Kft interpretation
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Now I have comprehensive information to provide a thorough KFT interpretation guide.
Kidney Function Tests (KFT) - Complete Interpretation Guide
KFT (also called Renal Function Tests / RFT) is a panel of blood and urine investigations used to assess how well the kidneys are filtering waste, regulating electrolytes, and maintaining fluid balance. Here is how each component is interpreted:
1. Serum Creatinine
| Reference Range | Interpretation |
|---|---|
| Males: 0.7-1.3 mg/dL | Normal |
| Females: 0.5-1.1 mg/dL | Normal |
| Elevated | Reduced GFR / renal impairment |
Key points:
- Creatinine is a waste product of muscle metabolism. Serum levels depend on muscle mass, age, gender, race, and dietary meat intake.
- Normal serum creatinine ranges from 0.5 mg/dL (thin/elderly women) to 1.5 mg/dL (muscular men) - Goldman-Cecil Medicine
- Creatinine rises in a parabolic fashion as GFR falls - large drops in GFR cause small creatinine changes at higher GFR, but small drops cause large creatinine changes at low GFR
- Drugs that falsely elevate creatinine (by blocking tubular secretion): cimetidine, trimethoprim, fenofibrate, salicylates
- Serum creatinine remains normal with unilateral renal pathology if the contralateral kidney functions normally - Bailey & Love's Surgery
2. Blood Urea Nitrogen (BUN)
| Reference Range | Value |
|---|---|
| Normal | 7-20 mg/dL (2.5-7.1 mmol/L) |
- BUN is a product of protein catabolism processed by the liver and excreted by the kidneys
- BUN:Creatinine Ratio (normal = 10:1 to 20:1)
- >20:1 (prerenal): dehydration/hypovolemia, upper GI bleed, high protein diet, corticosteroid use
- <10:1: malnutrition, liver disease (reduced urea production), low protein intake
- 10-20:1: intrinsic renal disease (ratio usually stays "normal" proportionally)
"In volume-contracted states, this ratio may increase because of an associated differential increase in urea reabsorption in the collecting duct." - Comprehensive Clinical Nephrology, 7th Ed.
3. eGFR (Estimated Glomerular Filtration Rate)
eGFR is the most clinically informative marker of overall kidney function. The CKD-EPI equation is now the preferred formula (replaced MDRD), using serum creatinine, age, and sex.
KDIGO CKD Staging by eGFR
| Stage | eGFR (mL/min/1.73 m²) | Description |
|---|---|---|
| G1 | ≥90 | Normal or high |
| G2 | 60-89 | Mildly decreased |
| G3a | 45-59 | Mildly to moderately decreased |
| G3b | 30-44 | Moderately to severely decreased |
| G4 | 15-29 | Severely decreased |
| G5 | <15 | Kidney failure |
CKD is defined as eGFR <60 mL/min/1.73m² persisting for >3 months, OR evidence of kidney damage (proteinuria, hematuria, structural abnormality). - Comprehensive Clinical Nephrology, 7th Ed.
Schwartz equation is used for children:
eGFR = 0.413 × Height (cm) / Serum Creatinine (mg/dL)
Cystatin C is an emerging, more accurate GFR marker - not influenced by muscle mass, freely filtered, not tubularly secreted. Now incorporated into updated CKD-EPI equations.
4. Serum Urea (BUN)
Often reported as urea (mmol/L) in many countries, or BUN (mg/dL) in others.
- Conversion: BUN (mg/dL) = Urea (mmol/L) × 2.8
- Elevated in: dehydration, high protein intake, GI bleed, renal failure, catabolic states
- Low in: liver disease, malnutrition, overhydration
5. Serum Electrolytes
| Electrolyte | Normal Range | Clinical Notes |
|---|---|---|
| Sodium (Na⁺) | 136-145 mEq/L | Hyponatremia in nephrotic syndrome, SIADH; hypernatremia in dehydration |
| Potassium (K⁺) | 3.5-5.0 mEq/L | Hyperkalemia is a key complication of renal failure - can be fatal |
| Bicarbonate (HCO₃⁻) | 22-29 mEq/L | Low in metabolic acidosis of CKD |
| Chloride (Cl⁻) | 96-106 mEq/L | Interpreted with Na and bicarb for acid-base status |
6. Serum Uric Acid
| Reference Range | Value |
|---|---|
| Males | 3.4-7.0 mg/dL |
| Females | 2.4-6.0 mg/dL |
- Elevated in gout, renal impairment, diuretic use, high purine diet
- Uric acid is filtered and partially reabsorbed/secreted by the tubules
7. Serum Calcium & Phosphorus
These are routinely checked in renal panels because the kidneys regulate their balance:
- Calcium (normal: 8.5-10.5 mg/dL): Low serum albumin artificially lowers measured calcium - correct by adding 0.8 mg/dL for every 1 g/dL albumin is below 4 g/dL
- Phosphorus (normal: 2.5-4.5 mg/dL): Rises in CKD as phosphate excretion fails
- In CKD, the pattern is typically: low calcium + high phosphorus + elevated PTH (secondary hyperparathyroidism)
8. Urine Analysis Components
| Test | Normal | Significance |
|---|---|---|
| Urine specific gravity | 1.005-1.030 | Low in renal tubular disease, DI; high in dehydration |
| Proteinuria | <150 mg/day (trace or absent) | Key marker of glomerular damage; >3.5 g/day = nephrotic range |
| Hematuria | Absent | Glomerulonephritis, stones, malignancy |
| Urine sodium | Variable | Low (<20 mEq/L) in prerenal; high (>40 mEq/L) in ATN |
| FENa | - | <1% = prerenal; >1% = intrinsic renal (ATN) |
Fractional Excretion of Sodium (FENa):
FENa = (U_Na × P_Cr) / (U_Cr × P_Na) × 100
9. Creatinine Clearance (CrCl)
Calculated from a 24-hour urine collection:
CrCl = (U_Cr × Urine flow rate) / P_Cr
- Estimates GFR but overestimates it slightly due to tubular secretion of creatinine
- Cockcroft-Gault equation estimates CrCl without urine collection - used for drug dosing adjustments
Summary: Quick Clinical Clues
| Pattern | Likely Cause |
|---|---|
| High creatinine + low eGFR + high K⁺ + metabolic acidosis | CKD/AKI |
| High BUN:Cr ratio (>20) + low urine Na (<20) | Prerenal (dehydration/hypovolemia) |
| Normal BUN:Cr + elevated creatinine + urine Na >40 | Intrinsic renal disease (ATN) |
| Nephrotic: heavy proteinuria + low albumin + edema | Glomerular disease |
| Low Ca²⁺ + high PO₄ + high PTH + anemia | CKD with secondary hyperparathyroidism |
Sources:
- Campbell-Walsh-Wein Urology
- Comprehensive Clinical Nephrology, 7th Edition
- Goldman-Cecil Medicine
- Textbook of Family Medicine, 9th Edition
- Bailey & Love's Short Practice of Surgery, 28th Edition
What is acute kidney injury
Finding Sources
Searching PubMed
"acute kidney injury"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information. Here is a thorough guide on Acute Kidney Injury:
Acute Kidney Injury (AKI)
Definition
AKI is defined by the KDIGO (Kidney Disease: Improving Global Outcomes) criteria as any of the following:
- Rise in serum creatinine ≥0.3 mg/dL within 48 hours, OR
- Rise in serum creatinine to ≥1.5× baseline within 7 days, OR
- Urine output <0.5 mL/kg/h for ≥6 hours
- National Kidney Foundation Primer on Kidney Diseases, 8th Ed.
KDIGO Staging
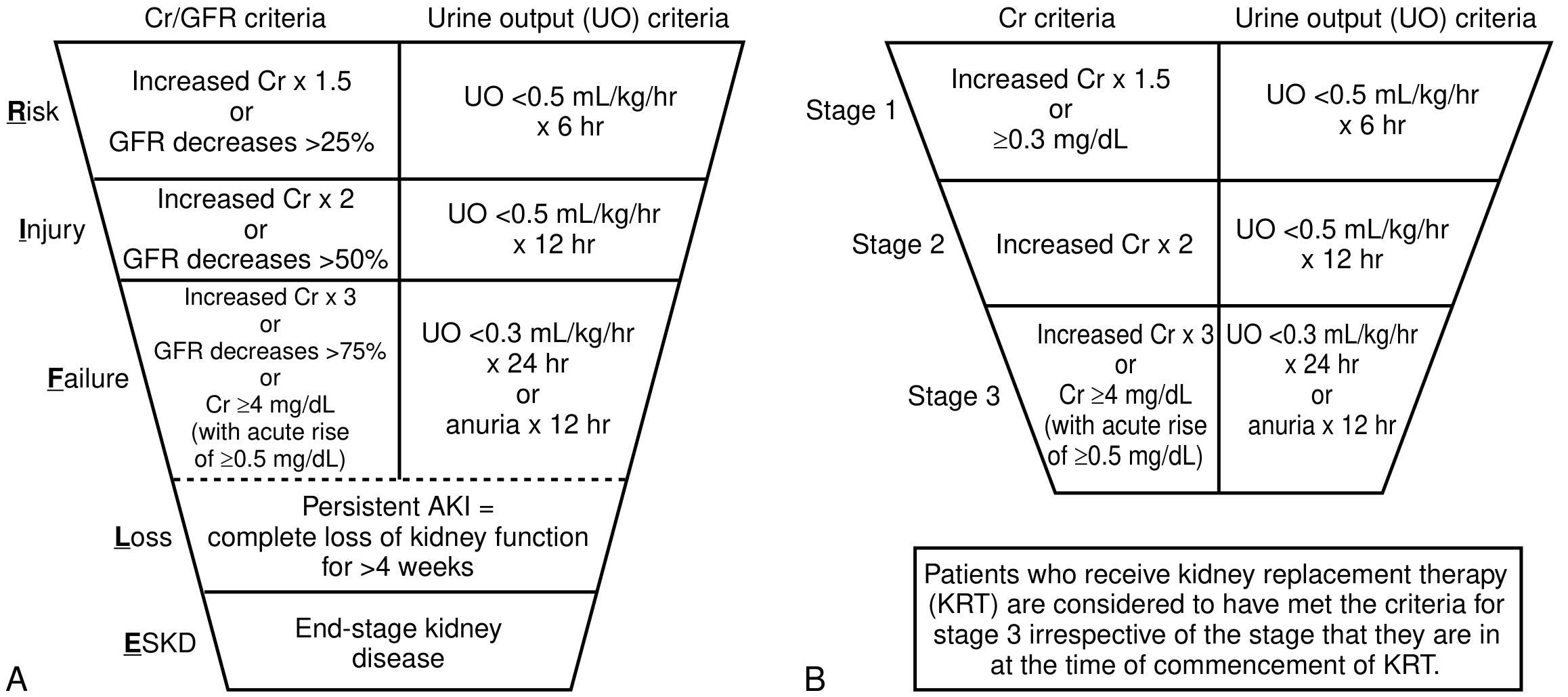
| Stage | Serum Creatinine Criteria | Urine Output Criteria |
|---|---|---|
| 1 | ↑ ≥0.3 mg/dL OR ↑ ×1.5-1.9 from baseline | <0.5 mL/kg/h for 6-12 h |
| 2 | ↑ ×2.0-2.9 from baseline | <0.5 mL/kg/h for ≥12 h |
| 3 | ↑ ×3.0 OR ≥4.0 mg/dL OR initiation of RRT* | <0.3 mL/kg/h for ≥24 h OR anuria ≥12 h |
*In patients <18 years: eGFR <35 mL/min/1.73m² also qualifies for Stage 3.
Patients who receive kidney replacement therapy (KRT) are automatically classified as Stage 3 regardless of their creatinine at the time KRT is started.
Classification by Cause
AKI is classically divided into three anatomical categories:
1. Prerenal AKI (~21% of hospital AKI)
Caused by reduced renal perfusion - GFR falls but the kidney itself is structurally intact initially.
Causes:
- True hypovolemia: hemorrhage, GI losses (vomiting/diarrhea), burns, diuretic overuse
- Reduced cardiac output: congestive heart failure, cardiogenic shock
- Systemic vasodilation: sepsis, liver failure (hepatorenal syndrome), anaphylaxis
- Renal vasoconstriction: NSAIDs, ACE inhibitors/ARBs in the setting of hypotension, contrast nephropathy
Key diagnostic features:
- BUN:Creatinine ratio >20:1
- Urine sodium <20 mEq/L
- FENa <1%
- Urine specific gravity high (concentrated urine)
- Reversible within 24-72 hours of fluid resuscitation/correction
"The hallmark of prerenal disease is its reversibility after treatment of the underlying cause, with absence of structural damage to the kidney if treated promptly." - Campbell-Walsh-Wein Urology
2. Intrinsic (Renal) AKI (~58% of hospital AKI)
Structural damage to the kidney itself.
| Compartment | Disease | Features |
|---|---|---|
| Tubules | Acute Tubular Necrosis (ATN) - most common (45%) | Urine Na >40, FENa >1%, muddy brown casts |
| Glomeruli | Glomerulonephritis, TTP/HUS | RBC casts, heavy proteinuria |
| Interstitium | Acute Interstitial Nephritis (AIN) | WBC casts, eosinophilia, drug/infection cause |
| Vessels | Renal artery/vein thrombosis, vasculitis |
Common causes of ATN:
- Ischemic: Prolonged hypotension, septic shock
- Nephrotoxic drugs: Aminoglycosides, amphotericin B, cisplatin, vancomycin, NSAIDs, contrast agents, cyclosporine, tenofovir
- Endogenous toxins: Myoglobin (rhabdomyolysis), hemoglobin (hemolysis), uric acid (tumor lysis syndrome)
Newer nephrotoxic agents to be aware of:
- Checkpoint inhibitors (nivolumab, pembrolizumab) - cause AIN
- Tyrosine kinase inhibitors (sorafenib, sunitinib) - cause TMA and proteinuria
3. Postrenal AKI (~10% of hospital AKI)
Caused by obstruction at any level of the urinary tract. Requires bilateral obstruction (or unilateral in a solitary kidney) to cause AKI.
Causes:
- Benign prostatic hyperplasia (most common in older men)
- Bilateral ureteral stones
- Pelvic/retroperitoneal malignancy
- Neurogenic bladder
- Strictures
Clinical Features
AKI is often asymptomatic in early stages. Symptoms arise from the metabolic consequences:
- Oliguria (urine output <400 mL/day) or anuria
- Fluid overload: edema, pulmonary edema, hypertension
- Uremic symptoms: nausea, vomiting, hiccups, metallic taste, encephalopathy, asterixis
- Fatigue, decreased appetite
Complications
| System | Complication |
|---|---|
| Metabolic | Hyperkalemia, metabolic acidosis (↑anion gap), hyponatremia, hypocalcemia, hyperphosphatemia, hyperuricemia, hypermagnesemia |
| Cardiovascular | Pulmonary edema, arrhythmias (from hyperkalemia), pericarditis, pericardial effusion, hypertension, MI |
| Gastrointestinal | Nausea, vomiting, GI hemorrhage, malnutrition |
| Neurologic | Encephalopathy, asterixis, seizures, mental status changes |
| Hematologic | Anemia, uremic bleeding (platelet dysfunction) |
| Infectious | Pneumonia, septicemia, UTI |
- Brenner & Rector's The Kidney, 2-Volume Set
Diagnosis: Key Lab Differentiation
| Test | Prerenal | Intrinsic (ATN) | Postrenal |
|---|---|---|---|
| BUN:Cr ratio | >20:1 | ~10-15:1 | Variable |
| Urine Na (mEq/L) | <20 | >40 | >40 |
| FENa | <1% | >1-2% | >1% |
| Urine osmolality | >500 mOsm/kg | <350 mOsm/kg | Variable |
| Urine specific gravity | >1.020 | ~1.010 (isosthenuric) | Variable |
| Urinary casts | Hyaline casts | Muddy brown granular casts | None or RBC/WBC |
Management
General Supportive Measures
- Treat the underlying cause - fluid resuscitation for hypovolemia, antibiotics for sepsis, relieve obstruction for postrenal
- Stop nephrotoxins - hold ACE inhibitors, ARBs, NSAIDs, contrast agents, aminoglycosides
- Optimize fluid balance - avoid both over- and under-hydration
- Nutrition: KDIGO recommends 20-30 kcal/kg/day; protein 0.8-1.0 g/kg/day (non-dialysis), 1.0-1.5 g/kg/day (dialysis), up to 1.7 g/kg/day (hypercatabolic on CRRT)
- Metabolic acidosis: Treat only if pH <7.20 and HCO₃⁻ <15 mmol/L with IV/oral sodium bicarbonate
- Hyperphosphatemia: Phosphate binders (calcium carbonate, sevelamer, lanthanum)
- DVT prophylaxis - avoid LMWH and factor Xa inhibitors in severe AKI; prefer unfractionated heparin
Renal Replacement Therapy (RRT)
Indications (the "AEIOU" mnemonic):
- A - Acidosis (severe, refractory to bicarbonate)
- E - Electrolytes (hyperkalemia refractory to medical management)
- I - Intoxications (certain toxic ingestions)
- O - Overload (volume/fluid overload refractory to diuretics)
- U - Uremia (asterixis, pericardial rub, encephalopathy, uremic bleeding)
Many nephrologists also initiate dialysis empirically when BUN exceeds ~100 mg/dL without signs of kidney recovery.
RRT modalities:
- Intermittent Hemodialysis (IHD) - standard, for hemodynamically stable patients
- Continuous Renal Replacement Therapy (CRRT) - preferred in septic shock or hemodynamic instability, as it avoids rapid intravascular fluid shifts
- Peritoneal Dialysis - alternative when vascular access is unavailable
"Initiating early RRT has not been demonstrated to improve survival and may increase the risk of adverse events." - Harrison's Principles of Internal Medicine, 22nd Ed.
Prognosis and Long-Term Outcomes
AKI carries significant long-term consequences even after apparent recovery:
- 72.1% of patients who had AKI without pre-existing CKD developed CKD within 2 years
- AKI requiring dialysis is associated with a 3.23× increased incidence of chronic dialysis vs. matched controls
- AKI increases risk of ESKD by 13-fold (no prior CKD) and 41-fold (with prior CKD)
- AKI that required dialysis carries >double the risk of death in the long-term
Recent systematic review (PMID: 40424522) confirms the significant long-term risk of adverse kidney outcomes after AKI episodes.
- Brenner & Rector's The Kidney
Key Concepts to Remember
| Concept | Detail |
|---|---|
| Baseline creatinine | Always needed for AKI diagnosis; if unavailable, KDIGO recommends back-calculating from MDRD assuming eGFR of 75 mL/min/1.73m² |
| AKD (Acute Kidney Disease) | New KDIGO term for kidney dysfunction lasting 7 days to 3 months - between AKI and CKD |
| Anuria vs. Oliguria | Anuria (<100 mL/day) suggests complete obstruction or cortical necrosis; oliguria <400 mL/day |
| "AKI on CKD" | Common scenario - these patients are at highest risk for rapid progression to ESKD |
Sources:
- Campbell-Walsh-Wein Urology
- Brenner & Rector's The Kidney, 2-Volume Set
- Harrison's Principles of Internal Medicine, 22nd Edition (2025)
- National Kidney Foundation Primer on Kidney Diseases, 8th Edition
- Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.