Genu valgus, genu varum, genu recurrvatum biomechanics types antomy diagnostic criteria for orthopaedic and role of physiotherapy
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Searching Images
genu valgum genu varum knee deformity alignment mechanical axis
Searching the Web
genu valgum varum recurvatum physiotherapy management biomechanics diagnostic criteria orthopaedics
Loading Image
Loading Image
Reading Web Page
https://www.physio-pedia.com/Valgus_Knee
Here is a comprehensive reference on all three knee angular deformities — their anatomy, biomechanics, classification, diagnostic criteria, orthopaedic management, and physiotherapy role.
Knee Angular Deformities: Genu Valgum, Genu Varum & Genu Recurvatum
1. Anatomical & Biomechanical Foundations
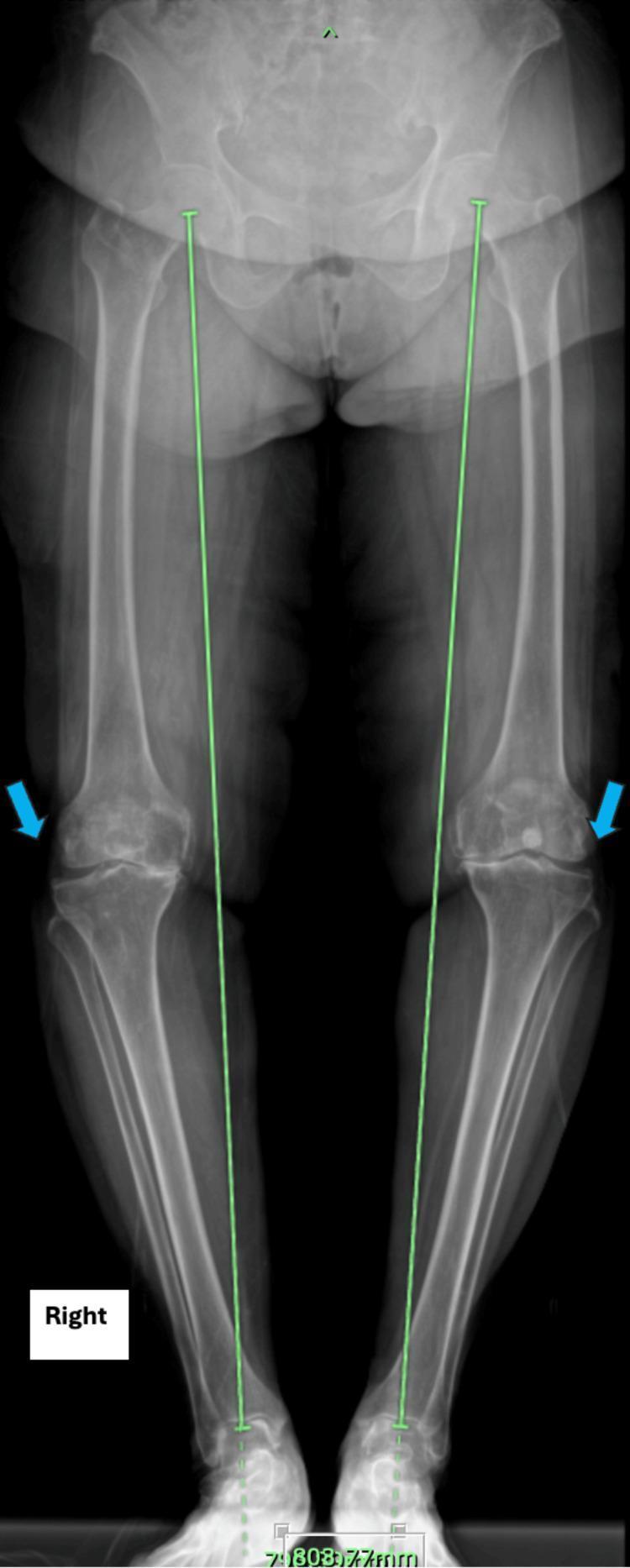
The Mechanical Axis (Mikulicz Line)
The cornerstone of understanding all three deformities is the mechanical axis of the lower limb — a straight line running from the centre of the femoral head through the intercondylar eminence of the tibial plateau down to the centre of the ankle mortise. In a normally aligned limb, all three large joints (hip, knee, ankle) lie on this line.
Key angular relationships:
- The anatomical axis of the femur and the mechanical axis diverge by ~6°
- The longitudinal anatomical axes of femur and tibia form a laterally open angle of 174° at the knee (femorotibial angle)
- Any deviation shifts joint loading abnormally — progressive cartilage and bone degeneration follows
General Anatomy and Musculoskeletal System (THIEME Atlas), p. 431
Axis deviation terminology (international guidelines):
| Plane | Type | Term |
|---|---|---|
| Frontal (coronal) | Concave to vertical axis / tibia points medially | Varus |
| Frontal (coronal) | Convex to vertical axis / tibia points laterally | Valgus |
| Sagittal | Hyperextension at knee | Recurvatum |
| Sagittal | Flexion deformity | Antecurvatum |
General Anatomy and Musculoskeletal System (THIEME Atlas), p. 46
2. Genu Varum (Bow Legs)
Definition
The knee joint centre lies lateral to the mechanical axis. The tibia points toward the median line.
Normal vs. Pathologic
| Age | Normal finding |
|---|---|
| 0–12 months | Up to 20° genu varum is physiologic |
| 18 months | Spontaneous correction begins |
| 3–4 years | Should resolve to neutral or slight valgus |
Miller's Review of Orthopaedics 9th Ed., p. 277
Types / Causes
| Type | Key Features |
|---|---|
| Physiologic | Symmetric, age <2 yrs, radiograph shows symmetric flaring of tibia and femur, self-resolving |
| Blount disease (infantile, 0–4 yrs) | Tibia vara; overweight child, early walker, internal tibial torsion; Drennan metaphyseal-diaphyseal angle >16° is abnormal |
| Blount disease (adolescent) | Unilateral, obesity-associated |
| Rickets | Bilateral, associated with vitamin D/calcium/phosphorus deficiency, rachitic rosary, frontal bossing |
| Skeletal dysplasia / OI / trauma | Asymmetric, based on underlying condition |
Biomechanical Consequences
- Mechanical axis passes medial to knee → medial compartment overloaded (compression)
- Lateral structures (lateral collateral ligament, iliotibial band, biceps femoris) under abnormal tension
- Greater stress on the lateral border of the foot → fallen pedal arch
- Long-standing varus → medial compartment osteoarthritis
THIEME Atlas, p. 431
Diagnostic Criteria (Orthopaedic)
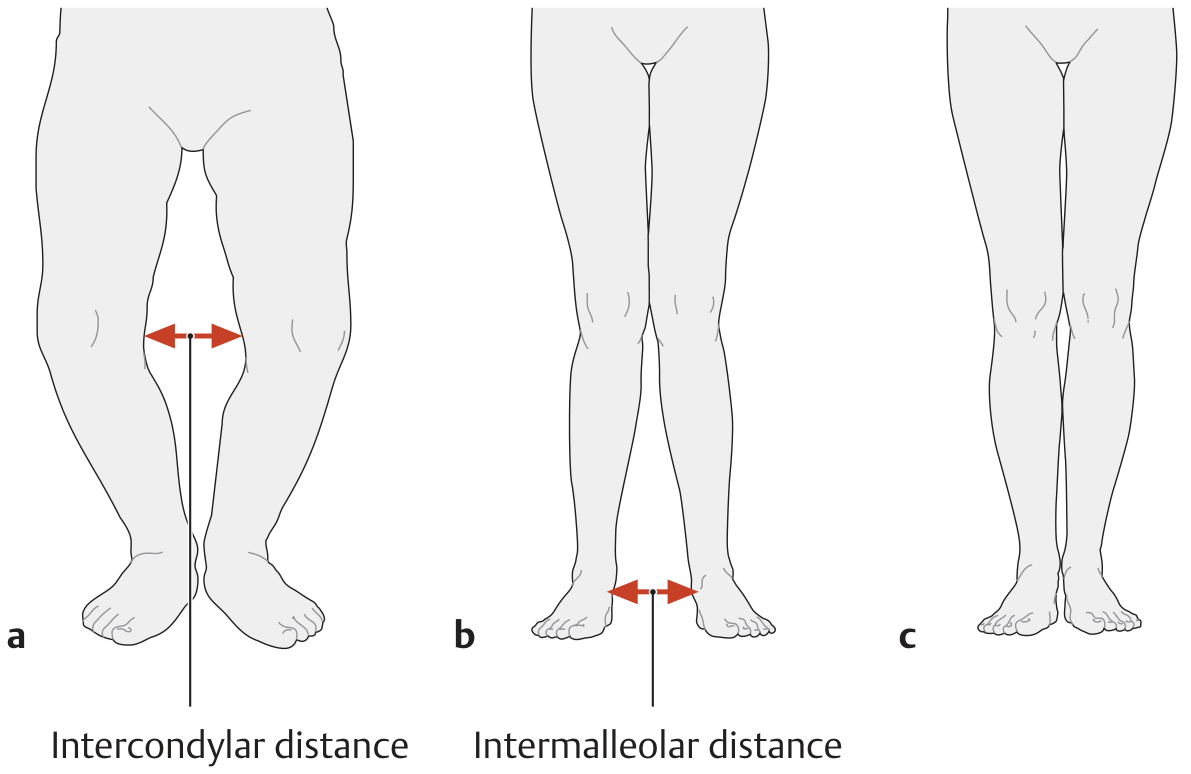
- Clinical: intercondylar distance >3 cm with feet together = abnormal
- Radiograph (weight-bearing full-length): mechanical axis passes medial to knee; Drennan angle >16° for Blount
- Pathologic if: asymmetric, persists beyond age 2, associated with short stature (<10th centile), pain, or prior infection/trauma
3. Genu Valgum (Knock Knees)
Definition
The knee joint centre lies medial to the mechanical axis. The tibia points away from the median line.
Normal vs. Pathologic
| Age | Normal finding |
|---|---|
| 2–6 yrs | Up to 15° valgus is physiologic |
| 3–4 yrs | Maximum physiologic valgus |
| 7 yrs | Resolves to slightly valgus adult alignment (~6°) |
Miller's Review of Orthopaedics 9th Ed., p. 278
Types / Causes
| Type | Features |
|---|---|
| Physiologic | Bilateral, symmetric, within age norms, no treatment needed |
| Renal osteodystrophy | Most common cause of bilateral pathologic valgum |
| Post-traumatic | Asymmetric proximal tibial growth stimulation after fracture or infection |
| Skeletal tumours | Osteochondromas at the proximal tibia |
| Obesity/hyperlaxity | Common in adolescent females |
Biomechanical Consequences
- Mechanical axis passes medial to knee centre → lateral compartment overloaded
- Medial structures (MCL) under tension/elongation
- Increased patellofemoral lateral pressure → anterior knee pain, patellar instability
- Increased Q-angle → lateral patellar tracking dysfunction
- Lateral compartment OA in chronic cases
Diagnostic Criteria (Orthopaedic)
- Clinical: intermalleolar distance >5 cm (THIEME) or >8 cm (StatPearls) with medial femoral condyles touching = abnormal
- Q-angle >10° indicates valgus malalignment
- Radiograph (weight-bearing full-length): mechanical axis medial to knee centre; valgus angulation measured at tibiofemoral joint
- Surgical threshold (children): >10 cm intermalleolar distance OR >15° valgus angulation in children >10 years
Miller's Review of Orthopaedics 9th Ed.; THIEME Atlas, p. 431
Orthopaedic Management
| Severity | Treatment |
|---|---|
| Physiologic / <15° in child <6 yrs | Observation only |
| Metabolic cause | Treat underlying disorder first |
| Pathologic / progressive | Hemiepiphysiodesis (guided growth) — medial distal femur; relies on Heuter-Volkmann law |
| Adolescent / skeletally mature | Corrective osteotomy (distal femoral varus osteotomy) |
| End-stage OA | Total knee arthroplasty |
4. Genu Recurvatum (Back Knee / Hyperextension)
Definition
Hyperextension of the knee joint in the sagittal plane — the knee extends beyond 0° (neutral). Also called "back-kneeing."
Types / Causes
| Type | Mechanism |
|---|---|
| Neuromuscular | Quadriceps weakness → gravity shifts body weight anterior to knee → hyperextension compensates; seen in muscular dystrophies, polio |
| Ligamentous laxity | Hypermobility syndromes (Ehlers-Danlos, Marfan), posterior capsule/oblique popliteal ligament insufficiency |
| Post-ACL reconstruction | Physeal injury with growth disturbance in children (physis-sparing techniques) |
| Anterior fat pad syndrome | Trauma → fibrous changes in fat pad → worsened in recurvatum position |
| Posteromedial corner injury | Unrepaired severe injury → chronic recurvatum instability |
Miller's Review of Orthopaedics 9th Ed.; Imaging Anatomy Atlas Vol. 3
Biomechanical Consequences
- The oblique popliteal ligament is the primary restraint to recurvatum — its failure is central to pathologic hyperextension
- Weight line shifts anterior to knee axis → posterior capsule and cruciate ligaments under chronic tensile stress
- Quadriceps function at disadvantage — passive hyperextension substitutes for active extension
- Compensatory lumbar hyperlordosis and anterior pelvic tilt common
General Anatomy and Musculoskeletal System (THIEME Atlas), p. 522
Diagnostic Criteria (Orthopaedic)
- Clinical: knee extension beyond 0° (normal extension = 5–10° hyperextension is borderline); pathologic if >10–15° or symptomatic
- Associated with: positive posterior drawer, PCL/posterolateral corner laxity
- Gait analysis: characteristic "back-kneeing" gait pattern
- Neurological assessment to exclude quadriceps weakness as primary cause
- MRI to evaluate posterior capsule, oblique popliteal ligament, PCL
5. Clinical Assessment Summary
Physical Examination Protocol
| Measurement | Genu Varum | Genu Valgum |
|---|---|---|
| Standing (feet together) | Intercondylar distance (knees apart) | Intermalleolar distance (ankles apart) |
| Threshold | >3 cm = abnormal | >5–8 cm = abnormal |
Radiographic Assessment
- Weight-bearing full-length AP radiograph (hip to ankle) — gold standard
- Measures: mechanical axis deviation, tibiofemoral angle, Drennan angle (Blount)
- Low-dose biplanar systems (EOS imaging) increasingly used
- CT scanogram for limb length discrepancy
Grainger & Allison's Diagnostic Radiology
6. Role of Physiotherapy
Physiotherapy plays a critical role in conservative management, pre-surgical optimisation, and post-surgical rehabilitation.
A. Genu Valgum — Physiotherapy
Goal: Realign and stabilise the knee by correcting muscle imbalances
| Target | Weakness Found | Exercise Intervention |
|---|---|---|
| Hip abductors / external rotators | Commonly weak → tibial internal rotation | Hip abduction with resistance band, clamshells, side-lying leg raises |
| Vastus medialis oblique (VMO) | Deficient → lateral patellar tracking | Terminal knee extensions, single-leg squats, VMO-biased leg press |
| Glutes (maximus + medius) | Underactive → knee valgus during gait | Bridges, squats with resistance band around thighs, step-ups |
| ITB / lateral retinaculum | Often tight | Foam rolling, soft tissue mobilisation, lateral hip flexor stretching |
| Proprioception | Impaired in chronic cases | Single-leg stance, wobble board, perturbation training |
Specific exercises:
- Single-leg band stretches (hip abductor strengthening)
- Leaning ankle band stretches (hip flexor stretch + ankle stabilisation)
- Resistance band squats (quadriceps + hip abductor co-activation)
- Step-down with knee alignment cues (neuromuscular re-education)
Physiopedia — Valgus Knee
B. Genu Varum — Physiotherapy
Goal: Offload medial compartment, strengthen lateral stabilisers
| Target | Rationale | Intervention |
|---|---|---|
| Hip abductors | Reduce lateral pelvic drop (Trendelenburg) → less varus moment | Hip abduction strengthening |
| Lateral quadriceps (VL) | Unload medial compartment | Lateral step-ups |
| Gait retraining | Lateral trunk lean reduces medial knee adduction moment | Walking/running gait feedback |
| Foot pronation | Compensates for varus; may need orthotic | Medial wedge insoles, intrinsic foot exercises |
| Iliotibial band | Under excess tension in varus | Stretching, soft tissue work |
C. Genu Recurvatum — Physiotherapy
Goal: Restore active knee control and eliminate compensatory hyperextension
| Target | Intervention |
|---|---|
| Quadriceps strengthening | Core of all recurvatum rehab — removes reliance on passive hyperextension; straight-leg raises, mini-squats, leg press |
| Hamstring strengthening | Dynamic posterior stabiliser; Nordic curls, prone knee flexion with resistance |
| Proprioception / neuromuscular control | Perturbation training, single-leg stance on unstable surfaces |
| Posterior capsule stretching | Gentle only — avoid further laxity |
| Gait retraining | Cue patient to maintain slight flexion at heel-strike; taping/bracing as adjunct |
| Core and pelvic stability | Address lumbar hyperlordosis; pelvic floor and deep abdominals |
THIEME Atlas of Anatomy — Knee Muscle Function, p. 522–523
Orthotics & Adjuncts in Physiotherapy
- Medial wedge insoles (genu varum): shift load laterally
- Valgus unloader brace (medial compartment OA + varum)
- Knee immobiliser / hyperextension brace (recurvatum with ligamentous laxity)
- Kinesio taping — patellar tracking (valgum), quadriceps facilitation (recurvatum)
7. Orthopaedic Decision Algorithm
Angular deformity detected
↓
Age-appropriate physiologic? → YES → Observe, review 6–12 monthly
↓ NO
Identify cause (metabolic, trauma, infection, dysplasia)
↓
Treat underlying condition
↓
Persistent / progressive / pain / LLD?
↓
Skeletally immature → Guided growth (hemiepiphysiodesis)
Skeletally mature → Corrective osteotomy
End-stage OA → TKR / UKR
Summary Table
| Feature | Genu Varum | Genu Valgum | Genu Recurvatum |
|---|---|---|---|
| Plane | Coronal | Coronal | Sagittal |
| Knee centre vs. axis | Lateral to axis | Medial to axis | Posterior/hyperextension |
| Overloaded compartment | Medial | Lateral | Posterior capsule / PCL |
| Clinical measure | Intercondylar distance | Intermalleolar distance | Degree of hyperextension |
| Pathologic threshold | >3 cm / Drennan >16° | >8 cm / >15° | >10–15° hyperextension |
| Key physio target | Hip abductors, gait | VMO, hip ER, glutes | Quadriceps, hamstrings |
| Surgery (child) | Hemiepiphysiodesis medial tibia | Hemiepiphysiodesis medial femur | PCL/posterolateral corner repair |
Sources: Miller's Review of Orthopaedics 9th Edition; General Anatomy and Musculoskeletal System (THIEME Atlas of Anatomy); Grainger & Allison's Diagnostic Radiology; Harrison's Principles of Internal Medicine 22E; Imaging Anatomy Atlas Vol. 3; Physiopedia — Valgus Knee; StatPearls — Genu Valgum.
This is a shared conversation. Sign in to Orris to start your own chat.