Write ETIOPATHOGENESIS, C/F, investigations & management of DIABETIC FOOT
Reading File
Finding Sources
Finding Sources
Searching PubMed
"diabetic foot" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, authoritative content from multiple textbooks to write a thorough clinical answer. Here is the complete write-up:
DIABETIC FOOT
ETIOPATHOGENESIS
Diabetic foot disease arises from the combined and synergistic effects of three main pathological processes: peripheral neuropathy, peripheral vascular disease (macroangiopathy/microangiopathy), and immune dysfunction. The annual incidence of foot complications is 1-2% per year, with a lifetime risk of developing a diabetic foot ulcer (DFU) of ~15%.
1. Peripheral Neuropathy
Neuropathy is the single most important initiating factor. Intracellularly, glucose metabolism pathways become saturated and glucose is converted to sorbitol and fructose via the polyol pathway, impairing ATPase pumps and causing structural axonal breakdown. Excess glucose interacts with intracellular proteins causing glycation; mitochondria increase production of free radicals, causing oxidative damage. The basement membrane of small vessels (vasa nervorum) becomes glycosylated and thickened, producing chronic ischemia of nerve fibers. These processes begin in the smallest unmyelinated fibers and progress to larger nerves.
Three types of nerve dysfunction result:
| Nerve Type | Effect |
|---|---|
| Sensory | Loss of pain, temperature, vibration sensation (glove-and-stocking distribution) - the most critical contributor to ulceration |
| Autonomic | Decreased sweating and skin lubrication → dry, cracked, fissuring skin; decreased blood flow integrity |
| Motor | Intrinsic muscle wasting → claw toes, hammer toes, distal migration of the plantar fat pad; gastrocnemius contracture increases forefoot pressure |
The absence of protective sensation is the pivotal event - patients cannot detect minor injuries, badly fitting footwear, or painful bony prominences. These progress to pressure ulceration undetected. Gait abnormalities follow: increased step width, decreased proprioception, and slower gait increase mechanical stress at pressure points.
2. Peripheral Vascular Disease (Macrovascular + Microvascular)
Macrovascular disease: Glycosylation of the endothelial basement membrane impairs oxygen diffusion. Arteriosclerosis and calcinosis of the arterial wall lead to a narrowed lumen. Hyperlipidemia and atherosclerosis are common co-contributors. In diabetics, PAD primarily affects the tibial and femoral-popliteal distributions. Diabetic patients with PAD are nine times more likely to develop a foot ulcer.
Microvascular disease: Thickening of capillary basement membranes reduces tissue oxygenation and impairs delivery of inflammatory cells essential for wound healing.
These vascular defects mean that once a wound forms, it heals extremely poorly. The ischemic component also predisposes to tissue necrosis and gangrene.
3. Impaired Wound Healing
Normal wound healing requires four stages: hemostasis, inflammation, proliferation, and remodeling. In diabetes:
- Hyperglycemia reduces the function of neutrophils, macrophages, and fibroblasts
- Epigenetic modifications to wound macrophages maintain a persistent pro-inflammatory state, preventing transition to the proliferation/remodeling phase
- Glycation end-products impair chemotaxis of polymorphonuclear cells
- The net result is a chronic non-healing ulcer
4. Immune Dysfunction
Diabetes impairs the chemotaxis of PMNs and causes cell wall abnormalities, making patients highly susceptible to secondary infections. Wounds are predominantly polymicrobial. Gram-positive aerobes (Staphylococcus aureus) are most prevalent; gram-negative bacilli and obligate anaerobes are often also present. Pseudomonas is over-represented. Biofilm formation within chronic wounds further inhibits healing.
5. Mechanical / Biomechanical Factors
Motor neuropathy causes muscle imbalance: weak intrinsics are overpowered by stronger extrinsic muscles, producing hammer toes, claw toes, and distal migration of the plantar fat pad. Gastrocnemius-soleus contracture increases force on the forefoot. These architectural changes create abnormal plantar pressure points that progress to ulceration - particularly at the first and fifth metatarsal heads, the heel, and the great toe. Diabetic tissue has significantly thicker elastic septae and dermal layers, and 46% higher dynamic midfoot joint pressures compared to non-diabetic tissue.
CLINICAL FEATURES (C/F)
History
- Long-standing diabetes mellitus (often Type 2)
- Patient may not recall the specific injury - sensory neuropathy blunts pain
- Prior episodes of ulceration, prior amputations
- Symptoms of peripheral neuropathy: numbness, paresthesias, burning pain (feet and lower legs)
- Claudication or rest pain (if significant PAD)
- Visual impairment (retinopathy) - impairs daily foot inspection
General Examination
- Evidence of poor glycemic control
- Peripheral edema, hypertension
Local Foot Examination
Skin & Soft Tissue:
- Dry, scaly skin; fissuring (autonomic dysfunction)
- Shiny, taut, hairless skin (PAD)
- Callus formation overlying pressure points
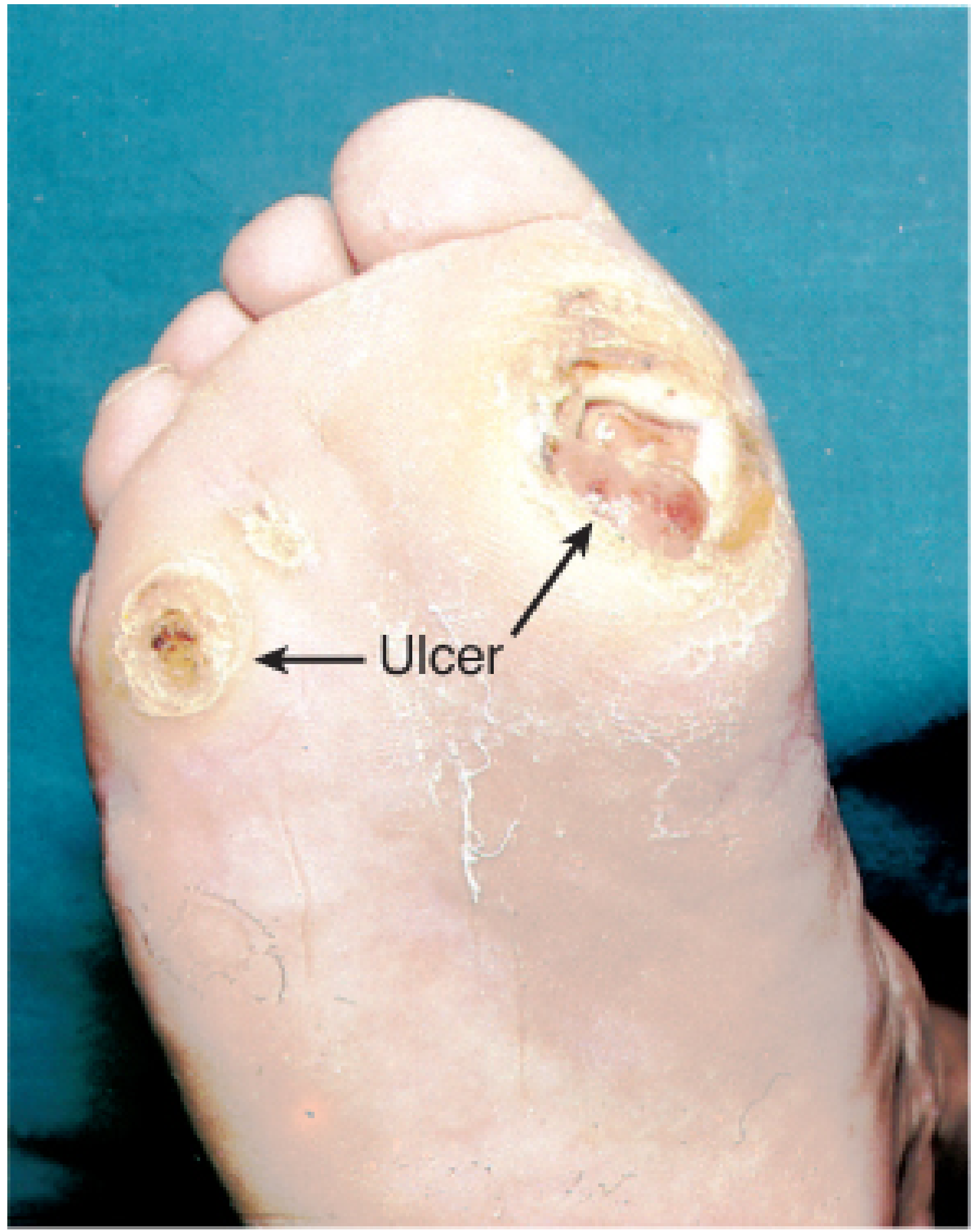
- Plantar ulcers - typically painless, pink/punched-out edges, surrounded by callus, located at metatarsal heads, heel, or inter-digital spaces (neuropathic ulcers)
- Ischemic ulcers may appear at toe tips with pale, pale wound beds
Deformities:
- Claw toes, hammer toes, pes cavus (motor neuropathy)
- Charcot neuroarthropathy: acute erythema + warmth + swelling of the foot, often mimicking infection; the "rocker bottom" deformity in late stages; distinguishes from infection by subsiding with elevation
Vascular Signs:
- Absent or diminished dorsalis pedis and posterior tibial pulses
- Prolonged capillary refill time
- Dependent rubor, pallor on elevation
Neurological Signs:
- Reduced or absent vibration sense (128 Hz tuning fork)
- Loss of proprioception
- Inability to feel 5.07 Semmes-Weinstein monofilament (10 g) - most predictive risk factor for foot morbidity
- Absent ankle reflexes
Signs of Infection:
- Cellulitis, erythema, warmth, induration
- Purulent discharge from ulcer
- Crepitus (gas-forming organisms)
- Spreading lymphangitis
- Systemic signs: fever, tachycardia, hypotension, altered mental status (pedal sepsis = surgical emergency)

ULCER CLASSIFICATION
Wagner Classification (most widely used)
| Grade | Description |
|---|---|
| 0 | Skin intact but at risk (callus, bony deformity) |
| I | Superficial ulcer - skin broken but no subcutaneous involvement |
| II | Deep ulcer - exposed tendon, joint capsule, or deep structures |
| III | Deep ulcer with abscess, osteomyelitis, or joint infection |
| IV | Partial gangrene (forefoot / toe) |
| V | More extensive/whole foot gangrene |
Brodsky Depth-Ischemia Classification
| Depth | Description | Ischemia | Description |
|---|---|---|---|
| 0 | At-risk foot, no ulceration | A | Not ischemic |
| 1 | Superficial ulceration, no infection | B | Ischemia without gangrene |
| 2 | Deep ulceration, tendons/joints exposed | C | Partial forefoot gangrene |
| 3 | Extensive ulceration or abscess | D | Complete foot gangrene |
Key point: Ulcers that are both infected and ischemic are 90 times more likely to require amputation. An infected ulcer alone carries a 40-55% chance of some form of amputation. - Campbell's Operative Orthopaedics, 15e
INVESTIGATIONS
Bedside / Clinical Tests
- Semmes-Weinstein 5.07 (10-g) monofilament - gold standard for screening protective sensation loss; 10 sites tested on the foot
- 128 Hz tuning fork - vibration sense assessment
- Probe-to-bone test - positive (bone felt on probing) has 57% PPV for osteomyelitis, 96% NPV; combined with raised inflammatory markers and abnormal X-ray, confirms the diagnosis
Laboratory Investigations
| Investigation | Purpose |
|---|---|
| Blood glucose / HbA1c | HbA1c >7% is independent risk factor for DFU; HbA1c >8% = poor prognosis |
| CBC (FBC) | Leucocytosis (infection); anaemia |
| ESR, CRP | Elevated supports osteomyelitis; note - often normal/mildly raised even in significant infection |
| Blood cultures | If systemic sepsis |
| Renal function (urea, creatinine) | Diabetic nephropathy co-assessment |
| Serum albumin | Nutritional status - hypoalbuminaemia impairs healing |
| Wound swab / deep tissue culture | Guide antibiotic therapy; surface swabs are unreliable for deep infection |
| Bone biopsy culture | Gold standard for identifying organisms in osteomyelitis; provides antibiotic sensitivity |
Vascular Investigations
| Test | Normal | Interpretation |
|---|---|---|
| Ankle Brachial Index (ABI) | 0.9 - 1.2 | <0.5 = unlikely to heal without revascularisation; >1.3 = non-compressible vessels (calcification) |
| Toe Brachial Index (TBI) | >0.7 | >0.4 or toe pressure >40 mmHg = adequate perfusion; preferred in diabetics with calcified vessels |
| Ankle systolic pressure | >90 mmHg needed for healing in diabetics | |
| Duplex USS / Doppler | Assess dorsalis pedis and posterior tibial signals | |
| Digital subtraction angiography | Assessment of infrageniculate circulation prior to revascularisation | |
| CT angiography | Evaluation of aorta, iliac, and femoral arteries |
Imaging
Plain Radiographs (X-ray):
- First-line, widely available
- Findings: demineralisation, loss of trabecular pattern, periosteal reaction, joint destruction, soft-tissue gas (gas-producing organisms), foreign bodies
- Limitation: early osteomyelitis is NOT visible on X-ray - takes weeks to months before changes appear
MRI (Magnetic Resonance Imaging):
- Most sensitive and specific imaging modality for osteomyelitis
- Distinguishes soft tissue infection from bone involvement and Charcot neuroarthropathy
- T1 shows bone marrow replacement; STIR shows oedema
- Preferred when clinically suspected osteomyelitis with normal/equivocal X-rays
- Limitations: scheduling delays, cost, metal implants
CT Scan:
- Useful for bone architecture detail in multiple planes
- Detects subtle cortical disruptions, sequestra, involucrum
- Good for assessing aorta/iliac/femoral vessels in PAD evaluation
Bone Scan (Technetium-99m):
- High sensitivity but low specificity (positive in any cause of increased bone turnover)
- Useful when MRI is unavailable
Tagged White Blood Cell (WBC) Scan (In-111 or Tc-99m HMPAO):
- More specific for osteomyelitis than bone scan
- Helps differentiate Charcot from infection when MRI is equivocal
Ultrasound:
- Detects soft tissue collections, abscesses, and fluid
- Guides aspiration
MANAGEMENT
Management is multidisciplinary - involving diabetologist, vascular surgeon, orthopaedic/podiatric surgeon, infectious disease specialist, wound care nurse, dietitian, and physiotherapist.
A. Glycaemic Control
- Target HbA1c <7%
- Tight glucose control halts progression of neuropathy; prolonged good control can partially reverse it
- Pre-operative glucose <200 mg/dL to minimise surgical complications
- ACE inhibitor for hypertension; statin for dyslipidaemia; aspirin for PAD
B. Prevention (Cornerstone of Treatment)
- Routine foot examination at every clinic visit; daily self-inspection for cuts, fissures, ulcers, callus
- Never walk barefoot; wear well-cushioned protective footwear (avoid sandals)
- Avoid heating pads/hot water bottles on feet (thermal burns)
- Professional toenail trimming
- Callus reduction by podiatrist to unroof occult ulcers
- Regular moisturising of dry skin
- Tobacco cessation
C. Wound Care & Off-loading
Off-loading (most important therapeutic intervention for neuropathic ulcers):
- Total contact cast (TCC) - gold standard for off-loading; extends above ankle, reduces plantar pressure by up to 60%; non-removable so patient compliance guaranteed
- Fixed ankle walking boot / Removable walker boot - alternative when frequent dressing changes are needed
- Custom orthotics / therapeutic footwear once healed
Wound Dressings:
- Moist wound environment is the goal (saline- or Vaseline-impregnated gauze changed daily or twice daily)
- Silver-impregnated dressings for infection control
- Foam/cushioning dressings for pressure protection
- Wet-to-dry dressings: classic non-surgical debridement method
Debridement:
- Required when proteinaceous eschar or necrotic tissue inhibits healing
- Methods: wet-to-dry dressings, topical enzymatic debridement, surgical debridement
- Negative pressure wound therapy (VAC therapy): sponge applied to wound and placed on vacuum suction, changed 2-3x/week; promotes angiogenesis, accelerates granulation tissue, decreases healing time; infusion-VAC can deliver local antibiotics
- Medical maggot therapy: selective debridement of non-viable tissue; effective but limited by patient/provider acceptance
- Platelet-derived growth factor (PDGF): topical application for wounds failing other therapies - data supports use
Hyperbaric Oxygen Therapy (HBO):
- Increases tissue oxygenation by delivering oxygen-rich plasma
- Promotes angiogenesis within the wound bed
- Best candidates: good perfusion (palpable pulses, normal TBI)
- Multiple treatment sessions required (weeks of therapy)
Bioengineered Skin Substitutes: Used for non-healing ulcers; evidence is evolving.
D. Antibiotic Therapy
| Severity | Organisms | Treatment |
|---|---|---|
| Mild (superficial, localised) | Gram-positive cocci (S. aureus, Streptococci) | PO: TMP-SMX 800/160 mg BD, or cephalexin 500 mg QID, or clindamycin 300 mg QID |
| Moderate-Severe (deep, spreading cellulitis >2 cm, lymphangitis, systemic toxicity) | Polymicrobial: aerobes + anaerobes + Gram-negatives including Pseudomonas | IV: Piperacillin-tazobactam 3.375 g q8h + Vancomycin 15 mg/kg q12h |
| Osteomyelitis | Same + anaerobes | 6 weeks IV antibiotics after bone biopsy culture; surgery often needed |
| Anaerobes / Devitalised tissue | Add metronidazole |
- Surface wound swabs are not reliable - they do not reflect deep infection organisms
- Bone biopsy culture is the gold standard and guides targeted therapy
- MRSA cover (vancomycin/linezolid) should be included in severe infections
E. Surgical Management
Debridement:
- Required for collections, necrotic areas, or osteomyelitis
- All non-viable tissue debrided at initial operation
- Wounds generally left open to drain and heal by secondary intention
Incision & Drainage:
- For deep-space abscess; explore for extensions and bony involvement
Pressure-Relieving Surgery:
- Metatarsal head resection - reduces abnormal pressure and ulcer recurrence
- Achilles tendon lengthening - reduces forefoot pressure
- Arthroplasty/osteotomy - correction of structural deformity
Osteomyelitis:
- Superficial osteitis (periosteal only) may not require bone resection
- True osteomyelitis with cortical involvement requires resection of affected bone
- In good perfusion with limited disease: prolonged IV antibiotics may be considered
- Extensive osteomyelitis may require amputation
F. Revascularisation
- Mandatory assessment with ABI/TBI in all patients with poor pulses or non-healing wounds
- ABI >1.3 → non-compressible → use TBI instead
- ABI <0.5 or toe pressure <40 mmHg → refer to vascular surgery
- Revascularisation should precede debridement/amputation when not in septic emergency, to limit resection of ischaemic but potentially viable tissue
- Methods: angioplasty (endovascular, preferred), femoral-popliteal or tibial bypass (open)
- In distal tissue loss, pulsatile in-line flow to the foot must be restored
- Digital subtraction angiography remains the gold standard for infrageniculate assessment
G. Amputation
- Last resort, but often necessary
- Minor amputations: toe, ray (toe + metatarsal) resection
- Major amputations: below-knee (BKA) - preferred for maximal rehabilitation; above-knee (AKA) - reserved for extensive disease
- Wound healing after amputation is unreliable due to neuropathy and vascular compromise
- SVS WIfI classification (Wound, Ischemia, Foot Infection) is used to estimate benefit of revascularisation and risk of amputation
- Excess bone resected to allow tension-free skin closure; consider BKA over ray amputation if extensive peripheral neuropathy is present
H. Treatment of Charcot Neuroarthropathy
- Total contact casting in acute phase
- Elevation (distinguishes from infection - Charcot subsides with elevation)
- No weight bearing until acute inflammation resolves
- Surgical reconstruction for severe deformity causing recurrent ulceration
PROGNOSIS
- 5-year mortality of diabetic foot complications is comparable to many cancers (30.5% for DFU)
- Ulcers <1 cm² - 96% eventually heal without amputation
- Ulcers >3 cm² - only 72% heal without amputation
- Infected + ischaemic ulcers: 90x more likely to require amputation
- Up to one-third of patients with deep infections eventually undergo amputation
Sources: Fischer's Mastery of Surgery (8e), Campbell's Operative Orthopaedics (15e 2026), Bailey & Love's Short Practice of Surgery (28e), Goldman-Cecil Medicine, Rosen's Emergency Medicine.Recent evidence note: A 2024 systematic review (PMID 39241769) confirms negative pressure wound therapy (NPWT/VAC) significantly improves healing rates in DFUs compared to standard care (RCT-level evidence). Smart wearable technology for pressure monitoring shows promise for prevention (PMID 40682082, 2025 systematic review).
This is a shared conversation. Sign in to Orris to start your own chat.