23 year old male with loose stools and lower abdominal pain since 4 days which start 1 hour after eating food relived on standing up aggrevated by lying down mostly at night
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Searching PubMed
"irritable bowel syndrome" AND "diarrhea predominant" AND management
I now have comprehensive information to provide a detailed clinical analysis. Here is my full response:
Clinical Analysis: 23-Year-Old Male with Loose Stools and Lower Abdominal Pain
The Symptom Pattern - What Stands Out
This presentation is highly characteristic. Let me break down each feature:
| Feature | Clinical Significance |
|---|---|
| Age 23, male | Classic IBS demographic (though IBS is more common in women overall) |
| 4 days duration | Acute onset - could be post-infectious trigger |
| Loose stools + lower abdominal pain | Core IBS-D (diarrhea-predominant) symptoms |
| Starts 1 hour after eating | Exaggerated gastrocolic reflex - hallmark of IBS |
| Relieved on standing | Positional relief - functional disorder behavior |
| Aggravated by lying down | Positional worsening - typical functional pattern |
| Mostly at night | This is a yellow flag - see below |
Most Likely Diagnosis: IBS-D (Diarrhea-Predominant IBS)
Rome IV Diagnostic Criteria (2016)
Recurrent abdominal pain, on average at least 1 day/week in the last 3 months, associated with 2 or more of:
- Related to defecation
- Associated with a change in frequency of stool
- Associated with a change in form (appearance) of stool
This patient meets criteria provisionally (though only 4 days - so IBS technically requires 3+ months; the pattern is classic for early/evolving IBS or post-infectious IBS).
Why Postprandial Onset?
As Harrison's explains - IBS patients exhibit increased rectosigmoid motor activity for up to 3 hours after eating. The motility index and peak amplitude of high-amplitude propagating contractions (HAPCs) in IBS-D patients are greatly increased compared to healthy subjects and are associated with rapid colonic transit accompanied by abdominal pain. This is the mechanistic basis for pain starting 1 hour after meals.
Additionally, there is visceral hypersensitivity: lipids lower the thresholds for gas, discomfort, and pain in IBS patients - so the postprandial state (fat release, CCK secretion) triggers an exaggerated response.
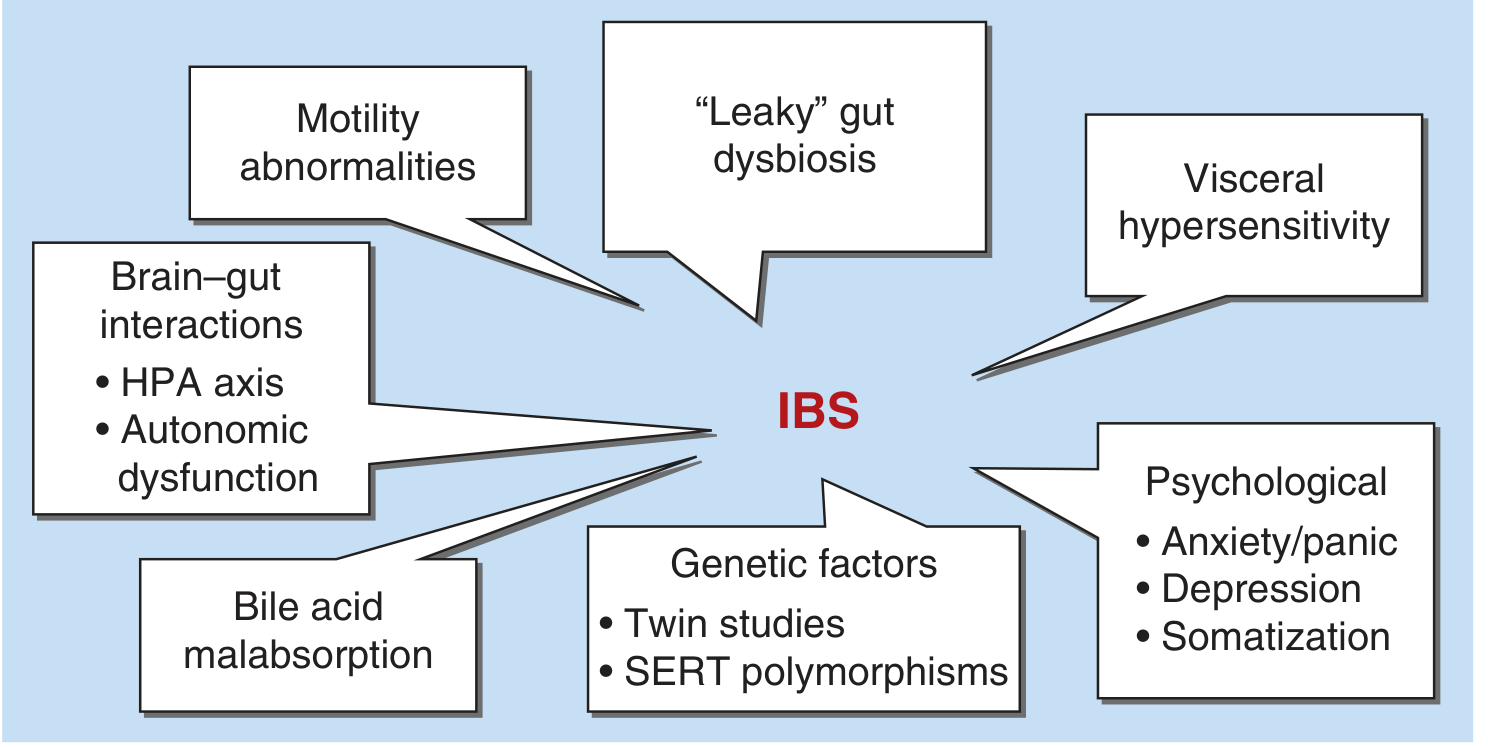
Pathophysiology of IBS - multifactorial (Harrison's Principles of Internal Medicine, 22E)
⚠️ Yellow Flag: Nocturnal Symptoms
Symptoms mostly at night is atypical for IBS. Classical teaching states that nocturnal diarrhea argues against IBS. This must be explained:
- True organic disease (IBD, microscopic colitis, infection) causes nocturnal diarrhea
- However, positional aggravation (lying down) worsening symptoms - rather than waking from sleep with urgency - may explain the "night" predominance
Ask specifically: Does he wake from sleep to defecate (true nocturnal diarrhea = organic cause more likely), or does he simply experience more symptoms while lying in bed at night while still awake?
Differential Diagnosis
Given this is only 4 days old, consider these in parallel with IBS:
| Diagnosis | Supporting Features | Against |
|---|---|---|
| IBS-D | Young age, postprandial onset, positional relationship, no blood | Only 4 days (<3 months for formal dx) |
| Post-infectious IBS | Acute onset, may follow gastroenteritis | Need history of prior GI infection |
| Giardiasis | Loose stools, lower abdominal cramps, young person | Usually no positional variation |
| IBD (Crohn's disease) | Young male, lower abdominal pain, diarrhea | No blood, no weight loss, no fever described |
| Celiac disease | Loose stools, abdominal pain | Usually bloating, steatorrhea; no wheat history given |
| Lactose intolerance | Postprandial, loose stools | Usually within 30 min, more gassy |
| Small intestinal bacterial overgrowth (SIBO) | Bloating, loose stools, abdominal pain | Usually more distension |
| Infectious diarrhea | Acute 4-day onset | Usually self-limiting, fever often present |
As Harrison's notes: "When diarrhea is the major complaint, the possibility of lactose deficiency, laxative abuse, malabsorption, celiac sprue, hyperthyroidism, IBD, and infectious diarrhea must be ruled out." - Harrison's Principles, 22E
Alarm Features to Screen For (Ask the Patient)
- Blood in stool or rectal bleeding
- Significant unintentional weight loss
- Fever
- Onset after age 40 (not applicable here)
- Family history of colorectal cancer, IBD, or celiac disease
- Nocturnal diarrhea that wakes him from sleep
- Progressive worsening
If none of the above, this is a low-risk presentation.
Investigations
For a young patient with no alarm features, investigations should be targeted, not exhaustive:
First line (minimum):
- CBC (rule out anemia, leukocytosis)
- CRP / ESR (rule out inflammatory process)
- Fecal calprotectin - most important: elevated in IBD, normal in IBS. Harrison's specifically recommends this "even in the absence of alarm features to rule out IBD" in IBS-D
- Stool microscopy, culture, ova & parasites (especially if travel history or endemic area for parasites - relevant in many regions)
- Stool for Giardia antigen (given acute onset)
- Serum anti-tTG IgA (celiac screening, if IBS-D pattern)
Second line (if first line inconclusive or red flags):
- Hydrogen breath test (lactase deficiency, SIBO)
- Colonoscopy with random biopsies (microscopic colitis) - only if alarm features or no response to treatment
Management
1. Reassurance and Education
Explain the functional nature and the gut-brain axis mechanism. This alone reduces health anxiety and improves outcomes.
2. Dietary Modification
- Low-FODMAP diet - strong evidence for IBS-D; reduces fermentable carbohydrates that drive symptoms
- Identify and eliminate personal food triggers (dairy, gluten, high-fat meals, caffeine)
- Encourage regular meals; avoid skipping and then large meals
- Soluble fiber (psyllium) can help regulate stool form
3. Pharmacological (if dietary measures insufficient)
| Drug Class | Agent | Role |
|---|---|---|
| Antispasmodic | Mebeverine, hyoscine butylbromide | For abdominal cramping/pain |
| Antidiarrheal | Loperamide | Reduces stool frequency; does NOT improve global IBS or pain |
| Gut-selective antibiotic | Rifaximin | For IBS-D, particularly if SIBO component |
| Tricyclic antidepressant (low dose) | Amitriptyline 10-25 mg | Modulates visceral hypersensitivity, reduces diarrhea |
| Serotonin modulator | Alosetron (5-HT3 antagonist) | IBS-D in women; restricted use |
| Peppermint oil | Enteric-coated capsules | Antispasmodic, OTC, reasonable evidence |
4. Psychological/Behavioral
- Stress management, cognitive behavioral therapy (CBT)
- Gut-directed hypnotherapy has good evidence
Clinical Bottom Line
This 23-year-old male almost certainly has IBS-D, with the postprandial onset, positional features, and young age being highly supportive. The 4-day duration means you should also actively exclude acute infectious gastroenteritis and Giardia (which can mimic IBS and trigger post-infectious IBS).
The nocturnal predominance needs clarification - if he is waking from sleep to defecate, organic disease (IBD, infection) should be prioritized. If symptoms are simply worse when lying in bed at night (positional), functional etiology remains most likely.
Start with: Stool culture + Giardia antigen + fecal calprotectin + CBC + CRP. Reassure, trial of low-FODMAP diet, antispasmodic PRN. Review at 2-4 weeks.
Sources: Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine, International Edition; Sleisenger & Fordtran's Gastrointestinal and Liver Disease
Dark coloured stools , no h/o fever
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
I have enough information now. Here is the updated, comprehensive clinical analysis:
🔴 Critical Update: Dark Stools (Melena) = Alarm Feature
This changes the diagnosis entirely. Dark/black tarry stools are melena until proven otherwise - a direct indicator of upper gastrointestinal bleeding. Combined with lower abdominal pain, postprandial onset, and nocturnal symptoms in a 23-year-old male, this presentation now points strongly toward peptic ulcer disease (PUD), most likely a duodenal ulcer, as the primary diagnosis.
IBS is now excluded as the working diagnosis - loose dark stools are not a feature of IBS.
Revised Leading Diagnosis: Duodenal Ulcer with Bleeding (Complicated PUD)
Why Duodenal Ulcer Fits This Presentation
| Symptom | Duodenal Ulcer Explanation |
|---|---|
| Pain 1 hour after food | DU pain classically occurs 1-3 hours postprandially when the acid bolus empties into the unprotected duodenum |
| Relieved on standing | Positional relief is documented in PUD - gravity and posture affect acid pooling |
| Aggravated lying down | Lying flat increases acid contact with duodenal mucosa |
| Night pain (50-88% of DU patients) | Classic - pain wakes patients at night due to acid hypersecretion during sleep; present in up to 88% of DU cases |
| Dark/black stools (melena) | Blood from duodenum undergoes bacterial digestion → black tarry stool |
| Loose stools | Altered stool consistency from blood in the bowel - melaena can appear "loose" or tarry |
| No fever | Uncomplicated ulcer bleed - no perforation or peritonitis |
| Young male | DU is more common in young males, strongly associated with H. pylori |
From Yamada's Textbook of Gastroenterology: nocturnal pain occurs in 50-88% of duodenal ulcer patients vs only 24-32% in functional dyspepsia, and pain occurs at night in 32-43% of gastric ulcer cases. This strongly favors organic disease over functional.
Pathophysiology
In duodenal ulcer, there is increased gastric acid secretion and/or impaired mucosal defence. The most common cause in a 23-year-old is:
- Helicobacter pylori infection (most likely) - causes ~90-95% of DU in developing countries
- NSAIDs - ask about regular analgesic use (aspirin, ibuprofen, diclofenac)
- Stress - physiological or psychological
- Rare: Zollinger-Ellison syndrome (gastrinoma) if symptoms severe and refractory
The bleeding occurs when the ulcer erodes into a submucosal vessel - most dangerously the gastroduodenal artery on the posterior wall of the duodenum.
Differential Diagnosis of Melena in a 23-Year-Old
| Diagnosis | Likelihood | Key Distinguishing Feature |
|---|---|---|
| Duodenal ulcer | Most likely | Postprandial, nocturnal pain, young male |
| Gastric ulcer | Possible | Pain often worsened by food (not relieved) |
| Erosive gastritis/duodenitis | Possible | NSAID/alcohol history; less severe bleed |
| Mallory-Weiss tear | Less likely | Preceded by vomiting/retching |
| Esophageal varices | Unlikely at 23 | Liver disease, alcohol history; massive bleed |
| Meckel's diverticulum | Possible | Can present <25 years with melena |
| IBD (Crohn's) | Possible | Often also has fever, weight loss |
Note: Dark stools from diet (iron tablets, red meat, bismuth, beetroot) must also be excluded - confirm the stools are truly tarry/black with a characteristic offensive smell (melena) vs simply dark-coloured from dietary causes.
⚠️ Immediate Risk Assessment
Apply the Glasgow-Blatchford Score (GBS) - used pre-endoscopy to assess need for urgent intervention:
| Parameter | This Patient |
|---|---|
| Haemoglobin | Unknown - order urgently |
| Urea | Unknown - order urgently |
| Systolic BP | Assess now |
| Heart rate | Assess now |
| Melena | +1 point |
| Syncope/presyncope | Ask patient |
A GBS of 0 can be managed outpatient; any score ≥1 warrants inpatient management and endoscopy within 24 hours.
As Goldman-Cecil notes: "Upper GI bleeding is manifested by bloody emesis, coffee ground emesis, and, in most cases, black stools (melena). Common causes include peptic ulcer disease, esophageal varices, Mallory-Weiss tears, erosive gastritis or esophagitis.**"
Investigations - Urgent Priority
Immediate (same day):
- Full blood count - haemoglobin (anaemia from blood loss), MCV
- Urea and electrolytes - elevated urea:creatinine ratio (>100:1) strongly suggests upper GI bleed (blood protein digestion in gut)
- Coagulation screen - PT, aPTT
- Blood group and crossmatch - if significant bleeding suspected
- Liver function tests - rule out hepatic disease (varices)
- H. pylori testing - urea breath test (gold standard, non-invasive), stool antigen, or rapid urease test at endoscopy
Within 24 hours:
- Upper GI endoscopy (OGD) - MANDATORY for melena. Diagnoses the source, confirms ulcer, allows therapeutic intervention (haemostasis if active bleeding), and biopsies for H. pylori and malignancy (in gastric ulcers)
Management
Immediate
- Establish IV access; resuscitate if haemodynamically compromised (tachycardia, hypotension)
- Stop any NSAIDs immediately
- IV Proton Pump Inhibitor (PPI) - Omeprazole/Pantoprazole 80 mg IV bolus then 8 mg/hour infusion pre-endoscopy (downstages the stigmata of bleeding, reduces need for endoscopic therapy)
- Nil by mouth pending endoscopy
- Admit to hospital
Post-Endoscopy
- Oral high-dose PPI: Omeprazole 40 mg twice daily for 4-8 weeks
- H. pylori eradication if confirmed (standard 14-day triple therapy):
- PPI (e.g., Omeprazole 20 mg BD) + Amoxicillin 1g BD + Clarithromycin 500 mg BD
- Alternatively, bismuth-based quadruple therapy if clarithromycin resistance is suspected
- Confirm eradication 4 weeks after completion of antibiotics (urea breath test or stool antigen - not serology)
- Dietary advice: avoid spicy foods, caffeine, alcohol; eat small regular meals
Important: Confirm eradication
If H. pylori is treated and eradicated, the risk of duodenal ulcer recurrence drops from ~80% to less than 5% at one year.
Clinical Bottom Line
Dark stools in this context = melena = upper GI bleed = urgent investigation. This 23-year-old most likely has a bleeding duodenal ulcer, almost certainly driven by H. pylori infection. The postprandial onset, night pain, and positional features all fit duodenal ulcer. This is not IBS.
Immediate action:
- Admit and assess haemodynamic status
- IV PPI
- Blood tests including U&E, CBC, crossmatch
- Upper GI endoscopy within 24 hours
- Test for and treat H. pylori
Sources: Yamada's Textbook of Gastroenterology 7e; Goldman-Cecil Medicine, International Edition; Harrison's Principles of Internal Medicine 22E (2025); Sleisenger & Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.