Radionuclides in Orthopaedics
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
That was angiography content - I've already collected enough for a comprehensive answer. Let me now compile the full, structured response on Radionuclides in Orthopaedics.
Radionuclides in Orthopaedics
Radionuclide (nuclear medicine) studies in orthopaedics exploit radioactive isotopes to image metabolic and physiologic processes in bone and soft tissue. They complement conventional radiography, CT, and MRI by detecting disease at a functional level - often before anatomic changes are visible.
1. Basic Principles
Nuclear scintigraphy involves the intravenous injection of a radiopharmaceutical - a combination of a radionuclide and a pharmaceutical carrier molecule. The carrier localises to target tissue; the radionuclide emits gamma photons, which are detected by a gamma scintillation camera (sodium iodide crystal + photomultiplier tubes), producing a map of physiologic activity.
-
Radionuclides are radioactive isotopes that undergo spontaneous decay emitting gamma rays (from the nucleus) or X-rays (from electron orbital transitions).
-
Images reflect metabolic function, not anatomy; spatial resolution is lower than CT/MRI.
-
SPECT (Single Photon Emission Computed Tomography): the gamma camera rotates around the patient to generate 3D tomographic images, improving contrast resolution by eliminating overlapping activity.
-
PET (Positron Emission Tomography): detects annihilation photon pairs, giving better spatial resolution than SPECT. Hybrid systems (SPECT/CT, PET/CT, PET/MRI) correlate functional with anatomic data.
-
Rockwood and Green's Fractures in Adults, 10th Ed., p. 253
2. Radionuclides Used in Orthopaedics
| Radionuclide | Agent | Physical t½ | Key Property |
|---|---|---|---|
| Technetium-99m (⁹⁹mTc) | Diphosphonate (MDP/HDP) | 6 hours | 140 keV gamma, ideal for gamma cameras; widely available from ⁹⁹Mo/⁹⁹mTc generator |
| Gallium-67 (⁶⁷Ga) | Gallium citrate | 78 hours | Binds transferrin/lactoferrin; localises inflammation/tumour; imaging at 24-48 hrs |
| Indium-111 (¹¹¹In) | Oxine-WBC complex | 67 hours | Labels autologous leukocytes; specific for infection/abscess |
| ¹⁸F-FDG (PET tracer) | Fluorodeoxyglucose | 110 min | Glucose analogue; taken up by metabolically active cells (infection, tumour) |
| ¹⁸F-NaF (PET tracer) | Sodium fluoride | 110 min | Bone-specific PET agent; marks sites of increased bone metabolism |
| Iodine-125 (¹²⁵I) | Single energy beam | 60 days | Used in single-photon absorptiometry for bone density |
- Miller's Review of Orthopaedics, 9th Ed., p. Nuclear Medicine table
- Rockwood and Green's Fractures in Adults, 10th Ed., p. 253
- Campbell's Operative Orthopaedics, 15th Ed. 2026
3. Skeletal Scintigraphy (Bone Scan)
The most commonly performed nuclear medicine study in orthopaedics.
Agent: ⁹⁹mTc-labeled diphosphonate (MDP or HDP)
Mechanism: Chemisorption of phosphonate compound to the mineral (hydroxyapatite) phase of bone, particularly at sites of increased osteoblastic activity. Regional blood flow also governs tracer delivery. Over 50% of administered dose is delivered to bone within 1 hour; the kidneys excrete the remainder.
Three-Phase Bone Scan
| Phase | Timing | What it Shows |
|---|---|---|
| Phase 1 - Radionuclide Angiogram (Flow) | 0-2 min (dynamic, during injection) | Arterial blood flow to the region |
| Phase 2 - Blood Pool (Tissue Phase) | 2-6 min after injection | Vascular distribution, soft tissue hyperemia |
| Phase 3 - Delayed (Static) | 3-4 hours post-injection | Osteoblastic activity; bone metabolism |
- Adding the three phases increases specificity from 74% to 94% for osteomyelitis.
- A four-phase study is sometimes used (24-hour delayed images) for complex infection scenarios.
Scan Appearances
- "Hot" lesion (increased uptake): increased osteoblastic + osteoclastic activity + regional hyperemia - seen in infection, fracture, tumour, degenerative joint disease.
- "Cold" lesion (decreased uptake): permeative/small round cell tumours, avascular necrosis (early), sequestrum, regions shielded by periosteal pus/vasospasm.
Overall Performance
- Highly sensitive, poor specificity - a normal scan largely rules out skeletal pathology; a positive scan requires further workup.
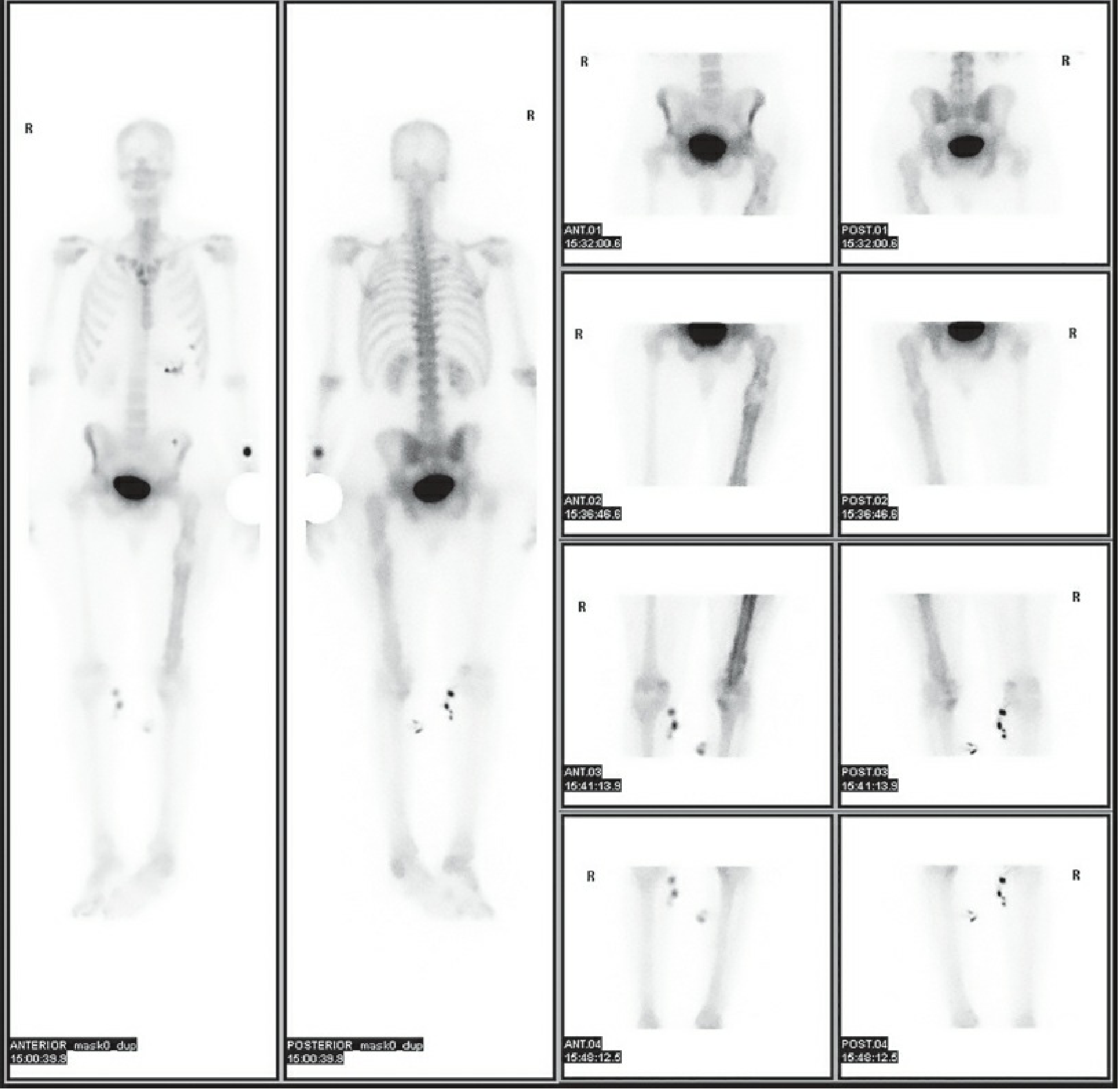
Whole-body ⁹⁹mTc bone scintigraphy showing anterior and posterior whole-body views alongside regional spot images - Rockwood & Green's Fractures in Adults, 10th Ed.
4. Gallium-67 Imaging
Mechanism: After IV injection, ⁶⁷Ga rapidly binds to serum transferrin and circulates. It localises to sites of infection/inflammation because:
- Increased regional blood flow and vascular permeability allow greater accumulation.
- Neutrophils release lactoferrin during inflammation; gallium has a higher binding affinity for lactoferrin than transferrin.
- Imaging performed at 24-48 hours (or longer); relatively poor imaging agent because photon energies are not optimal for modern gamma cameras.
- Less dependent on vascular flow than technetium - can identify foci missed by bone scan.
- Cannot differentiate cellulitis from osteomyelitis.
- Difficulty distinguishing pyogenic from granulomatous infections.
Use in orthopaedics:
- Best used in combination with ⁹⁹mTc bone scan for detection of osteomyelitis (especially spondylodiscitis): sensitivity 90%, specificity 100%, accuracy 94% with combined scanning.
- Useful for documenting resolution of infection (changes rapidly as active infection resolves).
- Localises in neoplasia - useful adjunct in tumour workup.
5. White Blood Cell (Leucocyte) Scintigraphy
Gold standard nuclear medicine technique for orthopaedic-related infections.
Labeling Methods
¹¹¹In-Oxine WBC:
- 50 mL blood drawn; leukocytes separated; incubated with ¹¹¹In-oxine (lipid-soluble, crosses cell membrane) for 30 min; reinjected.
- Imaging at 24 hours to allow leukocyte localisation and blood pool clearance.
- Preferred for chronic osteomyelitis and axial skeleton infections.
⁹⁹mTc-HMPAO WBC:
- 50-75 mL blood; labelled in plasma (no cell separation needed); faster preparation.
- Imaging at 4 hours for peripheral skeleton.
- Sensitivity 97.7%, specificity 96.8% for acute osteomyelitis.
- Preferred in children (smaller spleen radiation dose, less blood needed).
- Superior to bone scan in children under 6 months (poor bone scan sensitivity at that age).
Interpretation - Marrow Subtraction Protocol
WBC scans must be interpreted alongside ⁹⁹mTc-sulfur colloid marrow imaging:
- Sulfur colloid particles (0.1-2 µm) are taken up by reticuloendothelial cells in marrow, mapping normal marrow.
- In osteomyelitis: photopenic defect on sulfur colloid (marrow replaced) + increased activity on WBC scan = discordance = positive for infection.
- Congruent activity on both = normal marrow = no infection.
Limitations
- Labour-intensive; costly; requires processing of potentially infectious blood products.
- Diagnostic accuracy reduced in the axial skeleton.
- False-positives with periarticular nonunions/posttraumatic arthropathy.
6. In Vivo Labeling - Antigranulocyte Scintigraphy
- Uses monoclonal antibodies/fragments against granulocytes - no blood processing required.
- Distinguishes true infection (high granulocyte concentration) from areas of high metabolic activity without inflammation.
- Meta-analysis: sensitivity 81%, specificity 77% for osteomyelitis.
7. PET / FDG-PET
¹⁸F-FDG PET - highest diagnostic accuracy for infection and malignancy.
Mechanism: FDG enters the glucose metabolic cycle and accumulates in cells with high glucose utilisation - monocytes, lymphocytes, activated leukocytes, macrophages, giant cells. Patient fasts 4-6 hours and rests 1 hour before scan to minimise normal tissue uptake.
Clinical role in orthopaedics:
- Chronic osteomyelitis (especially axial skeleton): highest diagnostic accuracy of any nuclear technique.
- Bone and soft tissue tumours: delineates lesions and inflammatory activity at very early stages.
- PET/CT and PET/MRI provide simultaneous functional + anatomic correlation.
¹⁸F-NaF PET - bone-specific positron tracer; more sensitive and higher resolution than ⁹⁹mTc bone scan for skeletal metastases and metabolic bone disease.
Limitations: reduced availability, high cost; false-positives from postoperative granulation tissue, implants, recent fractures, atherosclerosis, and neuro-osteoarthropathy.
8. Marrow Imaging
Agent: ⁹⁹mTc-sulfur colloid
- Taken up by reticuloendothelial cells in liver (85%), spleen (10%), marrow (5%).
- Half-life in blood: 2-3 minutes; imaging after 20-minute delay.
- Primary role: combined with ¹¹¹In WBC scan for osteomyelitis diagnosis (marrow subtraction technique, above).
9. Bone Density Measurement (Photon Absorptiometry)
| Method | Radionuclide | Principle | Limitation |
|---|---|---|---|
| Single-photon absorptiometry (SPA) | ¹²⁵I (single energy) | Cortical bone density inversely proportional to photon transmission | Unreliable in axial skeleton; soft tissue depth alters beam |
| Dual-photon absorptiometry (DPA) | Gadolinium-153 (two energies) | Accounts for soft tissue attenuation | Allows femoral neck and axial skeleton measurement |
| DEXA (dual-energy X-ray absorptiometry) | X-ray (not isotope-based) | Replaced isotope-based methods clinically | - |
10. Clinical Applications in Orthopaedics
Fractures
- Bone scans positive in 80% of fractures at 24 hours, 95% at 72 hours.
- Detects stress fractures and insufficiency fractures not visible on plain X-ray.
- Classic "Honda sign" (H-pattern uptake) in sacral insufficiency fractures.
- Useful in non-accidental trauma (child abuse): skeletal survey + bone scan together detect more injuries than either alone.
- Hyperemia (phases 1+2) normalises 4-8 weeks post-injury, helping age fractures.
Osteomyelitis / Infection
- Three-phase bone scan: good screening tool; if all three phases negative, infection essentially excluded.
- Combined ⁹⁹mTc + ⁶⁷Ga: sensitivity 90%, specificity 100%, accuracy 94% for spinal infection.
- WBC scintigraphy: gold standard for peripheral bone infection.
- FDG-PET: best for chronic/axial osteomyelitis.
- SPECT-CT with delayed bone scan increases sensitivity by localising areas of increased metabolism.
Avascular Necrosis (AVN)
- Early AVN: decreased uptake ("cold") due to vascular compromise.
- Reparative phase: increased uptake as revascularisation and new bone formation occur.
- Bone scan predates MRI as an early-detection tool, though MRI is now preferred.
Prosthetic Joint / Periprosthetic Infection
- Three-phase bone scan: increased specificity (74% → 94%) with three-phase technique.
- Normal bone scan essentially excludes loosening/infection.
- ¹⁸F-FDG PET/CT and ¹⁸F-NaF PET/CT used for periprosthetic joint infection (PJI) diagnosis.
- Gallium scan combined with bone scan: distinguishes aseptic loosening from infection.
- ¹¹¹In WBC scan: differentiates true infection from hematoma/seroma when MRI is equivocal.
Tumours / Neoplasia
- Whole-body bone scan: detection of skeletal metastases and primary bone tumours.
- "Cold" lesions in permeative tumours (small round cell tumours) that elicit little bone reaction.
- ⁶⁷Ga scan: localises inflammation and tumour; used in bone tumour workup.
- FDG-PET: best for staging and monitoring treatment response in bone malignancies.
- ¹⁸F-NaF PET: superior to ⁹⁹mTc bone scan for osteoblastic metastases.
Spinal Infection (Spondylodiscitis)
- ⁹⁹mTc bone scan: increased activity, diffuse on blood pool, focally increased on delayed views - persists for months.
- ⁶⁷Ga scan: particularly useful for soft tissue component of spondylodiscitis; changes rapidly with resolution.
- ¹¹¹In WBC scan: useful for abscess detection but less reliable in acute infections; false-negatives in chronic infection.
Reflex Sympathetic Dystrophy (CRPS)
- Three-phase ⁹⁹mTc bone scan: periarticular uptake pattern is characteristic; helpful in diagnosis.
11. Artifacts from Orthopaedic Hardware
Indwelling metallic implants can shield the gamma camera from photons, projecting as photopenic defects on nuclear images. Multiple projections and knowledge of implant position are essential to avoid misinterpretation.
12. Summary Comparison
| Modality | Agent | Best Orthopaedic Use | Sensitivity | Specificity |
|---|---|---|---|---|
| ⁹⁹mTc Bone Scan (3-phase) | MDP | Fractures, AVN, osteomyelitis screening | High | Low-moderate |
| ⁶⁷Ga Scan | Gallium citrate | Spondylodiscitis (soft tissue), tumour | Moderate | Moderate |
| ¹¹¹In WBC Scan | Oxine-WBC | Chronic osteomyelitis, prosthetic infection | Moderate-high | High |
| ⁹⁹mTc HMPAO WBC | HMPAO-WBC | Acute osteomyelitis (esp. paediatric) | ~98% | ~97% |
| FDG-PET | ¹⁸F-FDG | Chronic/axial osteomyelitis, tumour staging | Highest | Highest |
| ¹⁸F-NaF PET | Sodium fluoride | Skeletal metastases, bone metabolism | Very high | High |
Sources:
- Rockwood and Green's Fractures in Adults, 10th Ed. 2025 - Nuclear Imaging, Bone Scintigraphy, Leucocyte Scintigraphy, PET sections (pp. 253-255, 963-964)
- Campbell's Operative Orthopaedics, 15th Ed. 2026 - Radionuclide Scanning, Nuclear Imaging for PJI
- Miller's Review of Orthopaedics, 9th Ed. - Nuclear Medicine table
This is a shared conversation. Sign in to Orris to start your own chat.