
- Lepromatous: abundant AFB arranged in globi within macrophages
- Tuberculoid: very few or no AFB
B. Skin Biopsy (Full-thickness)
- Histology: noncaseating granulomas (tuberculoid) vs. foamy macrophages with many bacilli (lepromatous)
- Nerve involvement confirmed by biopsy
C. Nasal Smear
- Useful in lepromatous leprosy (large numbers of bacilli in nasal secretions)
D. Culture
- Not useful - cannot be cultured on artificial media
E. PCR
- Increasingly used as mainstay along with skin biopsy
- Detects M. leprae-specific DNA sequences
- Useful in paucibacillary disease where AFB are absent on smear
F. Serology
- Anti-PGL-1 IgM antibody: positive in ~95% of lepromatous, only ~30% of tuberculoid cases (due to poor humoral response in TT)
- Not useful for diagnosis alone
G. Lepromin Test (Mitsuda test)
- NOT a diagnostic test
- Used to classify disease (indicates CMI status) and determine prognosis
- Read at 48-72 hrs (Fernandez reaction - DTH) and 3-4 weeks (Mitsuda reaction - granuloma)
10. Treatment (WHO MDT Regimen)
| Regimen | Paucibacillary | Multibacillary |
|---|---|---|
| Drugs | Rifampicin + Dapsone | Rifampicin + Dapsone + Clofazimine |
| Duration | 6 months | 12 months |
| Rifampicin | 600 mg monthly (supervised) | 600 mg monthly (supervised) |
| Dapsone | 100 mg daily | 100 mg daily |
| Clofazimine | - | 300 mg monthly + 50 mg daily |
- Dapsone mechanism: blocks para-aminobenzoic acid (PABA) metabolism in M. leprae
- Rifampicin is the most bactericidal drug against M. leprae
11. Key Points Summary (Apurba-style mnemonics)
- M. leprae = Obligate intracellular, Non-culturable, Acid-fast, targets Schwann cells
- Only AFB that cannot be cultured on artificial media
- Fite stain for tissue (not standard ZN)
- Mouse footpad for drug susceptibility
- Armadillo = best animal model and natural reservoir outside humans
- PGL-1 = species-specific antigen (trisaccharide); used in serology
- Temperature optimum = 27-30°C → explains skin/nerve/testes involvement
- Lepromin test = tests CMI, NOT a diagnostic test
- Lepromatous = Multibacillary = Poor CMI = Infectious
- Tuberculoid = Paucibacillary = Good CMI = Non-infectious
Sources: Sherris & Ryan's Medical Microbiology 8e (p.1110-1114) | Medical Microbiology 9e (p.260) | Harrison's Principles of Internal Medicine 22e (Ch.184) | Quick Compendium of Clinical Pathology 5e (§3.6.5)
This is a shared conversation. Sign in to Orris to start your own chat.