Hey, Aris. What can you do for me? I am a... MD General Medicine. President in second year.
Hey! I'm Orris, your AI assistant. Great to meet a second-year MD General Medicine resident - here's what I can help you with:
What I Can Do For You
📚 Medical Knowledge & Learning
- Explain clinical concepts - pathophysiology, mechanisms, pharmacology, anatomy
- Case-based learning - work through clinical scenarios, differentials, management
- Drug information - mechanisms, interactions, dosing, side effects
- Exam prep - USMLE, NEET PG, DNB, or any postgrad entrance format
🔬 Evidence-Based Medicine
- PubMed literature search - find recent RCTs, meta-analyses, systematic reviews
- Guideline summaries - ACC/AHA, WHO, NICE, and others
- Journal article analysis - break down a paper's methods, results, and clinical relevance
🏥 Clinical Practice Support
- Differentials for a presenting complaint
- Interpretation of labs, ECGs, imaging findings (describe or upload)
- Management protocols for common GM conditions (sepsis, DKA, AKI, CHF, etc.)
- Procedures - understand indications, steps, complications
📄 Documents & Files
- Create presentations (PPTX) - case presentations, teaching rounds, seminars
- Word documents / reports - discharge summaries, research write-ups
- Excel/data analysis - if you have patient data or research data to crunch
🖼️ Images & Visuals
- Analyze uploaded images - ECGs, X-rays, histology slides, rashes - describe what you see
- Generate diagrams - flowcharts, clinical algorithms, study aids
As a second-year resident in General Medicine, you're likely dealing with ward rounds, call duties, case write-ups, and preparing for exams. I'm here for all of it - just ask! What would you like to start with?
Make easy learning of different characters of pulses
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Now I have everything I need. Let me put together a clear, easy-to-learn reference on pulse characters.
Characters of the Pulse - Easy Learning Guide
For a second-year MD GM resident - clinical mnemonics + mechanisms + causes, all in one place.
The 6 Things You Assess in Every Pulse
| Parameter | What It Tells You |
|---|---|
| Rate | Fast / slow |
| Rhythm | Regular / irregular |
| Volume | Pulse pressure (SBP - DBP) |
| Tension | Approximates diastolic BP |
| Character | Waveform shape = the bulk of this guide |
| Vessel wall | Atherosclerosis, calcification |
- S Das Manual on Clinical Surgery, p. 11
Pulse Waveform Diagrams (Harrison's, 22nd Ed.)
The image below shows the carotid pulse contour in different conditions - this is the single most important visual to memorize:
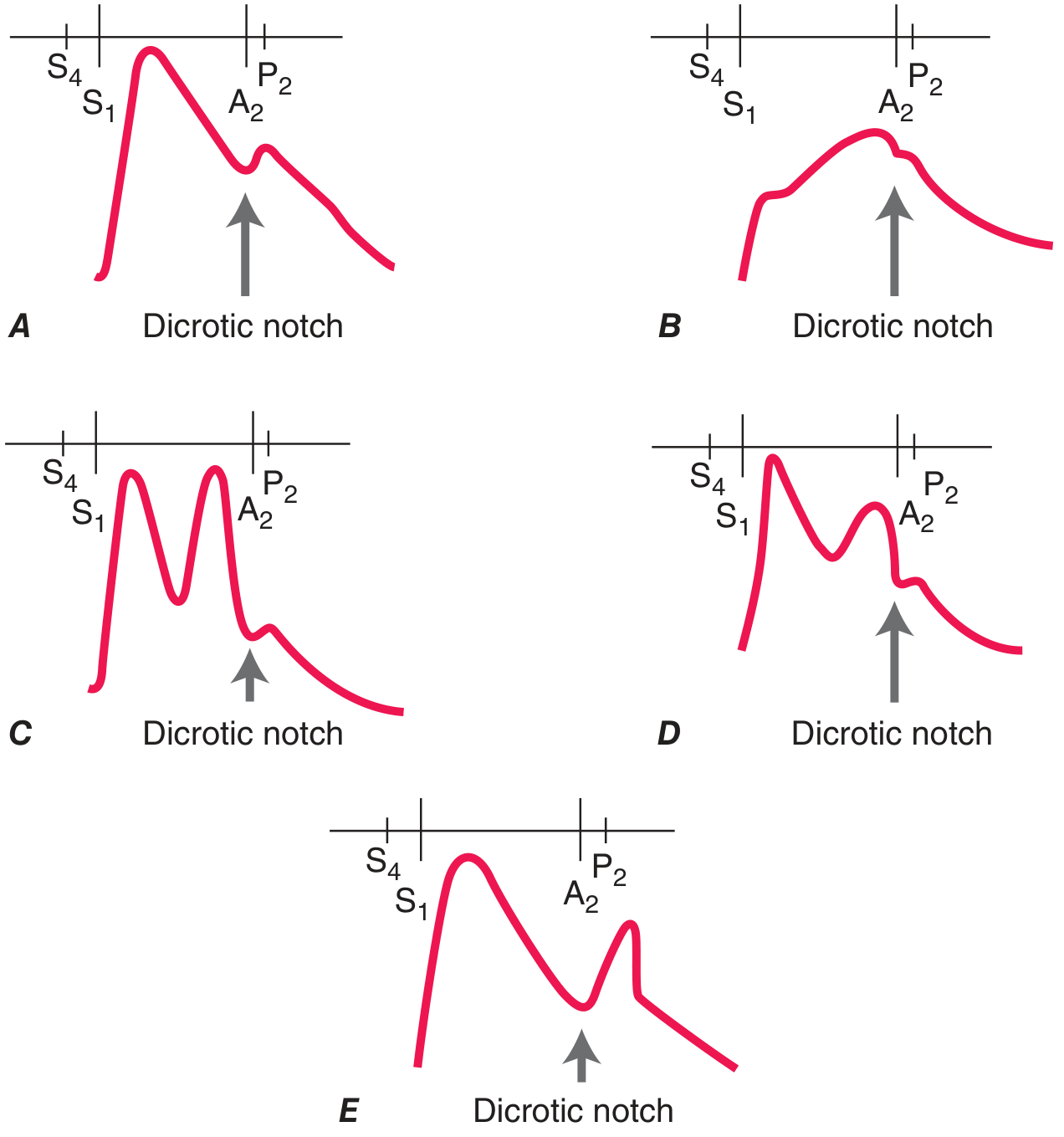
- A - Normal
- B - Aortic Stenosis: slow upstroke, small peak (parvus et tardus)
- C - Bisferiens: 2 systolic peaks (AR)
- D - Bisferiens/spike-and-dome: 2 peaks (HOCM)
- E - Dicrotic: one systolic peak + one diastolic peak (post-dicrotic notch)
All Named Pulse Characters - One by One
1. 🔴 Pulsus Parvus et Tardus
"Small and Late"
| Parvus | Reduced amplitude (narrow pulse pressure) |
| Tardus | Slow, delayed upstroke |
| Cause | Severe Aortic Stenosis (fixed LVOTO) |
| Feel | Like pushing through thick mud - slow rise, never peaks well |
| Mnemonic | "AS is PAST" - Parvus And Slow (Tardus) |
Also seen in subvalvular/supravalvular aortic stenosis. In HOCM (dynamic obstruction), upstroke is actually brisk initially.
- Fuster's The Heart, 15th Ed., p. 83
2. 🔴 Water-Hammer Pulse (Corrigan's Pulse)
"Bounding up, collapses fast"
| Feel | Sharp, forceful rise → rapid collapse; best felt by raising the arm |
| Cause | Severe Aortic Regurgitation (also thyrotoxicosis, high-output states) |
| Mechanism | Huge stroke volume (volume overload) + rapid diastolic run-off into LV |
| Mnemonic | "AR = A Rapid rise-and-fall" |
The pulse pressure is very wide (e.g., 160/40 mmHg). In severe AR, diastolic BP can approach 0 mmHg (Korotkoff sounds audible all the way down).
- Harrison's 22E, p. 1906; Fuster's The Heart, p. 83
3. 🔴 Bisferiens Pulse
"Two peaks in one beat"
| Peaks | Two palpable peaks within systole (double-humped) |
| Cause 1 | Severe AR (or mixed AS+AR with AR dominant) |
| Cause 2 | HOCM - spike-and-dome pattern (brisk early peak → mid-systolic obstruction → second peak) |
| Mnemonic | "Bis = Two" - BisFERIENS = Two peaks FERIOUS-ly in one beat |
Best felt at the carotid. In HOCM, the first peak is fast (percussion wave), second is slower (tidal wave).
- Harrison's 22E, p. 1906; Fuster's The Heart, p. 83
4. 🔴 Dicrotic Pulse
"One peak systole + one peak diastole"
| Peaks | First peak in systole, second peak after the dicrotic notch (early diastole) |
| Cause | Sepsis, dilated cardiomyopathy, severe peripheral vasoconstriction, IABP (balloon inflation) |
| Mechanism | Exaggeration of the normal dicrotic notch due to low SVR / poor cardiac output |
| Mnemonic | "DiCROTic = Di (two) + across the notCH" - peaks straddle the dicrotic notch |
- Harrison's 22E, p. 1906
5. 🔴 Anacrotic Pulse
"Notch on the way UP"
| Feel | A hesitation or notch on the ascending limb of the pulse |
| Cause | Severe Aortic Stenosis (especially severe fixed obstruction) |
| Mechanism | Turbulent, interrupted LV outflow due to stenotic valve |
| Mnemonic | "AnacrOTic = On Top of the upstroke" |
Anacrotic and parvus et tardus often co-exist in severe AS. Anacrotic notch + shoulder = the "anacrotism."
6. 🔴 Pulsus Paradoxus
"Falls too much on inspiration"
| Definition | SBP drops >10 mmHg with inspiration |
| Normal | SBP falls slightly (~5 mmHg) with inspiration - this is physiologic |
| Causes | Cardiac tamponade (most classic), massive PE, severe asthma/COPD, tension pneumothorax, hemorrhagic shock |
| Mechanism | Exaggerated interventricular dependence - inspiratory RV expansion compresses LV, reducing LV output |
| How to measure | Deflate BP cuff slowly - note pressure where sounds first appear (expiration only) vs. where heard in ALL phases → difference >10 mmHg = positive |
| Mnemonic | "TAPE" - Tamponade, Asthma/COPD, PE, Emergency (tension pneumothorax) |
- Harrison's 22E, p. 1906
7. 🔴 Pulsus Alternans
"Big beat, small beat, big beat, small beat..."
| Definition | Beat-to-beat alternation in pulse amplitude (not rhythm - rhythm stays regular) |
| Cause | Severe LV systolic dysfunction (low EF heart failure) |
| Mechanism | Alternating end-diastolic fiber lengths due to impaired Frank-Starling mechanism |
| Key distinction | NOT respirophasic (unlike pulsus paradoxus which changes with breathing) |
| Mnemonic | "AlterNAnS = Never the Same beat twice" |
Ominous sign - indicates very profound ventricular dysfunction.
- Harrison's 22E, p. 1096; Fuster's The Heart, p. 83
Quick Summary Table
| Pulse | Waveform | Classic Cause | Key Memory Hook |
|---|---|---|---|
| Parvus et Tardus | Small + slow upstroke | Aortic Stenosis | AS is PAST |
| Water-Hammer | Bounding + rapid collapse | Aortic Regurgitation | AR = A Rapid fall |
| Bisferiens | 2 peaks in systole | AR / HOCM | Bis = Two |
| Anacrotic | Notch on upstroke | Severe AS | On top of upstroke |
| Dicrotic | 1 systolic + 1 diastolic peak | Sepsis / DCM / IABP | Straddles the notch |
| Pulsus Paradoxus | Drops >10 mmHg on inspiration | Tamponade | TAPE mnemonic |
| Pulsus Alternans | Big-small-big-small amplitude | Severe LV dysfunction | Never same twice |
Clinical Exam Tips
- Best site for pulse character: Carotid artery (closest to aortic root, least distorted)
- Pulsus paradoxus: measured at brachial artery with sphygmomanometer
- Water-hammer: accentuated by raising the arm above the heart
- Pulsus alternans: can be subtle - slow cuff deflation unmasks it
Sources: Harrison's Principles of Internal Medicine 22E (2025), Fuster's The Heart 15th Ed., S Das Manual on Clinical Surgery 13th Ed.
Ausculatatory gap
Finding Sources
Reading File
Reading File
Reading File
Got everything I need. Here's the complete, easy-to-learn breakdown:
Auscultatory Gap
What Is It?
During BP measurement by auscultation, Korotkoff sounds disappear for a range of pressures between systolic and diastolic, then reappear again at a lower pressure - this silent interval is the auscultatory gap.
Cuff pressure falling ↓
180 mmHg → Korotkoff sounds APPEAR ← True Systolic (Phase I)
170 mmHg → Sounds present
160 mmHg → Sounds DISAPPEAR ┐
150 mmHg → Silence │ ← AUSCULTATORY GAP (e.g., 25 mmHg wide)
140 mmHg → Silence │
135 mmHg → Sounds REAPPEAR ┘
...
80 mmHg → Sounds disappear ← True Diastolic (Phase V)
Why It Matters - The Two Errors It Causes
| Error | How It Happens | Result |
|---|---|---|
| Underestimate SBP | Clinician starts auscultating too low (below the gap); first sounds heard = re-appearance, not true Phase I | Records falsely LOW systolic BP |
| Overestimate DBP | Clinician mistakes the gap as diastole; stops recording when sounds disappear for the first time | Records falsely HIGH diastolic BP |
The gap may account for up to a 25 mmHg discrepancy between true and measured SBP. - Washington Manual of Medical Therapeutics
Classic Associations
| Associated Condition | Why |
|---|---|
| Systemic hypertension | Most classic association |
| Atherosclerosis / arterial stiffness | Altered vessel wall compliance changes how turbulence (Korotkoff sounds) is generated |
| Older patients | Common due to noncompliant, stiff arteries |
| Severe aortic stenosis | Also described |
"The auscultatory gap is found in patients with systolic hypertension and is usually an indication of arterial stiffness." - Swanson's Family Medicine Review
Mechanism (Why Does the Gap Occur?)
The exact mechanism is not fully settled, but the leading explanation:
- Korotkoff sounds require turbulent flow under the cuff
- In stiff, atherosclerotic vessels - as cuff pressure drops through a certain range, there is a transitional phase where flow is neither fully turbulent nor laminar, generating sounds too faint to hear
- Below that range, turbulence resumes → sounds reappear
- Essentially: abnormal vessel compliance disrupts the smooth transition from occluded to open flow
How to AVOID Missing It - Two Methods
✅ Method 1: Palpatory Estimation Before Auscultation (Best practice)
- Palpate the radial pulse while inflating the cuff
- Note the pressure at which the radial pulse disappears → this is the estimated systolic
- Inflate the cuff 20-30 mmHg above this level
- Now auscultate - you start above the true systolic, so you won't miss Phase I even if a gap is present
"Palpation of the radial artery, while the cuff is inflated, prevents underestimation of blood pressure." - Fuster's The Heart, 15th Ed.
✅ Method 2: Simultaneous Radial Palpation During Deflation
- While deflating and auscultating, simultaneously palpate the radial pulse
- The radial pulse reappears at true systolic pressure, even if Korotkoff sounds are in the gap
- If you feel the pulse but hear nothing → you're inside the gap, keep deflating slowly
Quick Recall Card
AUSCULTATORY GAP
├── What: Silent zone between Phase I and II of Korotkoff sounds
├── Who: Hypertensives, elderly, atherosclerosis (stiff arteries)
├── Error 1: Underestimate SYSTOLIC (start too low → miss Phase I)
├── Error 2: Overestimate DIASTOLIC (stop at gap, not true Phase V)
├── Gap size: Can be up to 25 mmHg
└── Fix: Palpate radial first → inflate 30 mmHg above palpated systolic
Exam Tip
If a MCQ asks:
- "Auscultatory gap leads to underestimation of..." → Systolic BP ✓
- "Best way to avoid auscultatory gap error..." → Palpatory method first ✓
- "Auscultatory gap is a sign of..." → Arterial stiffness / hypertension ✓
Sources: Washington Manual of Medical Therapeutics; Fuster's The Heart 15th Ed.; Morgan & Mikhail's Clinical Anesthesiology 7th Ed.; Swanson's Family Medicine Review
This is a shared conversation. Sign in to Orris to start your own chat.