Thyrotoxicosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
thyrotoxicosis management
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material from multiple authoritative sources. Let me compile the full answer.
Thyrotoxicosis
Definition
Thyrotoxicosis is a clinicopathologic and biochemical syndrome resulting from exposure to excessive concentrations of thyroid hormones. It is categorized as:
- Overt thyrotoxicosis - elevated T4/T3 + suppressed TSH; most patients are symptomatic
- Subclinical thyrotoxicosis - normal T4/T3 + low TSH; most patients asymptomatic
- T3 thyrotoxicosis - elevated T3 but normal T4 (more common in iodine-deficient regions and in toxic adenoma/recurrent Graves)
- Cummings Otolaryngology Head and Neck Surgery
Causes / Etiology
Thyrotoxicosis WITH Hyperthyroidism (increased production)
| Cause | Notes |
|---|---|
| Graves disease | 60-85% of all cases; most common |
| Toxic multinodular goiter (Plummer disease) | 10-30% of cases |
| Toxic thyroid adenoma | 2-20% of cases |
| TSH-secreting pituitary adenoma | Rare; secondary hyperthyroidism |
| Gestational thyrotoxicosis / hCG-mediated | First trimester; hCG stimulates TSH receptors |
| Trophoblastic tumors | hCG-mediated |
| McCune-Albright syndrome | Activating mutation of Gs-alpha |
| Struma ovarii | Ectopic thyroid tissue |
| Jod-Basedow phenomenon | Iodine excess in susceptible individuals |
Thyrotoxicosis WITHOUT Hyperthyroidism (release from destroyed tissue)
- Subacute (de Quervain) thyroiditis
- Silent (painless) thyroiditis, postpartum thyroiditis
- Drug-induced thyroid destruction: amiodarone, cytokines, tyrosine kinase inhibitors, immune checkpoint inhibitors (nivolumab, pembrolizumab)
- Radiation thyroiditis
- Factitious thyrotoxicosis (exogenous ingestion)
- Harrison's Principles of Internal Medicine 22E (2025)
Epidemiology
- Overall prevalence: ~0.5-1 per 1,000 in the USA
- 10 times more common in women than men
- Graves disease: peak age 30-60 years
- Toxic multinodular goiter/adenoma: age 40-70 years, higher in iodine-deficient areas
- Cummings Otolaryngology Head and Neck Surgery
Pathophysiology
Thyrotoxicosis results from unregulated release of T4 and T3, either through:
- Increased synthesis (TSH receptor stimulation by antibodies, autonomous nodules)
- Destruction of thyroid tissue releasing stored hormone
- Exogenous ingestion
Thyroid hormones have a direct stimulatory effect on cardiac muscle - heart rate and output increase, peripheral vascular resistance falls, and cardiac oxygen demand rises. Despite mimicking a hyperadrenergic state, catecholamine levels are normal; beta-blockers work by blocking downstream adrenergic effects, particularly of T3.
- Tietz Textbook of Laboratory Medicine 7e
Clinical Features
Symptoms (in descending order of frequency)
- Hyperactivity, irritability, dysphoria
- Heat intolerance and sweating
- Palpitations
- Fatigue and weakness
- Weight loss with increased appetite (weight gain in 5% due to hyperphagia)
- Diarrhea / increased stool frequency
- Polyuria
- Oligomenorrhea, loss of libido
- Fine tremor (best elicited at fingertips)
- Insomnia, impaired concentration
Signs
- Tachycardia (most common cardiovascular sign); atrial fibrillation especially in elderly
- Goiter
- Warm, moist skin; palmar erythema; onycholysis
- Proximal myopathy (without fasciculations)
- Lid retraction / lid lag
- Fine tremor
- Diffuse alopecia (up to 40%)
- Bounding pulse, widened pulse pressure
- Gynecomastia (males)
- Hyperreflexia
Apathetic (elderly) presentation
The elderly may present with fatigue and weight loss only, without the typical hyperadrenergic features - easily mistaken for depression or malignancy.
Cardiovascular complications
These carry the highest morbidity and mortality of all manifestations:
- Sinus tachycardia → supraventricular tachycardia → atrial fibrillation
- Systolic hypertension, widened pulse pressure
- High-output cardiac failure (in elderly or pre-existing cardiac disease)
- Worsening angina
- Osteoporosis, mild hypercalcemia (in up to 20%), fractures
- Harrison's Principles of Internal Medicine 22E (2025); Tietz Textbook of Laboratory Medicine 7e
Graves Disease - Specific Features
Graves disease is the most common cause, accounting for 60-85% of cases. It is an autoimmune disorder driven by TSH receptor-stimulating autoantibodies (TSI / TRAb).
Pathogenesis:
- TSI (IgG) binds and activates TSH receptors on follicular cells → continuous T4/T3 production independent of TSH
- Pituitary feedback loop is bypassed → TSH becomes profoundly suppressed (<0.01 mIU/L)
- TPO and Tg antibodies also present in up to 80%
- Genetic associations: HLA alleles, CTLA4
Unique features (not seen in other causes):
- Ophthalmopathy (exophthalmos/proptosis) - TSH receptors expressed on orbital fibroblasts; activated T cells release IFN-γ, TNF, IL-1 → glycosaminoglycan accumulation → muscle swelling, increased retro-orbital fat → proptosis, diplopia, corneal injury, optic neuropathy
- Pretibial myxedema (dermopathy) - scaly thickening/induration of skin over shins; glycosaminoglycan deposition
- Thyroid acropachy - rare periosteal reaction of digits/toes
- Diffuse goiter (>90% of patients) - symmetrically enlarged, soft, bruit audible over gland
- Thyroid bruit - increased blood flow
Histology (Robbins): Follicular hyperplasia and hypertrophy, small papillae lacking fibrovascular cores projecting into lumen, pale scalloped colloid, lymphoid infiltrates with germinal centers.
- Robbins & Kumar Basic Pathology; Harrison's 22E; Textbook of Family Medicine 9e
Diagnosis
Laboratory Tests
| Test | Finding |
|---|---|
| Serum TSH | Suppressed (<0.01 µU/mL) - most sensitive test; normal TSH excludes hyperthyroidism |
| Free T4 | Elevated (overt); normal (subclinical) |
| Free T3 | Elevated; T3 rises disproportionately more than T4 |
| TRAb / TSI | Positive in Graves disease |
| TPO antibodies | Present in Graves and Hashimoto |
Imaging
- Radioiodine uptake (RAIU) scan with 123I: differentiates causes - diffuse uptake (Graves) vs. hot nodule (toxic adenoma) vs. cold scan (thyroiditis)
- Thyroid ultrasound: goiter size, nodules
- Textbook of Family Medicine 9e; Rosen's Emergency Medicine
Treatment
1. Symptomatic / Immediate Control
- Beta-blockers (propranolol 20-40 mg q6h, or long-acting atenolol): first-line for symptomatic relief - controls tachycardia, tremor, anxiety, heat intolerance; also blocks T4→T3 peripheral conversion (at high doses of propranolol)
- Anticoagulation: consider for all patients with atrial fibrillation (CHA2DS2-VASc score); majority revert to sinus rhythm with treatment of thyrotoxicosis
2. Antithyroid Drugs (ATDs)
- Methimazole (MMI): preferred in most patients; blocks thyroid peroxidase → inhibits thyroid hormone synthesis
- Propylthiouracil (PTU): preferred in first trimester of pregnancy (MMI associated with embryopathy); also blocks peripheral T4→T3 conversion
- Dosing for storm: PTU 500-1000 mg loading, then 250 mg q4h; MMI 60-80 mg/day
- Side effects: Rash, urticaria, fever, arthralgia (1-5%); agranulocytosis (<1%, abrupt onset - warn patients about sore throat/fever); hepatitis (PTU - avoid in children)
3. Radioiodine (131I) Ablation
- Progressive destruction of thyroid cells
- Treatment of choice for toxic multinodular goiter and toxic adenoma
- For Graves: widely used after ATD control; dose 370-555 MBq (10-15 mCi)
- Absolutely contraindicated in pregnancy
- Pre-treat with ATD for ≥1 month to prevent thyrotoxic crisis post-RAI; stop methimazole 2-3 days before; restart 3-7 days after if at risk
- Most patients ultimately develop hypothyroidism and require lifelong T4 replacement
4. Surgery (Total/Near-Total Thyroidectomy)
- Indicated for large goiters, suspected malignancy, ophthalmopathy, pregnancy (after first trimester if ATDs fail), patient preference
- Requires pre-operative ATD to achieve euthyroid state
- Complications: hypoparathyroidism, recurrent laryngeal nerve injury
- Harrison's 22E; Textbook of Family Medicine 9e; Cummings Otolaryngology
Thyroid Storm (Thyrotoxic Crisis)
A rare, life-threatening emergency. Untreated mortality approaches 100%; with treatment, mortality is 10-30%. Death results from multiorgan dysfunction, CHF, arrhythmias, DIC, or sepsis.
Precipitants
Surgery, trauma, infection, iodine load, parturition, RAI treatment, ATD discontinuation, MI, PE, DKA, hyperemesis gravidarum
Clinical Features
- Marked pyrexia: 104-106°F (40-41°C)
- Extreme tachycardia (disproportionate to fever)
- Altered mental status: agitation → delirium → psychosis → coma
- Cardiovascular collapse: CHF, hypotension, AF
- GI: nausea, vomiting, diarrhea, abdominal pain; hepatic failure (poor prognosis)
Burch-Wartofsky Score (1993) - Scoring for Thyroid Storm Diagnosis
| Category | Score |
|---|---|
| Fever ≥104°F | 30 |
| Tachycardia ≥140 | 25 |
| Mental status: coma/seizures | 30 |
| CHF: pulmonary edema | 15 |
| Atrial fibrillation | 10 |
| GI symptoms: jaundice | 20 |
| Precipitating event present | 10 |
Score ≥45: thyroid storm; <25: unlikely storm
Treatment of Thyroid Storm (order matters - iodine MUST follow thionamide by ≥1 hour)
| Step | Drug | Dose |
|---|---|---|
| 1. Beta-blockade | Propranolol | 60-80 mg PO q4h; or 0.5-1 mg IV then 1-2 mg q15 min; Esmolol 50-100 µg/kg/min infusion |
| 2. Inhibit synthesis | PTU | 500-1,000 mg loading, then 250 mg q4h |
| Methimazole | 60-80 mg/day in divided doses | |
| 3. Inhibit release (≥1 h after step 2) | SSKI | 1-2 drops PO/PR tid (50 mg iodide/drop) |
| Lugol solution | 5-7 drops tid (8 mg iodide/drop) | |
| If iodine allergy | Lithium carbonate 300 mg PO qid | |
| 4. Steroids | Hydrocortisone | 300 mg IV loading, then 100 mg tid |
| Dexamethasone | 2-4 mg IV qid | |
| 5. Supportive | IVF (D5/0.9 NS), acetaminophen (not ASA - displaces T4 from TBG), cooling blankets, treat precipitant | |
| 6. Other | Cholestyramine 1-4 g bid (blocks enterohepatic recirculation) |
- Rosen's Emergency Medicine; Cummings Otolaryngology Head and Neck Surgery
Special Situations
Pregnancy
- PTU preferred in first trimester (methimazole associated with aplasia cutis, choanal atresia)
- Switch to methimazole in 2nd/3rd trimester (PTU hepatotoxicity risk)
- High maternal TSI can cross placenta → neonatal thyrotoxicosis; TRAb levels should be monitored
- RAI absolutely contraindicated
- Graves disease has 3x higher relapse rate postpartum
Subclinical Thyrotoxicosis
- Treat if: TSH <0.1 mIU/L with age >65, cardiac disease, osteoporosis, or symptoms; or TSH persistently suppressed
- Observe with close monitoring if TSH 0.1-0.4 mIU/L and asymptomatic
Atrial Fibrillation
- Occurs in 10-20% of thyrotoxic patients, more common >50 years
- Up to 75% revert to sinus rhythm with treatment of thyrotoxicosis alone
- Warfarin dose requirements are decreased in thyrotoxic state
- Digoxin doses need to be increased (increased clearance)
Recent Evidence (2025-2026)
A 2024 systematic review on perioperative thyrotoxicosis management (PMID: 39722810) addressed management when standard therapy is contraindicated or fails - relevant for complex surgical patients. A 2026 systematic review on autoimmune thyroid diseases post-COVID-19 (PMID: 42354220) documents new-onset Graves disease and thyrotoxicosis as COVID-19 sequelae, adding immune checkpoint disruption as an emerging cause.
Diabeties milletus DM-2 D. Keto acidosis Non pharmacological management of insulin Types of insulin New insulin
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
insulin analogues new formulations diabetes
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading Article
PMID: 40156735
Reading File
Reading File
Reading Article
PMID: 39911031
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Diabetes Mellitus - Comprehensive Notes
1. Diabetes Mellitus - Overview
Diabetes mellitus (DM) is a group of metabolic diseases characterized by chronic hyperglycemia resulting from defects in insulin secretion, insulin action, or both. Chronic hyperglycemia leads to long-term damage, dysfunction, and failure of various organs.
Diagnostic Criteria (ADA)
| Test | Diabetes | Prediabetes |
|---|---|---|
| Fasting Plasma Glucose | ≥126 mg/dL | 100-125 mg/dL (IFG) |
| 2-hour OGTT (75g) | ≥200 mg/dL | 140-199 mg/dL (IGT) |
| HbA1c | ≥6.5% | 5.7-6.4% |
| Random glucose + symptoms | ≥200 mg/dL | - |
Glycemic Targets (ADA 2024)
| Parameter | Goal |
|---|---|
| HbA1c | <7.0% |
| Preprandial glucose | 80-130 mg/dL (4.4-7.2 mmol/L) |
| Peak postprandial glucose | <180 mg/dL (<10.0 mmol/L) |
| Time-in-range (CGM) | >70% (3.9-10.0 mmol/L) |
- Goodman & Gilman's Pharmacological Basis of Therapeutics; Harrison's 22E (2025)
2. Type 2 Diabetes Mellitus (T2DM)
Pathophysiology - The "Ominous Octet" (DeFronzo)
T2DM results from progressive insulin resistance combined with relative insulin secretory deficiency. Key mechanisms:
- Insulin resistance - skeletal muscle, liver, adipose tissue
- Beta-cell failure - progressive, irreversible over time
- Increased hepatic glucose production (fasting hyperglycemia)
- Impaired incretin effect - reduced GIP/GLP-1 activity
- Alpha-cell hypersecretion of glucagon
- Increased renal glucose reabsorption (raised renal threshold)
- Increased lipolysis - elevated free fatty acids worsen insulin resistance
- Neurotransmitter dysfunction - central appetite dysregulation
Risk Factors
- Obesity (especially central/visceral adiposity)
- Family history (strong genetic component)
- Physical inactivity
- Age >45 years
- Dyslipidemia (low HDL, high triglycerides)
- Hypertension
- Prior gestational diabetes
- Polycystic ovary syndrome (PCOS)
- Ethnicity (South Asian, African, Hispanic)
Clinical Features
- Often asymptomatic for years (insidious onset)
- Polyuria, polydipsia, polyphagia
- Fatigue, blurred vision
- Recurrent infections (candidal, UTIs, skin)
- Acanthosis nigricans (insulin resistance marker)
- Peripheral neuropathy / foot ulcers may be first presentation
- No ketoacidosis typically (residual insulin prevents lipolysis)
Natural History
T2DM is a progressive disorder - most patients ultimately require multiple agents and eventually insulin. Any therapy that improves glycemic control reduces "glucose toxicity" to beta cells and may improve endogenous insulin secretion.
Pharmacological Treatment Summary
| Class | Mechanism | Key Drug | Notes |
|---|---|---|---|
| Biguanides | ↓ hepatic glucose production | Metformin | First-line; max 2000 mg/day |
| Sulfonylureas | ↑ insulin secretion (ATP-K channel) | Glipizide, Glimepiride | Hypoglycemia risk |
| GLP-1 RAs | Incretin mimic | Semaglutide, Liraglutide | Weight loss, CV benefit |
| SGLT2 inhibitors | ↑ urinary glucose excretion | Empagliflozin, Dapagliflozin | CV + renal benefit |
| DPP-4 inhibitors | Prolong incretin effect | Sitagliptin | Weight neutral |
| Thiazolidinediones | ↑ insulin sensitivity (PPARγ) | Pioglitazone | Weight gain, edema |
| Meglitinides | ↑ insulin secretion (short) | Repaglinide | Postprandial |
| Insulin | Direct insulin replacement | Various | Progressive disease |
- Harrison's Principles of Internal Medicine 22E (2025)
3. Diabetic Ketoacidosis (DKA)
Definition
DKA is an acute, life-threatening complication defined by the triad:
- D = Hyperglycemia (glucose ≥250 mg/dL) - or history of diabetes
- K = Ketonemia (β-hydroxybutyrate ≥3.0 mmol/L) or ketonuria ≥2+
- A = Acidosis (arterial/venous pH <7.3)
Note: Euglycemic DKA (glucose <200 mg/dL) occurs in: pregnancy, alcohol ingestion, fasting, SGLT2 inhibitor use.
Pathophysiology
Insulin deficiency + excess counter-regulatory hormones (glucagon, cortisol, catecholamines, GH) →
- Liver: Substrates (amino acids, lactate, free fatty acids, glycerol) delivered → glucose and ketone bodies (β-hydroxybutyrate, acetoacetate, acetone) released into circulation faster than utilization
- Adipose: Unrestrained lipolysis → free fatty acids → ketogenesis
- Osmotic diuresis: Hyperglycemia → dehydration, electrolyte loss → hemoconcentration → worsens hyperglycemia
DKA vs HHS
| Feature | DKA | Hyperosmolar Hyperglycemic State (HHS) |
|---|---|---|
| Glucose | ≥250 mg/dL | Often >600 mg/dL |
| pH | <7.3 | Usually >7.3 |
| Ketones | +++ | Absent/minimal |
| Bicarbonate | <18 mEq/L | Usually normal |
| Anion gap | Elevated | Normal or mildly elevated |
| Onset | Rapid (hours) | Slow (days) |
| Typical patient | T1DM (young) | Elderly T2DM |
Precipitants of DKA
Most common:
- Infections (most frequent - UTI, pneumonia)
- Inadequate insulin or non-adherence
- New-onset diabetes
- Acute coronary syndrome
Other precipitants:
- Cerebrovascular accident, pulmonary embolism
- Acute pancreatitis, alcohol intoxication
- Endocrinopathies: Cushing, thyrotoxicosis, acromegaly
- Drugs: Corticosteroids, SGLT2 inhibitors, clozapine, olanzapine, cocaine, thiazides
DKA Classification
| Mild | Moderate | Severe | |
|---|---|---|---|
| Glucose (mg/dL) | >250 | >250 | >250 |
| pH | 7.25-7.3 | 7.0-7.24 | <7.0 |
| Bicarbonate | 15-18 | 10-15 | <10 |
| Ketones | Positive | Positive | Positive |
| Mental status | Alert | Alert/drowsy | Stupor/coma |
Treatment of DKA
Priorities: Fluids first → Insulin → Potassium replacement
Step 1 - IV Fluid Resuscitation
- 0.9% Normal saline: 1 L bolus, then 500-1000 mL/h (to restore circulating volume)
- Switch to 0.45% saline (150-500 mL/h) once hemodynamics stable
- Aim for positive fluid balance over 12-24 h; no faster than 3 mOsm/kg/h
- Total-body water deficit is usually 7-9% body weight
- When glucose reaches 200 mg/dL → add Dextrose 5% to prevent hypoglycemia while continuing insulin
Step 2 - Insulin
Goal: turn off ketogenesis; correct hyperglycemia
- Regular insulin IV infusion: 0.1 units/kg/h (standard) or 0.05 units/kg/h (in hypokalemia)
- Some protocols: 0.1 units/kg IV bolus, then 0.1 units/kg/h infusion
- Target glucose reduction: 50-70 mg/dL/hour
- Switch to subcutaneous insulin when: pH >7.3, bicarbonate >18, patient eating, anion gap closed
- Do NOT stop insulin until ketoacidosis is fully resolved (even if glucose is normal)
- Continuous infusion of regular or short-acting insulin (lispro/aspart) allows frequent adjustment
Step 3 - Potassium Replacement
| Serum K+ | Action |
|---|---|
| <3.3 mEq/L | Hold insulin; replace K+ at 40 mEq/h until ≥3.5 |
| 3.3-5.5 mEq/L | Add 20-40 mEq K+ per liter IV fluid |
| >5.5 mEq/L | Monitor K+ every 2 hours; no supplementation |
Rationale: Insulin drives K+ into cells → hypokalemia risk → cardiac arrhythmia
Other Measures
- Bicarbonate: NOT routinely given; only if pH <6.9 (50 mEq NaHCO3 over 1 hour)
- Phosphate: Not routinely supplemented
- ECG: Obtain to evaluate electrolyte abnormalities and rule out ACS (a precipitant)
- Search for and treat precipitating cause (broad-spectrum antibiotics if infection suspected)
- ICU monitoring preferred; non-ICU for mild-moderate DKA with close monitoring
- The Washington Manual of Medical Therapeutics; Goldman-Cecil Medicine; Creasy & Resnik's Maternal-Fetal Medicine
4. Non-Pharmacological Management of Diabetes
These form the foundation of all diabetes management - for both T1DM and T2DM.
A. Medical Nutrition Therapy (MNT)
General Principles (ADA 2024):
- Emphasis on high-quality, nutrient-dense foods
- Individualized - consider personal, cultural, religious preferences
Carbohydrates:
- Monitor carbohydrate intake to reduce postprandial glycemia
- Avoid fructose- and sucrose-containing beverages
- Minimize foods with added sugar
- Use glycemic index to predict postprandial glucose impact
- Carbohydrate counting for insulin dosing (1 unit per 10-15g carbohydrate)
Fats:
- Mediterranean-style diet (monounsaturated and polyunsaturated fats)
- Minimal/no trans fats
Protein:
- Optimal percentage individualized
Other dietary points:
- Sodium <2,300 mg/day
- Minimize sleep disruption (shift work and sleep deprivation increase insulin resistance)
- Religious fasting (Ramadan) - risk-stratify; close monitoring required
- Reduced-calorie sweeteners may be useful; routine vitamin supplements are not evidence-based
B. Physical Activity / Exercise
ADA Recommendation:
- 150 min/week of moderate aerobic activity, distributed over at least 3 days
- No gaps longer than 2 consecutive days
- Plus: Resistance training, flexibility, balance training
- Reduce sedentary behavior throughout the day
Benefits:
- Lowers plasma glucose (during and after exercise)
- Increases insulin sensitivity
- Cardiovascular risk reduction
- Reduced blood pressure
- Maintenance of muscle mass, reduction in body fat
- Weight loss
Exercise precautions in T1DM:
- Monitor glucose before, during, and after exercise
- Delay exercise if glucose >250 mg/dL with ketones present
- Ingest carbohydrate if glucose <90 mg/dL before exercising
- Reduce insulin doses before/after exercise
- Inject insulin into a non-exercising area
- Untreated proliferative retinopathy = relative contraindication (risk of vitreous hemorrhage)
C. Weight Management
- Weight loss of even 5-10% body weight significantly improves glycemic control in T2DM
- Caloric restriction + exercise
- Very low calorie diets / bariatric surgery in selected obese patients
D. Self-Monitoring of Blood Glucose (SMBG) / Continuous Glucose Monitoring (CGM)
- CGM: provides real-time glucose data, time-in-range, and trends
- "Smart" pens record and report insulin injection data
- Closed-loop (artificial pancreas) systems: CGM + pump; automate insulin delivery
E. Psychosocial Care
- Patient should be an active member of the diabetes care team
- Screen for depression, anxiety, "diabetes distress"
- Address eating disorders (binge eating, bulimia, anorexia - more common in DM)
- Emotional stress disrupts adherence to diet, exercise, and medications
- Mental health specialist referral if needed
F. Smoking Cessation
- Smoking worsens insulin resistance, accelerates cardiovascular disease and nephropathy
G. Foot Care Education
- Daily inspection, proper footwear, podiatry referral
- Critical for preventing ulceration and amputation
- Harrison's Principles of Internal Medicine 22E (2025)
5. Types of Insulin
Molecular Structure of Insulin Analogues
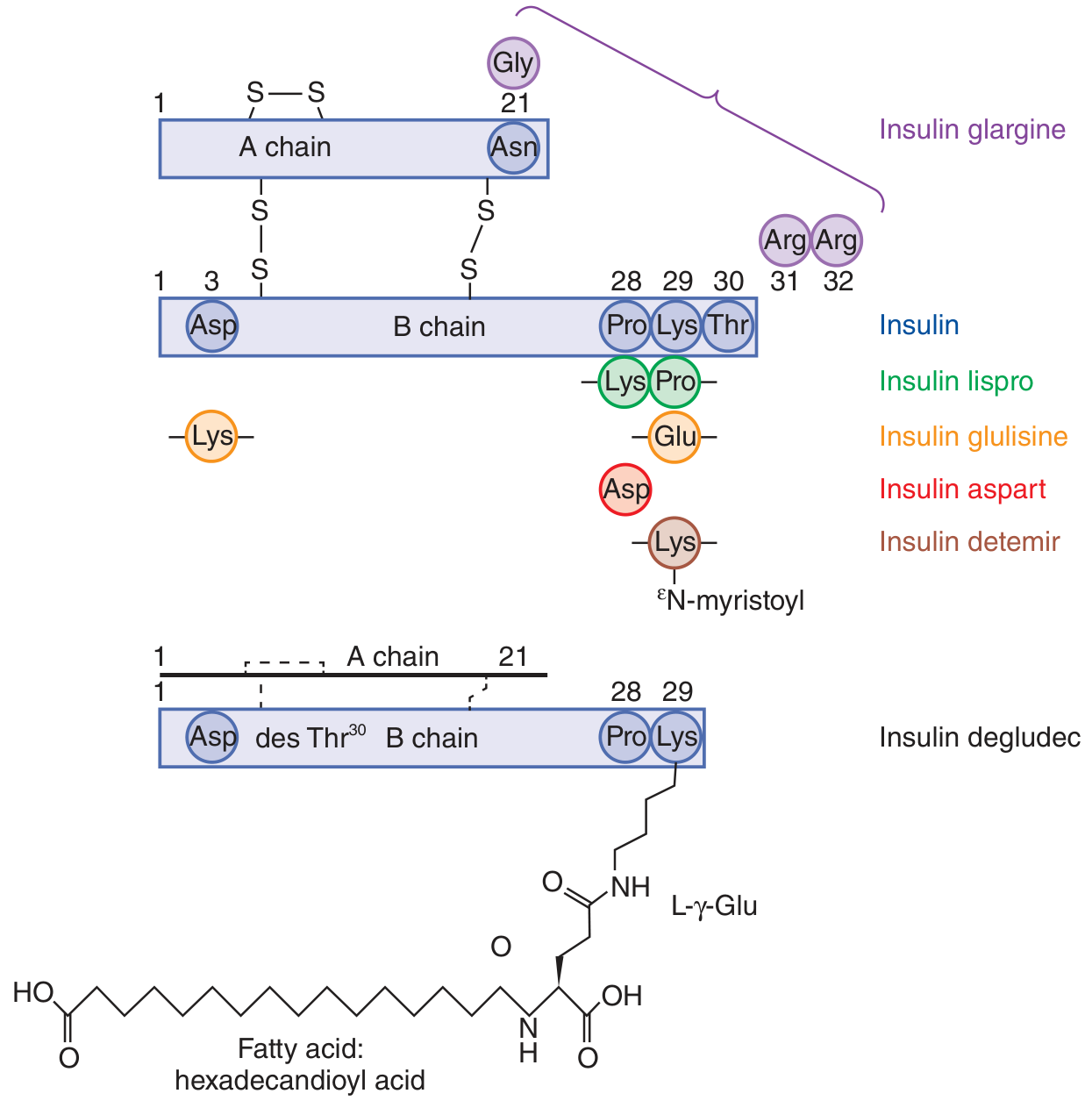
Fig: Structural modifications of insulin analogues - Goodman & Gilman's Pharmacological Basis of Therapeutics
Complete Insulin Pharmacokinetics Table
| Category | Preparation | Onset | Peak | Duration | Key Notes |
|---|---|---|---|---|---|
| Rapid-acting (prandial) | Lispro (U-100, U-200) | 15-30 min | 30-90 min | 3-4 h | Reverse B28 Pro↔Lys; inject ≤15 min before meal |
| Aspart | 15-30 min | 30-90 min | 3-4 h | Pro→Asp at B28 | |
| Glulisine | 15-30 min | 30-90 min | 3-4 h | Lys→Glu at B29; Asn→Lys at B3 | |
| Short-acting | Regular (human, U-100) | ~30 min | 2-4 h | 5-8 h | Inject 30-45 min before meal; can be given IV |
| Regular (U-500) | ~30 min | 2-4 h | 5-8 h | Severe insulin resistance only; SC only | |
| Intermediate-acting | NPH (Isophane) | 2-4 h | 6-10 h | 16-20 h | Cloudy; zinc + protamine suspension |
| Long-acting (basal) | Glargine (U-100) | 1.5-2 h | Peakless | 16-24 h | Clear, pH 4.0; precipitates at neutral SC pH |
| Glargine (U-300, Toujeo) | 1.5-2 h | Peakless | >24 h | More concentrated; once daily | |
| Detemir | 1.5-2 h | Peakless | 16-20 h | Albumin-bound via myristoyl chain; often twice daily | |
| Ultra-long-acting | Degludec (U-100, U-200) | 1 h | Peakless | ~42 h | Multihexamer formation SC; less nocturnal hypoglycemia vs glargine |
| Premixed | NPH/Regular (70/30) | Dual | Dual | Dual | Convenience; less flexibility |
| Premixed analogues | Dual | Dual | Dual | e.g., BiAsp 70/30 | |
| Inhaled | Technosphere insulin (Afrezza) | Very rapid | ~12-15 min | 1.5-3 h | Faster than injected rapid-acting; combined with long-acting required |
Mechanism Modifications - How Analogues Work
To make insulin FASTER:
- Reduce self-association (prevent hexamer formation)
- Lispro: swap B28-Pro and B29-Lys → rapid monomer dissociation
- Aspart: replace B28-Pro with aspartic acid → rapid dissociation
- Glulisine: B29-Lys→Glu, B3-Asn→Lys → rapid dissociation
To make insulin SLOWER/LONGER:
- Glargine: add 2 Arg to C-terminus of B chain + replace A21-Asn with Gly → precipitates at SC pH 7.4 → slow absorption; peakless; cannot mix with acidic solutions
- Detemir: add myristoyl fatty acid to Lys-B29 → albumin binding → slows vascular transport
- Degludec: delete Thr-B30 + hexadecanedioyl acid via γ-Glu spacer at Lys-B29 → multi-hexamer depot SC → albumin binding → duration >42 h
Concentrated Insulins
| Concentration | Preparation | Use |
|---|---|---|
| U-200 | Degludec, Lispro | High-dose patients (reduces injection volume) |
| U-300 | Glargine (Toujeo) | High-dose patients; longer duration |
| U-500 | Regular insulin | Severe insulin resistance (>200 units/day) |
Insulin Delivery Methods
- Subcutaneous injection - syringes, pen devices
- Smart pens - record dose and timing, connect to CGM
- Continuous Subcutaneous Insulin Infusion (CSII / Insulin Pump) - uses rapid-acting analogues only; programmable basal rates + prandial boluses
- Closed-loop (Artificial Pancreas) - CSII + CGM + algorithm; automates delivery; reduces hypoglycemia
- IV infusion - regular insulin only; for DKA, perioperative, ICU (target 140-180 mg/dL in critically ill)
- Inhaled - Afrezza; used pre-prandially with long-acting insulin
- Goldman-Cecil Medicine; Goodman & Gilman's Pharmacological Basis of Therapeutics; Harrison's 22E
6. New and Emerging Insulins
A. Once-Weekly Basal Insulin - Insulin Icodec
The most significant recent advance in insulin therapy.
- Class: Ultra-long-acting basal insulin analogue
- Dosing: Once weekly subcutaneous injection
- Mechanism: Modified to bind reversibly to albumin with very high affinity → extremely prolonged half-life (~196 hours = ~8 days)
- Clinical evidence: 14 clinical trials reviewed; majority showed non-inferiority and in some cases superiority vs daily basal insulins for HbA1c reduction; mild hypoglycemia slightly more frequent vs comparator in select studies
- Use: T1DM and T2DM (FDA approval sought)
- Advantage: Fewer injections → improved adherence, improved compliance, potentially improved glycemic control
[2025 review by Pham et al. in Reviews in Endocrine & Metabolic Disorders, PMID: 40156735]
B. Insulin Efsitora (BIF - Basal Insulin Fc)
- Second once-weekly insulin in late-stage clinical trials (2025)
- Fc fusion protein approach for prolongation
- Results of registration studies becoming available
[2025 review by DeVries & Heise in Diabetes Technology & Therapeutics, PMID: 39911031]
C. Faster-Acting Insulin Aspart (Fiasp)
- Formulated with niacinamide and L-arginine
- Even faster absorption than standard aspart
- Allows injection at meal start or up to 20 min after
D. Biosimilar Insulins
- Glargine biosimilars (e.g., Basaglar, Semglee, Rezvoglar) - lower cost alternatives
- Lispro biosimilar available
- Important for cost-accessibility
E. Smart Closed-Loop (Artificial Pancreas) Systems
- Combine CGM + insulin pump + automated dosing algorithm
- Modern systems: Suspend delivery predicted hypoglycemia; increase delivery for predicted hyperglycemia
- User input still required for meal boluses in current-generation devices
F. Oral Insulin (in development)
- Bioavailability challenges remain; several formulations in clinical trials
- Hepato-preferential delivery would mimic physiologic portal insulin delivery - a key limitation of SC injection
- Harrison's 22E; Goodman & Gilman's; PMID 40156735; PMID 39911031
Quick Summary Table
| Topic | Key Points |
|---|---|
| T2DM pathophysiology | Insulin resistance + progressive beta-cell failure; 8 defects ("ominous octet") |
| T2DM first-line Rx | Metformin + lifestyle (MNT + exercise) |
| DKA triad | Hyperglycemia + ketosis + acidosis (pH <7.3) |
| DKA treatment order | Fluids → Insulin (IV regular) → K+ replacement |
| DKA insulin | 0.1 units/kg/h IV regular; add D5W when glucose <200; switch to SC only when pH >7.3 + anion gap closed |
| Rapid-acting insulins | Lispro, Aspart, Glulisine → inject 15 min before meal |
| Long-acting insulins | Glargine, Detemir, Degludec → peakless, basal coverage |
| Ultra-long | Degludec (~42 h), Icodec (~1 week) |
| Non-pharmacological | MNT + 150 min/week aerobic exercise + weight loss + smoking cessation + psychosocial support + SMBG/CGM |
| Newest insulin | Icodec (once-weekly) - approved/in approval process 2024-2026 |
This is a shared conversation. Sign in to Orris to start your own chat.