Clavicle fracture - tens nail approach
Reading File
Finding Sources
Finding Sources
Searching PubMed
clavicle fracture intramedullary nail TENS fixation
Reading File
Reading File
Searching PubMed
clavicle fracture intramedullary nail plate fixation
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a comprehensive answer. Here is the full write-up:
Clavicle Fracture - TENS Nail (Titanium Elastic Nail) Approach
What is TENS Nailing?
The Titanium Elastic Nail (TEN), also called Elastic Stable Intramedullary Nailing (ESIN), is a minimally invasive intramedullary (IM) fixation technique for displaced midshaft clavicle fractures. The nail is a small-diameter, smooth, flexible titanium rod inserted in either antegrade (anteromedial entry) or retrograde (posterolateral entry) fashion through the clavicular medullary canal.
Indications
TEN nailing is best suited for:
- Acute displaced midshaft clavicle fractures - simple transverse or short oblique patterns
- Patients who want a cosmetically superior, smaller incision
- Cases where hardware prominence from plate fixation is a concern
- Patients where shorter operative time and less blood loss are priorities
Contraindications / poor candidates:
- Comminuted fractures (unlocked TEN cannot maintain length or rotation in these)
- Very narrow or irregular medullary canal (preoperative canal sizing is mandatory)
- Older/delayed fractures (>2-3 weeks) - closed reduction becomes difficult; open reduction must be anticipated
Preoperative Planning
| Parameter | Detail |
|---|---|
| Table | Radiolucent or shoulder table |
| Position | Semisitting, small pad between scapulae |
| C-arm | Contralateral side (can also be ipsilateral or cranial) |
| Equipment | Appropriate IM pin + accompanying drill or awl; reduction clamps |
| Special note | Select nail diameter to match the IM canal size; closed reduction more difficult in older fractures - anticipate open reduction |
Pre-op imaging should confirm:
- Canal caliber adequate for intended device
- Fracture pattern suitable for unlocked device (simple patterns only unless a locking device is used)
Surgical Technique
Patient Positioning
- Semisitting (beach-chair) position on a radiolucent table
- Small pad placed between scapulae - allows the shoulder to "fall back," counteracting the typical shoulder protraction deformity
- Image intensifier on the contralateral side; rotating 45° caudal and 45° cephalad gives orthogonal views of the clavicle
- Head turned to the opposite side and taped
- Arm may be free-draped if difficult reduction is anticipated (e.g., significant shortening)
Key Surgical Steps
- Confirm complete fluoroscopic visualization of the entire clavicle before draping
- Entry site creation:
- Retrograde insertion: small posterolateral incision at the lateral clavicle
- Antegrade insertion: small anteromedial incision near the sternoclavicular joint
- An entry portal is made with a drill or awl
- Pass the nail through the near fragment - the nail is introduced into the medullary canal of the clavicle fragment on the entry side
- Reaming (if required by nail diameter)
- Fracture reduction - percutaneously or through a small open incision at the fracture site
- Nail passage across the fracture under fluoroscopy - guided into the far fragment and seated securely
- Alignment check - clinically and radiographically confirm correct length, alignment, and rotation
- Nail trimming / locking:
- If unlocked device: cut nail flush with the insertion surface, close incisions
- If locking device: perform locking, then close
Intramedullary fixation technique - Rockwood & Green's Fractures in Adults, 10th ed. (2025)
Advantages Over Plate Fixation
| Feature | TEN Nail | Plate Fixation |
|---|---|---|
| Incision | Small, cosmetically superior | Longer incision |
| Soft tissue stripping | Minimal - fracture hematoma preserved | More extensive |
| Hardware prominence | Lower | Higher (plate bulk) |
| Hardware removal | Technically simple (often under local) | More involved |
| Refracture at implant end | Lower theoretical risk | Small but real risk |
| Op time / blood loss | Shorter / less | More |
| Rotational/axial control | Poor (unlocked) / Good (locked) | Excellent |
Pitfalls and Complications
| Complication | Prevention |
|---|---|
| Inability to pass IM nail | Careful preoperative canal sizing |
| Iatrogenic fracture comminution | Avoid using the nail as a joystick; do not force |
| Neurovascular injury | Keep instrumentation anterior/superior; avoid posterior-inferior passage |
| Peri-incisional numbness | Preserve supraclavicular nerve branches (especially with open reduction) |
| Early hardware failure | Match device size to fracture type and patient activity |
| Malunion / shortening | Avoid IM fixation in comminuted fractures; consider locking devices |
| High hardware removal rate | Use a locking device (reduces migration and symptomatic prominence) |
| Migration | A well-known issue with smooth TENs; locking nails greatly reduce this |
Outcomes - What the Evidence Shows
From Rockwood & Green's Fractures in Adults (10th ed., 2025):
- Van der Meijden et al. RCT (n=120): TEN vs. compression plate - both achieved excellent results at 1 year (mean Constant scores 95-96); however, the plate group had less early disability (up to 6 months). Hardware removal was recommended for all TEN patients vs. only 1 patient in the plate group.
- Hoogervoerst et al. meta-analysis: Overall hardware removal rate for TENs ~20%, Rockwood/Hagie pins ~22% - lower than often reported in older series.
- Overall: Recent studies report IM nailing outcomes similar to plate fixation for low nonunion rates and functional scores, with potential benefits of shorter operative time, less blood loss, and better cosmesis.
- Important caveat: A meta-analysis of 895 patients reported better functional outcomes after IM nailing vs. plates, but sensitivity analysis showed this was solely driven by locking IM nails - not unlocked TENs.
- Comminuted fractures: Fuglesang found in subgroup analysis that functional recovery after ESIN was significantly slower in comminuted fractures vs. simple patterns.
Bottom line (Rockwood & Green's): "For simple pattern fractures, with an accommodating IM canal, elastic titanium nailing is a reasonable option, with the expectation that hardware removal will be required once healing ensues." Locking IM nails, by maintaining length and reducing migration, are emerging as a more competitive alternative to plate fixation. - Rockwood and Green's Fractures in Adults, 10th ed. 2025
Key Takeaways
- TEN/ESIN is a minimally invasive, cosmetically appealing option for simple midshaft clavicle fractures
- Patient selection is critical - avoid comminuted or unstable fractures with unlocked devices
- Hardware removal is expected with unlocked TENs and should be discussed preoperatively
- Locking IM nails represent the next evolution - better axial/rotational control, lower removal rates, broader fracture applicability
- Operate within 2-3 weeks of injury when possible; delayed fixation raises the risk of brachial plexus tethering to the inferior clavicle surface
Approach to clavicle
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have everything needed for a thorough, well-illustrated answer on the surgical approach to the clavicle.
Surgical Approach to the Clavicle
Overview
The clavicle is a subcutaneous bone, making it one of the more accessible bones in the body. However, its proximity to critical neurovascular structures (subclavian vessels, brachial plexus, lung apex) demands careful, layered dissection. The approach is used for:
- Open reduction and internal fixation (ORIF) of midshaft fractures
- Lateral (distal) clavicle fracture fixation
- Excision of the medial or lateral ends (e.g., AC joint arthroplasty)
- Pseudarthrosis repair
Relevant Anatomy
Structures at Risk
| Structure | Location | Danger |
|---|---|---|
| Supraclavicular nerves (medial, intermediate, lateral branches of C3/C4) | Cross the superior/anterior surface of the clavicle | Cutaneous numbness inferior to the incision if divided |
| Subclavian vein | Immediately posterior-inferior to the medial clavicle | Catastrophic hemorrhage |
| Subclavian artery / brachial plexus | Posterior-inferior, slightly lateral | Neurovascular injury with deep inferior drilling or plunging |
| Lung apex / pleura | Inferior to the clavicle medially | Pneumothorax with drill plunge |
| Cephalic vein | Deltopectoral groove laterally | Rarely at risk |
Key Layers (Superficial to Deep)
- Skin
- Subcutaneous fat
- Platysma muscle (fuses with superficial fascia over the clavicle region)
- Supraclavicular nerves
- Clavipectoral fascia / periosteum
- Clavicle bone
Patient Positioning
- Supine with a large roll/bump between the scapulae - allows the injured shoulder girdle to fall posteriorly, restoring length and improving exposure
- Head turned slightly to the contralateral side
- Semi-beach-chair position (20-30°) is also acceptable, particularly for combined procedures
- Arm is draped free if reduction is anticipated to be difficult
- Fluoroscopy: C-arm contralateral side; rotating 45° caudal and 45° cephalad provides orthogonal views of the S-shaped clavicle
Incision
Standard oblique (Langer's line) incision:
- Centered directly over the fracture or pathology, paralleling the superior border of the clavicle
- For midshaft fractures: typically 5-8 cm, angled slightly obliquely in skin tension lines (cosmetically superior)
- An alternative vertical incision is also acceptable
- For the full clavicle: incision from the sternal notch to the anterior edge of the acromion
The clavicle is subcutaneous - the skin incision directly overlies the bone. A longer but lower cosmetic scar (Langer's line) heals better than a transverse incision placed too medially.
Layer-by-Layer Dissection
Layer 1 - Skin and Platysma
- Incise skin and subcutaneous fat
- The platysma is encountered as a thin muscular layer; separate it from the overlying skin and split its fibers in line with the muscle
- The skin and platysma/subcutaneous layer should be mobilized and elevated together as one composite layer - kept together to maximize coverage over the plate at closure
Layer 2 - Supraclavicular Nerves
- Branches of the supraclavicular nerve (C3/C4) cross the superior and anterior surface of the clavicle
- Isolate and protect any visible, larger branches if possible
- Smaller branches crossing the operative field may require division
- Warn patients preoperatively about the likely area of numbness inferior to the incision - this typically improves with time but may be permanent in some cases
Layer 3 - Clavipectoral Fascia / Periosteum
- Incise the clavipectoral fascia along its attachment to the anterior clavicle
- Carefully elevate it inferiorly - this exposes the anterior clavicle surface
- The myofascial layer over the clavicle is incised and elevated as one continuous layer - this creates a second distinct layer for two-layer wound closure at the end
- Preserve soft tissue attachments to major fragments (especially butterfly fragments) - do NOT completely denude fragments of periosteum, as this devascularizes them
Layer 4 - Fracture Site
- Dissect first along the medial and lateral aspects of the fracture
- Debride fracture edges of periosteum and hematoma
- Identify the main fracture line and all major fragments
- Formulate fixation strategy before any further bone handling
Key Surgical Steps - ORIF (Plate Fixation)
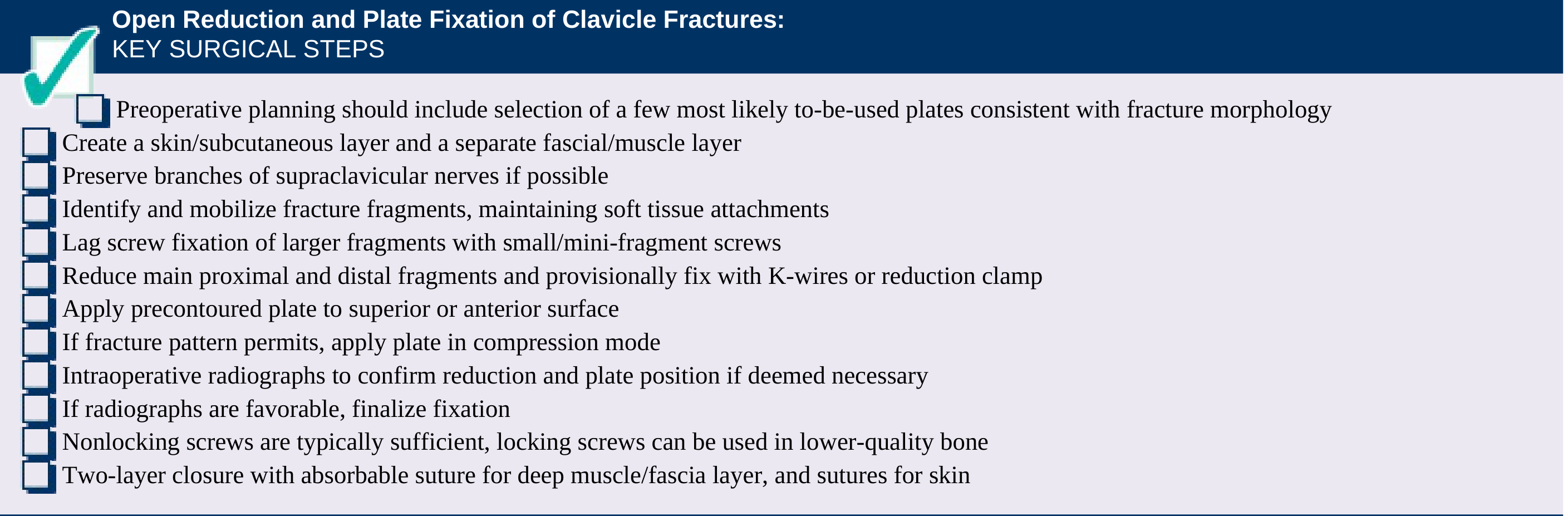
Open Reduction and Plate Fixation: Key Surgical Steps - Rockwood & Green's Fractures in Adults, 10th ed. (2025)
- Create two distinct layers: skin/subcutaneous and fascial/muscle
- Preserve branches of supraclavicular nerves where possible
- Identify and mobilize fracture fragments, maintaining soft tissue attachments
- Lag screw fixation of any large free fragment (≥1/3 clavicle circumference) to simplify the fracture to a two-part pattern - use 2.4 mm or 2.7 mm minifragmentary screws
- Reduce main proximal and distal fragments with reduction forceps; provisionally fix with K-wire or lag screw
- Apply precontoured plate to superior or anteroinferior surface
- If fracture pattern permits, apply plate in compression mode; if comminuted, apply in neutral/bridging mode
- Screw fixation: minimum 3 bicortical screws (6 cortices) each side of the fracture if a lag screw has been placed; 4 screws each side if no lag screw
- Intraoperative fluoroscopy to confirm reduction and plate position
- If any concern about pleural violation: Valsalva maneuver to detect air leak
- Two-layer closure: deep muscle/fascia layer with absorbable sutures, then skin
Plate Positioning Options
Superior Plating (Most Common)
- Plate sits on top of the clavicle
- Familiar approach, easily extended medially and laterally
- Clear postoperative radiographic views
- Disadvantage: screws directed inferior - risk of drill plunge into subclavian vessels, pleura
- Screw lengths typically 14-16 mm (females) to 16-18 mm (males) given narrow superoinferior dimension
- Medially: avoid plunging posteriorly into the subclavian/pleura
- Laterally: avoid screws that protrude into the subacromial space, irritating the rotator cuff
Anteroinferior Plating (Collinge Technique)
- Plate applied to the anteroinferior surface
- Screws directed posteriorly and superiorly - safer trajectory away from the pleura
- Better biomechanical position (tension side)
- Requires more careful dissection of clavipectoral fascia inferiorly
- Minifragmentary plates (2.7 mm) used
Dual Plating
- Superior 2.4 mm + anteroinferior 2.7 mm plate
- Reserved for complex or comminuted fractures requiring additional stability
Dangers by Surgical Step
| Step | Hazard | Avoidance |
|---|---|---|
| Skin incision | Supraclavicular nerve branches | Identify and protect; counsel patient preoperatively |
| Inferior dissection, medial third | Subclavian vein injury | Stay on bone surface; limit retraction depth |
| Drilling superiorly → inferiorly | Lung apex / pleura puncture | Use drill guides; limit drill depth; Valsalva test if concerned |
| Drilling inferiorly, medial | Subclavian vessels / brachial plexus | Maintain periosteal plane; never drive drill freehand medially |
| Lateral screw placement | Rotator cuff irritation (subacromial) | Confirm screw length intraoperatively |
| Periosteal stripping of fragments | Devascularization, non-union | Preserve soft tissue on all fragments |
Wound Closure
- Layer 1 (deep): Myofascial/clavipectoral fascial layer closed with absorbable sutures - provides direct plate coverage
- Layer 2 (superficial): Skin/subcutaneous layer closed with sutures or staples
- Two-layer closure is mandatory; single-layer closure risks wound breakdown over the plate and hardware prominence/exposure
Postoperative Care
- Arm in a sling for comfort (typically 4-6 weeks)
- Pendulum and Codman exercises started early
- Avoid heavy lifting, pushing, or pulling
- Full return to activities when fracture union is confirmed radiographically (typically ~2 months for simple patterns)
Sources: Rockwood and Green's Fractures in Adults, 10th ed. (2025); Campbell's Operative Orthopaedics, 15th ed. (2026)
Clavicle anatomy
Finding Sources
Finding Sources
Reading File
Loading Image
I have all the content needed. Here is the complete anatomy of the clavicle:
Anatomy of the Clavicle
Bony Anatomy
The clavicle is the only true bony connection between the torso and the arm. It acts as a strut, transmitting forces between the upper limb and the axial skeleton.
Ossification - Unique Features
- First bone to ossify in the body - begins by intramembranous ossification at 5-6 weeks of gestation
- Last bone to reach complete ossification - the medial physis (epiphysis) does not fuse until approximately 27 years of age
- This late fusion is clinically important: what appears as a medial clavicle fracture-dislocation in adolescents and young adults is often a physeal injury (Salter-Harris fracture), not a true dislocation
Shape and Curvature
The clavicle has a characteristic S-shape produced by two curves:
- Primary (coronal) curve - the dominant S-curve visible from above:
- Medial two-thirds: convex anteriorly (curves forward)
- Lateral third: concave anteriorly (curves backward)
- Secondary (superior) curve - a subtle superior bow:
- Apex located laterally, approximately 37 mm from the acromial articulation
- Mean magnitude of only 5 mm
- The medial superior surface is flat
Smaller clavicles have more pronounced curves; larger individuals have longer, less curved clavicles. There are significant sex and racial differences in clavicle shape, which explains why even "pre-contoured" anatomic plates frequently require intraoperative adjustment for optimal fit.
Cross-sectional Anatomy
Cross-sectional and topographic anatomy of the clavicle. Note how the bone is narrowest in its midportion - explaining the high incidence of fractures in this region. - Rockwood & Green's Fractures in Adults, 10th ed. (2025)
| Region | Shape | Medullary Canal |
|---|---|---|
| Medial end | Wide, rounded / prismatic | Large, triangular |
| Midshaft | Narrowest, cylindrical / tubular | Smallest diameter - most fractures occur here |
| Lateral end | Flat, wide | Flattened, broad |
The midshaft narrowing is the key reason why approximately 80% of clavicle fractures occur in the middle third.
Ligamentous Anatomy
Medial - Sternoclavicular (SC) Joint
- The SC joint has relatively little motion but is inherently stable due to strong soft tissue constraints
- Posterior SC capsule - the single most important soft tissue constraint resisting anterior and posterior translation of the medial clavicle
- Interclavicular ligament - runs from the medial end of one clavicle, across the superior sternum (sternal notch), to the contralateral medial clavicle; acts as a tension wire preventing inferior angulation/translation
- Costoclavicular ligament (rhomboid ligament) - extremely stout ligaments from the first rib to the inferior clavicle; attaches at the rhomboid fossa (a small depression on the inferior medial clavicle); primarily resists inferior translation of the medial clavicle
Lateral - Acromioclavicular (AC) Joint
The lateral clavicle is stabilized by two distinct ligament groups:
1. AC Ligaments (direct joint stabilizers)
- Superior and inferior AC capsular ligaments - primary restraints to anteroposterior (horizontal) translation
- Reinforce the AC joint capsule directly
2. Coracoclavicular (CC) Ligaments (primary vertical stabilizers)
These are the main suspension ligaments holding the shoulder girdle up to the clavicle:
| Ligament | Position | Function |
|---|---|---|
| Trapezoid ligament | More lateral, horizontal fibers | Resists axial (compressive) loading and lateral displacement |
| Conoid ligament | More medial and posterior, vertical/oblique fibers | Primary restraint to superior translation of the clavicle (or inferior displacement of the shoulder) |
The CC ligament interval (between the two limbs of the CC complex) is ~8 mm. This space is important in distal clavicle fracture classification (Neer type II) - fractures medial to the CC ligaments are unstable because the medial fragment has no ligamentous attachment to the scapula/shoulder.
Muscular Anatomy
The deforming forces on a clavicle fracture are determined by the muscles attached to each fragment:
Muscles Attached to the Clavicle
| Muscle | Attachment | Action on Fracture |
|---|---|---|
| Sternocleidomastoid (SCM) | Superior medial clavicle | Pulls medial fragment superiorly and posteriorly |
| Pectoralis major | Inferior medial/anterior clavicle | Pulls lateral/distal fragment inferiorly and anteriorly |
| Deltoid | Lateral clavicle (anterior border) | Pulls lateral fragment inferiorly |
| Trapezius | Lateral clavicle (posterior border) | Pulls lateral fragment superiorly and posteriorly |
| Subclavius | Inferior surface, groove of middle third | Minor depressor; acts as a protective buffer for the subclavian vessels |
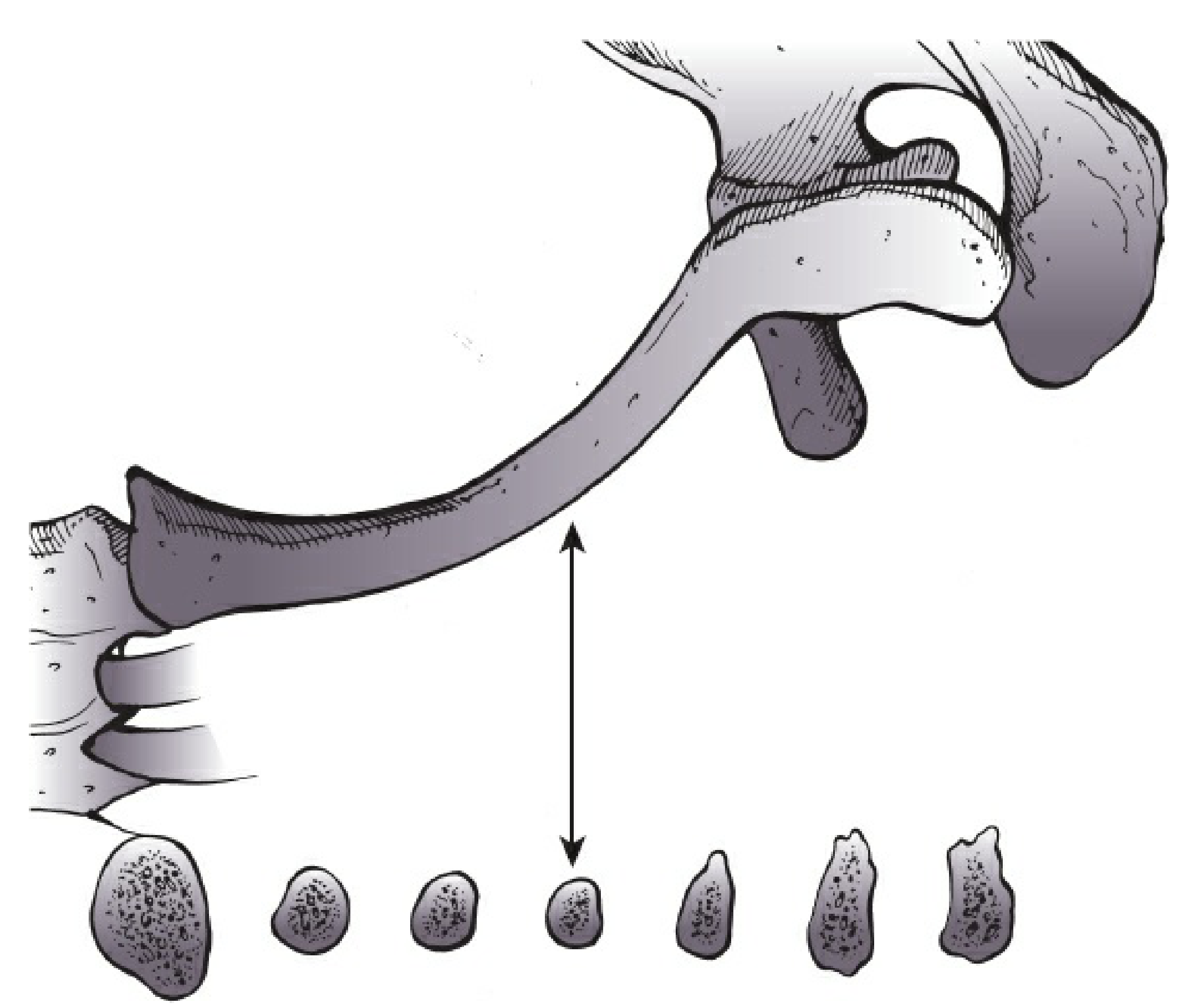
Typical Fracture Deformity (Midshaft)
- Medial fragment: elevated and retracted posteriorly by SCM
- Lateral fragment (with shoulder): displaced inferiorly, anteriorly, and medially by the weight of the arm + pectoralis major + deltoid pull
- Net result: shortening and the typical "drooping shoulder" deformity
Neurovascular Anatomy
Structures Posterior/Inferior to the Clavicle
These lie in the subclavicular space directly posterior and inferior to the bone, making inferior drill penetration potentially catastrophic:
| Structure | Relationship |
|---|---|
| Subclavian vein | Immediately posterior-inferior to the medial clavicle; crosses the first rib at the lateral border of the first rib |
| Subclavian artery | Lies posterior to the vein, slightly more lateral; separated from the vein by the anterior scalene muscle |
| Brachial plexus | Lateral to the subclavian artery; trunks pass between the anterior and middle scalene muscles |
| Lung apex / pleura | Rises above the first rib into the neck; lies inferior to the medial clavicle |
Supraclavicular Nerves (Surgical Relevance)
- Branches of the cervical plexus (C3/C4)
- Three branches: medial, intermediate, and lateral supraclavicular nerves
- Cross the superior and anterior surface of the clavicle, travelling inferiorly to supply the skin of the shoulder, upper chest, and deltoid region
- Routinely at risk during any surgical approach to the clavicle
- Division causes numbness inferior to the scar - usually improves but may be permanent
- Larger branches should be identified and protected where possible during ORIF
Nutrient Artery
- The clavicle's blood supply enters via a nutrient foramen on the inferior surface of the midshaft
- Extensive periosteal stripping during fixation devascularizes fragments and increases non-union risk
Summary: Why the Midshaft is Most Vulnerable
- Narrowest cross-section - least bone stock
- No muscular protection - the subclavius only covers part of the inferior surface
- Deforming muscle forces pull the fragments in opposite directions
- Lever arm effect - the clavicle acts as a strut; bending forces concentrate at the weakest (narrowest) point
- Single nutrient artery entry zone - midshaft stripping can compromise vascularity
Source: Rockwood and Green's Fractures in Adults, 10th ed. (2025)
Tens clavicle approach
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
I now have the complete detailed technique from both Campbell's and Rockwood & Green's. Here is the full surgical approach:
TENS Nail - Surgical Approach to the Clavicle
Device Overview
The Titanium Elastic Nail (TEN) / Elastic Stable Intramedullary Nail (ESIN) is a smooth, flexible nail inserted through the medullary canal of the clavicle. The nail can be inserted in two directions:
| Approach | Entry Site | Direction of Insertion |
|---|---|---|
| Retrograde (most common) | Posterolateral clavicle, 2-3 cm medial to AC joint | Nail driven medially across the fracture |
| Antegrade | Anteromedial clavicle, near sternoclavicular joint | Nail driven laterally across the fracture |
The retrograde approach is the standard technique and is described in detail below (Campbell's Operative Orthopaedics Technique 62.2).
Setup and Positioning
- Table: Radiolucent or shoulder table
- Position: Semi-seated (beach-chair), ~20-30° upright
- Pad: Small roll between scapulae - lets the shoulder fall back, counteracting the typical protraction deformity and aiding reduction
- Head: Turned to the contralateral side, taped in place
- Image intensifier: Ipsilateral or contralateral side; rotating 45° caudal and 45° cephalad obtains orthogonal views of the S-shaped clavicle
- Arm: Standard draping; may be draped free if a difficult reduction is anticipated
Incision and Approach (Retrograde)
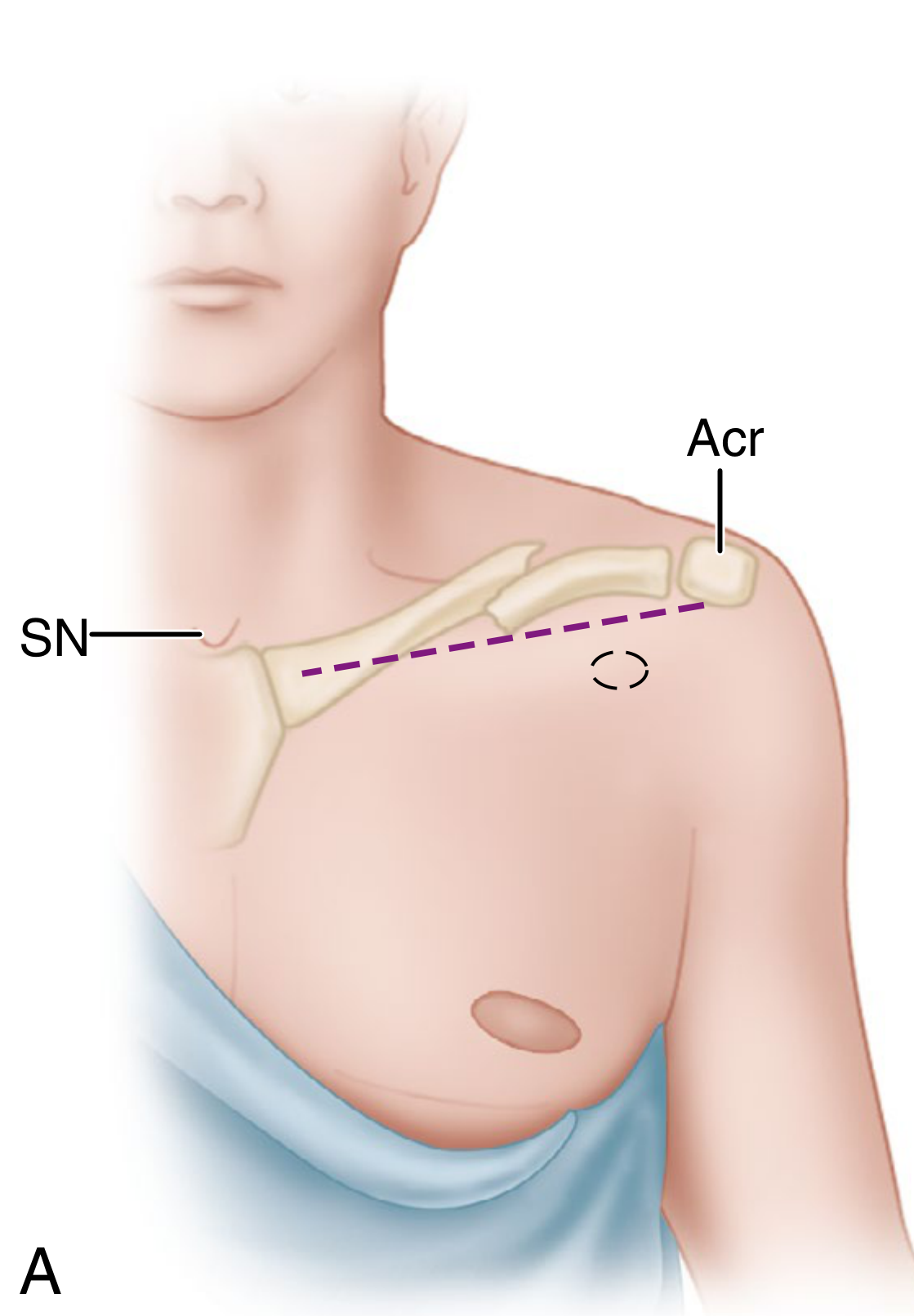
Incision planning for intramedullary fixation. The dashed line shows the clavicle axis from the sternal notch (SN) to the acromion (Acr). The circle marks the posterolateral entry portal - Campbell's Operative Orthopaedics, 15th ed. (2026)
Step 1 - Incision
- Make a 2-3 cm incision over the posterolateral corner of the clavicle, 2-3 cm medial to the AC joint
- Little subcutaneous fat in this region - take care immediately on incising the skin
Step 2 - Platysma
- Use scissors to free the platysma from the overlying skin; split its fibers in line with the muscle (not across)
- The middle branch of the supraclavicular nerve is usually found directly beneath the platysma muscle near the midclavicle - identify and retract it; do not divide it
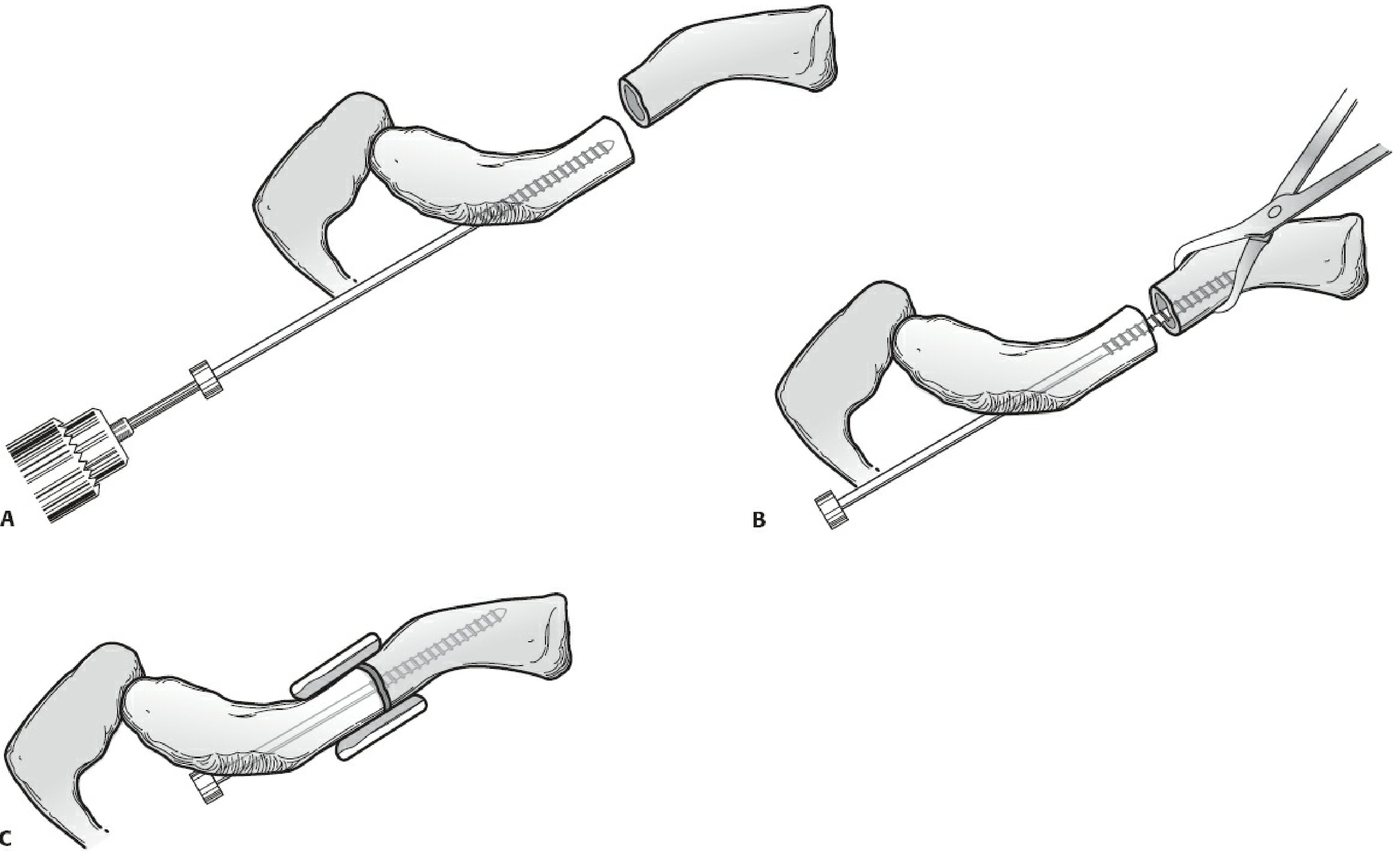
Step-by-Step Nail Insertion (Retrograde)
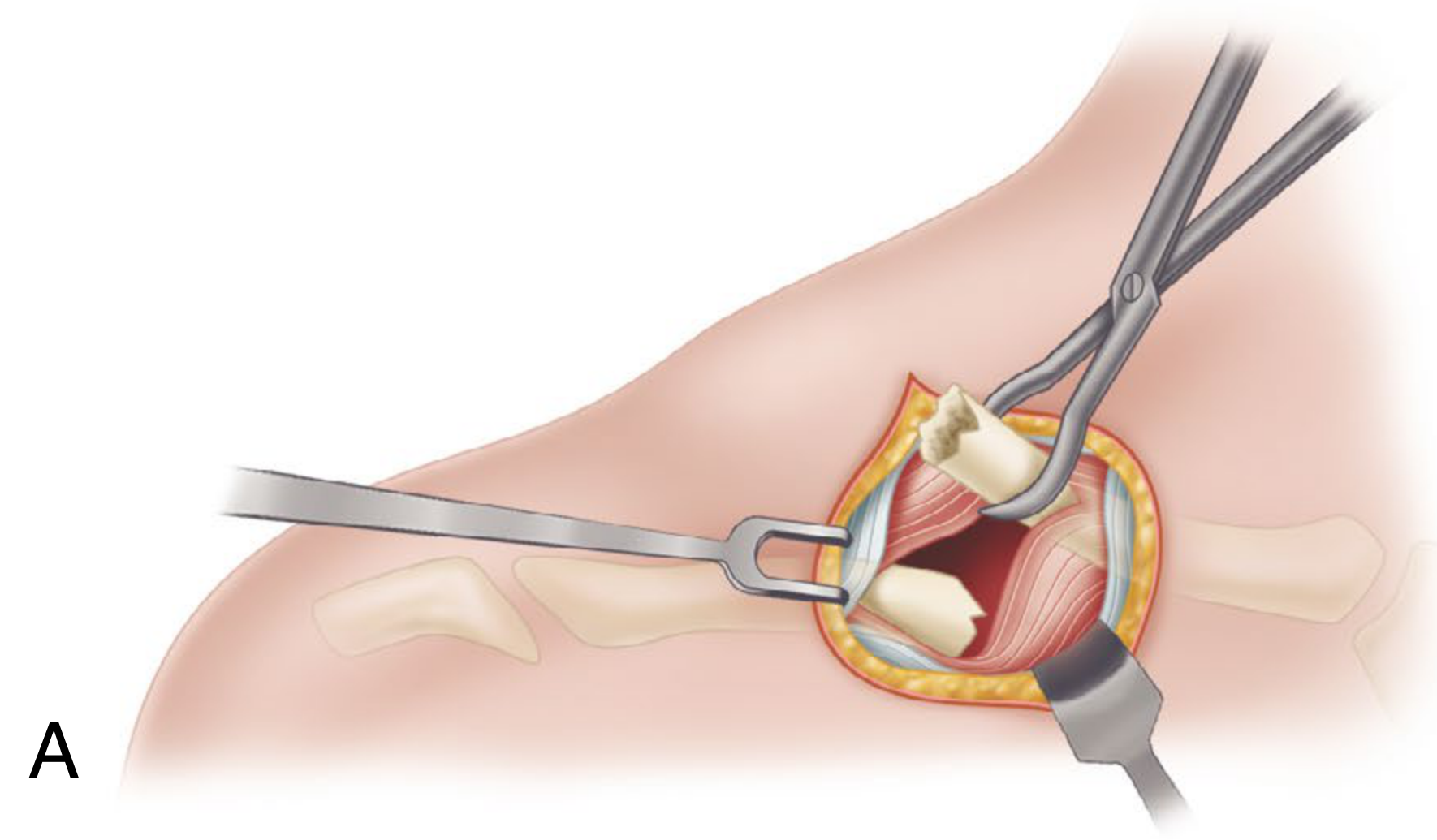
Step A: Elevation of the proximal (medial fragment) end of the clavicle through the posterolateral incision - Campbell's Operative Orthopaedics, 15th ed. (2026)
Phase 1 - Preparing the Medial Fragment
Step 3 - Elevate the medial fragment
- Use a towel clip to elevate the proximal end of the medial clavicle through the incision
- This brings the medullary canal mouth into the wound for direct access
Step 4 - Drill the medial canal
- Attach the appropriately sized drill to a ratchet T-handle
- Drill the medullary canal of the medial fragment
- Take care not to penetrate the anterior cortex - keep the drill within the canal
Step 5 - Tap the medial canal
- Remove the drill; attach the same-sized tap to the T-handle
- Tap the medullary canal to the anterior cortex
- Hand tapping is strongly recommended - especially for small patients and smaller-diameter pins (avoids over-tapping)
Phase 2 - Preparing the Lateral Fragment
Step 6 - Elevate the lateral fragment
- Elevate the lateral fragment through the incision
- Externally rotate the arm and shoulder - this improves exposure of the lateral fragment canal
Step 7 - Drill the lateral canal
- Use the same-sized drill on the lateral fragment medullary canal
Step 8 - Pass drill through posterolateral cortex
- Under C-arm guidance, pass the drill out through the posterolateral cortex of the lateral fragment
- Exit point: posterior and medial to the AC joint, approximately at the level of the coracoid
- Critical: allow the drill to exit no higher than the equator (midpoint) of the posterolateral clavicle - exiting too superiorly risks the supraclavicular nerve; too inferiorly risks the subclavian vessels
Step 9 - Tap the lateral canal
- Attach the tap and tap the lateral medullary canal so the large threads are fully advanced into the canal
- If the tap is a tight fit, re-drill with the next larger size
Phase 3 - Nail Passage and Reduction
Step 10 - Insert nail into lateral fragment (trocar end first)
- Remove nuts from the pin assembly
- Pass the trocar end of the nail into the medullary canal of the lateral fragment
- Advance until it exits through the previously drilled posterolateral cortex hole
- The pin tip will now be felt subcutaneously posterior to the shoulder
Step 11 - Exteriorize the nail tip
- Make a small stab incision directly over the palpable subcutaneous pin tip
- Spread subcutaneous tissue with a hemostat
- Place hemostat tip under the clavicle pin tip to facilitate passage out through this stab incision
- Drill the pin laterally/out until the large medial threads just start to engage the cortex
Step 12 - Retract nail into lateral fragment
- Attach a Jacobs chuck and T-handle to the laterally protruding pin end
- Carefully retract the nail back into the lateral fragment until the tip is just inside the medial end of the lateral fragment, ready to cross the fracture
- Ensure correct orientation
Step 13 - Reduce the fracture and advance nail across
- Reduce the fracture (closed or open)
- Advance the pin into the medial fragment
- Lifting the shoulder helps facilitate pin passage across - counteracts the downward pull of the arm weight
- Advance until all medial threads are across the fracture site
Phase 4 - Final Fixation and Compression
Step 14 - Apply nuts and compress
- Place the medial nut on the pin, followed by the smaller lateral nut
- Cold weld the two nuts: grasp the medial nut with needle-nose pliers; tighten the lateral nut against it with the lateral nut wrench
- Use T-handle and wrench to medially advance the pin down into the medial fragment until it contacts the anterior cortex
- Confirm final position with fluoroscopy - check both AP and oblique (45° caudal/cephalad) views
Step 15 - Final tightening
- Break the cold weld between the two nuts
- Re-tighten the lateral nut to the desired compression
- Cut any excess pin tail if needed
Reducing Complications (Frigg et al. Principles)
Per Frigg et al. (cited in Campbell's), complication rates are reduced by following these steps:
- Use an endcap - prevents nail migration medially
- Convert to open reduction after two failed attempts at closed reduction - do not persist with blind manipulations
- Use careful manual passage - never force the nail; torquing risks cortical perforation
- Rule out lateral perforation using intraoperative oblique radiographs specifically
- Limit postoperative range of motion to 90° for 6 weeks - reduces stress on the nail before fracture healing
Specific Hazards During This Approach
| Step | Hazard | Note |
|---|---|---|
| Platysma division | Supraclavicular nerve (middle branch) directly below | Identify and retract |
| Drilling medial canal | Anterior cortex perforation | Keep drill within canal; do not plunge |
| Posterolateral cortex exit | Too superior = nerve injury; too inferior = subclavian/pleural injury | Exit at equator of posterolateral clavicle only |
| Nail passage across fracture | Cortical breach; failure to reduce | Two attempts maximum before converting to open |
| Medial fragment advancement | Anterior cortex impingement | Stop when pin contacts anterior cortex; confirm on fluoroscopy |
| Final tightening | Distraction at fracture site | Nuts must be oriented for compression, not distraction |
Postoperative
- Sling for comfort
- ROM limited to 90° for 6 weeks
- Full return of activities at fracture union (~2 months for simple patterns)
- Hardware removal is expected with unlocked TENs once healing ensues - typically done under local anaesthetic through the original small stab incision
Sources: Campbell's Operative Orthopaedics, 15th ed. (2026), Technique 62.2; Rockwood and Green's Fractures in Adults, 10th ed. (2025)
This is a shared conversation. Sign in to Orris to start your own chat.