Explain me 10 common heart disease with ECG changes and ecg images of those disease
Reading File
Finding Sources
Finding Sources
Searching the Web
ECG changes 10 common heart diseases images STEMI atrial fibrillation heart block
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive textbook content and ECG images for all 10 conditions. Let me compile the full answer.
10 Common Heart Diseases and Their ECG Changes
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery causes transmural ischemia. Three ionic events drive the ECG changes: rapid repolarization, decreased resting membrane potential from K+ loss, and delayed depolarization in infarcted cells - all producing current flow toward the injured zone.
ECG Changes:
- Hyperacute T waves (very early - minutes)
- ST segment elevation ≥1 mm in ≥2 contiguous leads (hallmark finding)
- Reciprocal ST depression in opposite leads
- Pathological Q waves (>25% of R wave amplitude, >40 ms wide) - appear after hours/days as necrosis silences tissue
- T-wave inversion follows as ischemia evolves
- Localisation: Inferior (II, III, aVF) = RCA; Anterior (V1-V4) = LAD; Lateral (I, aVL, V5-V6) = LCx
(From Ganong's Review of Medical Physiology; Harrison's Principles of Internal Medicine 22E)
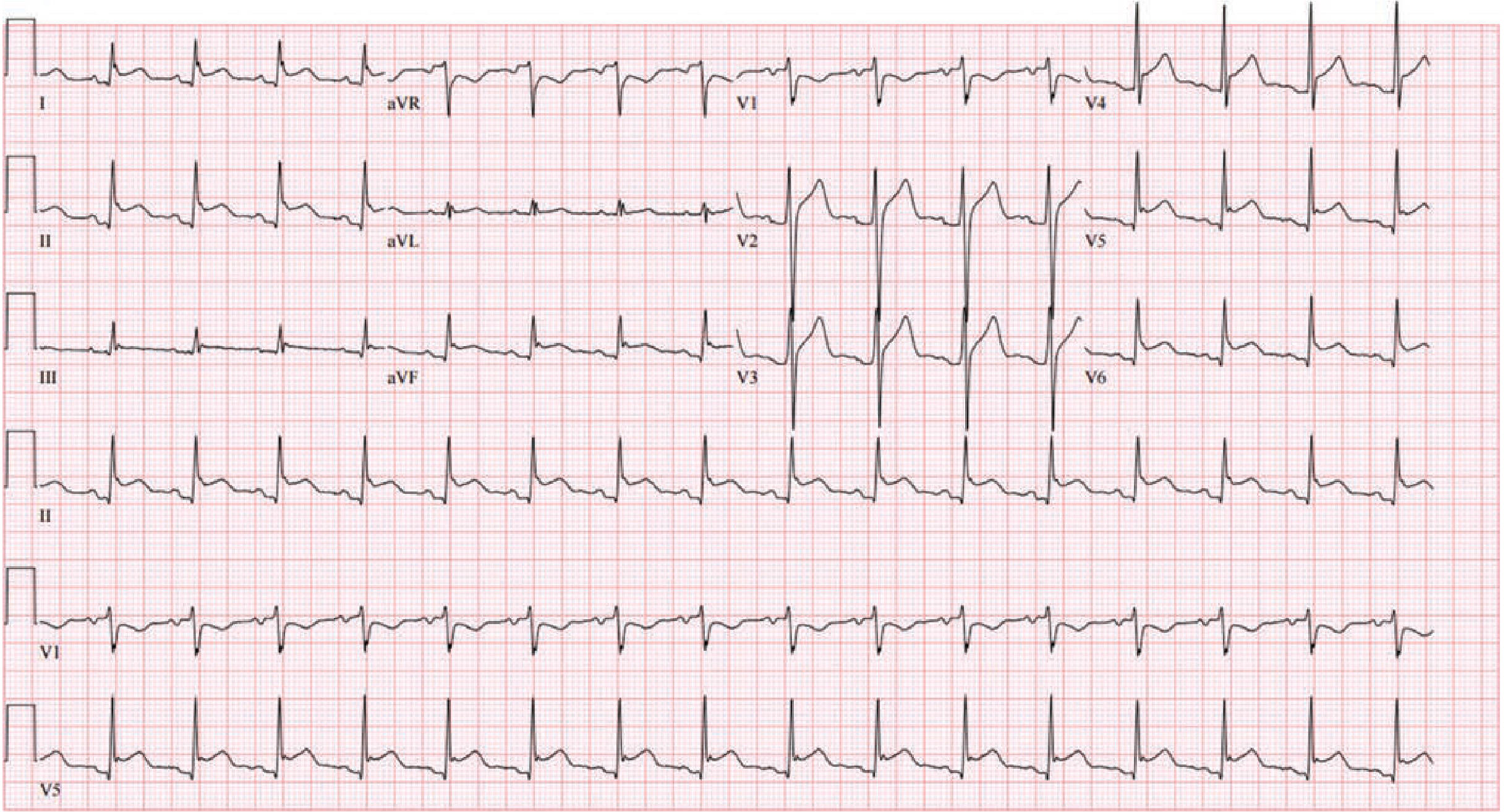
ECG Image - STEMI (inferior-lateral MI from LCx occlusion):
ST-segment elevation in leads II, III (inferior) and aVF, with ST depression as reciprocal changes in anterior leads. This patient had 100% occlusion of the left circumflex artery. - Tintinalli's Emergency Medicine
ST vector diagram explaining subendocardial vs transmural ischemia:

A: Subendocardial ischemia - ST vector toward ventricular cavity, giving ST depression in overlying leads. B: Transmural/epicardial ischemia - ST vector directed outward, giving ST elevation. - Harrison's Principles of Internal Medicine 22E
2. NSTEMI / Unstable Angina (Non-ST-Elevation ACS)
Pathophysiology: Partial coronary occlusion or severe stenosis causes subendocardial ischemia without full-thickness myocardial necrosis.
ECG Changes:
- ST depression (horizontal or downsloping) in affected leads
- T-wave inversion (may be deep and widespread)
- Wellens' T-wave sign: Deep symmetric T-wave inversions in V1-V4 - pathognomonic of critical LAD stenosis; associated with high-grade left anterior descending coronary artery obstruction
- ECG may be normal in up to 6% of cases
- No Q waves or ST elevation (by definition)
- Diagnosis relies on elevated troponin + ECG pattern + symptoms
ECG Image - Anterior wall ischemia with Wellens' T-wave pattern:

Deep, symmetric T-wave inversions in V1-V4 (and leads I, aVL) - "Wellens' T-wave sign." This pattern is strongly associated with high-grade LAD stenosis and may precede anterior STEMI. - Harrison's Principles of Internal Medicine 22E
3. Atrial Fibrillation (AF)
Pathophysiology: Chaotic, high-frequency electrical activity in the atria (often from pulmonary vein foci or dilated atria) prevents coordinated atrial contraction. The AV node is bombarded with irregular impulses, producing an irregularly irregular ventricular response.
ECG Changes:
- Absent P waves - replaced by fine, irregular fibrillatory (f) waves at 350-600/min (best seen in V1 and lead II)
- Irregularly irregular RR intervals (the defining feature)
- Normal QRS morphology unless aberrant conduction or bundle branch block present
- Ventricular rate typically 100-160/min if uncontrolled
- Fine baseline undulation between QRS complexes
(From Guyton and Hall Textbook of Medical Physiology)
ECG Image - Atrial Fibrillation:

Lead II tracing showing atrial fibrillation: absent organized P waves, fine fibrillatory baseline, and irregular QRS intervals. Only ventricular QRS and T waves are identifiable. - Guyton and Hall Textbook of Medical Physiology
4. AV Heart Block (1st, 2nd, and 3rd Degree)
Pathophysiology: Impaired conduction through the AV node or His-Purkinje system. Causes include fibrosis, ischemia, medications (beta-blockers, digoxin), and infiltrative diseases.
ECG Changes:
| Type | Key ECG Finding |
|---|---|
| 1st degree | PR interval >200 ms; all P waves conduct; no dropped beats |
| 2nd degree Mobitz I (Wenckebach) | Progressive PR prolongation until a P wave is blocked (dropped QRS); "group beating"; RR shortens before dropped beat |
| 2nd degree Mobitz II | Fixed PR interval with sudden non-conducted P waves; QRS may be wide (bundle branch block present) |
| 3rd degree (complete) | Complete AV dissociation - P waves and QRS are completely independent; escape rhythm (junctional 40-60 bpm, or ventricular 20-40 bpm) |
(From The Washington Manual of Medical Therapeutics; Harrison's Principles of Internal Medicine 22E)
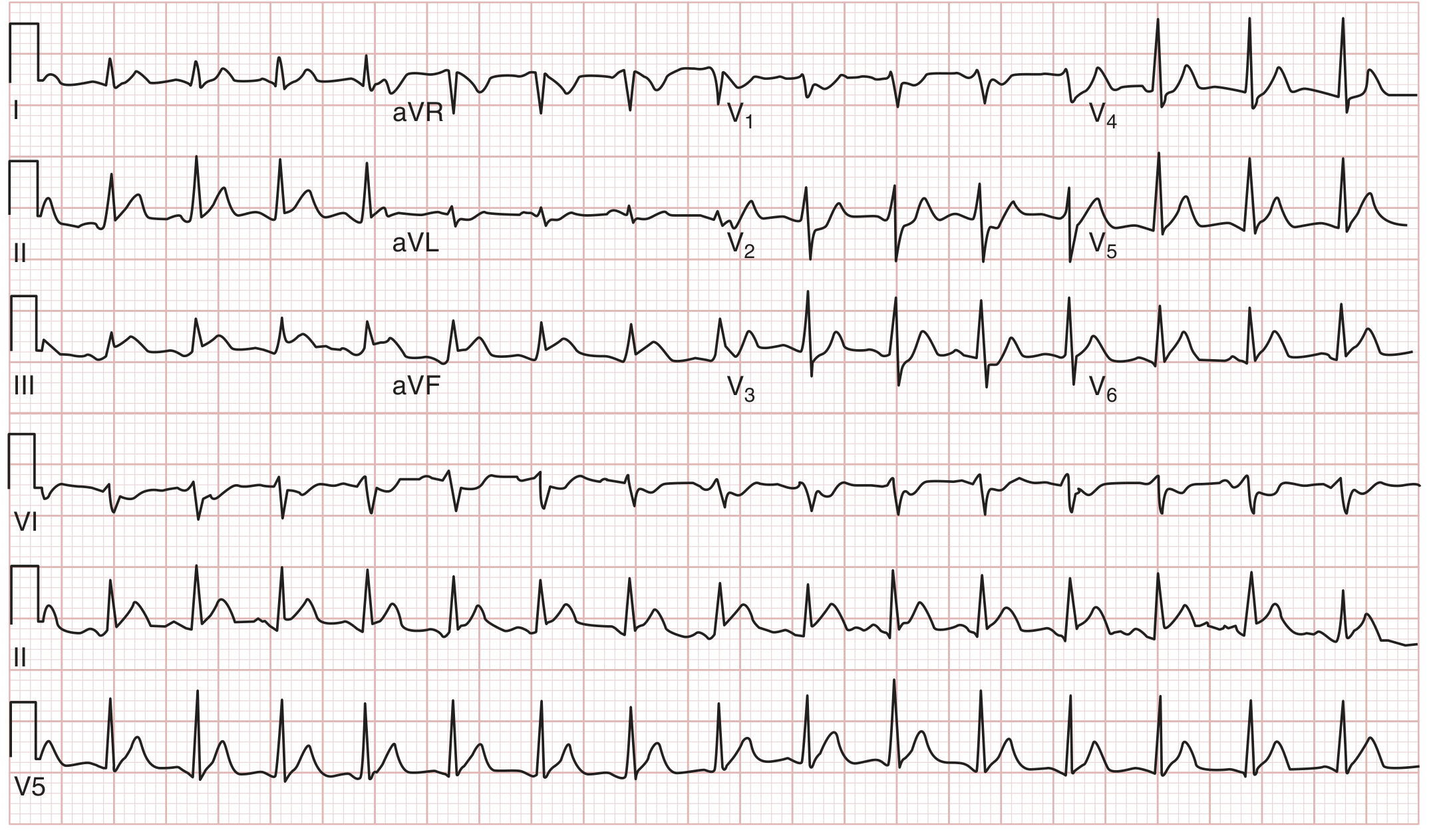
ECG Image - All degrees of AV block:

A: First-degree AV block - PR >200 ms, no dropped beats. B: Mobitz I (Wenckebach) - group beating with progressive PR prolongation before dropped beat. C: 2:1 AV block in lead V5. D: High-degree AV block - consecutive P waves not conducted. E: Complete (third-degree) AV block in lead V1 - complete AV dissociation. - The Washington Manual of Medical Therapeutics
5. Left Bundle Branch Block (LBBB) and Right Bundle Branch Block (RBBB)
Pathophysiology: Conduction block in the respective bundle branch forces the ventricle to depolarize via slower cell-to-cell spread, widening the QRS.
ECG Changes:
RBBB:
- QRS duration ≥120 ms
- RSR' ("M-shape" or "rabbit ears") in V1
- Wide, slurred S wave in leads I, V5-V6
- ST and T waves discordant with terminal QRS in right precordial leads
LBBB:
- QRS duration ≥120 ms
- Broad, notched (W-shaped) QRS in leads I, aVL, V5-V6
- Small r waves and broad deep S waves in right precordial leads (V1-V3)
- No septal q waves in leads I, V5-V6
- Axis usually normal or left deviated
- New LBBB in chest pain = treat as STEMI equivalent
(From Goldman-Cecil Medicine)
ECG Image - RBBB (B) and LBBB (E):
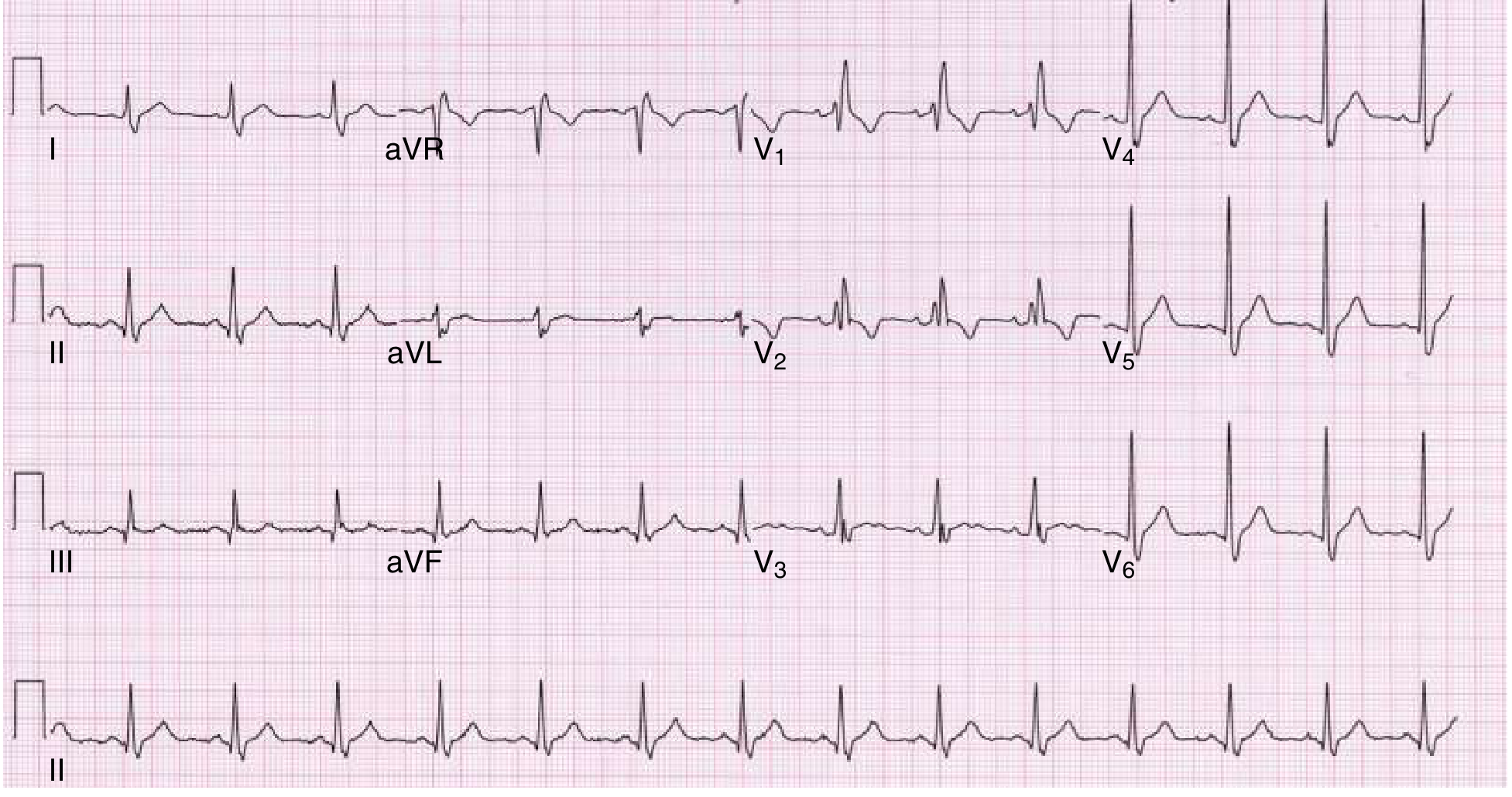
RBBB: Widened QRS, rsR' pattern in V1, wide terminal S wave in V5-V6, discordant ST/T waves in right precordial leads. - Goldman-Cecil Medicine
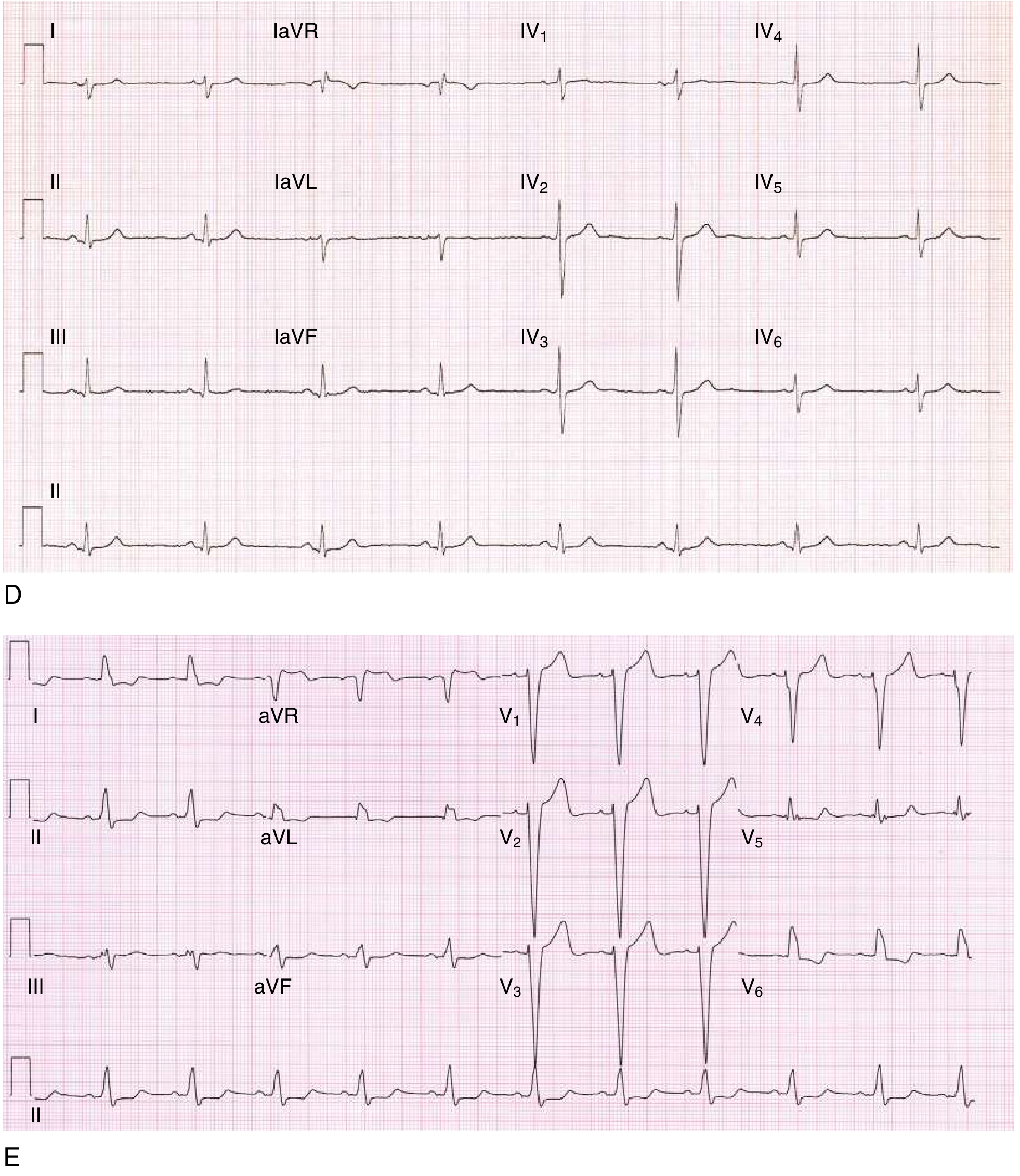
Top (D): Left posterior fascicular block with right axis deviation. Bottom (E): LBBB - widened QRS with broad notched complexes in I, aVL; deep S waves and ST-T discordance throughout precordium. - Goldman-Cecil Medicine
6. Wolff-Parkinson-White Syndrome (WPW)
Pathophysiology: An accessory pathway (Bundle of Kent) bypasses the AV node, pre-exciting the ventricles before the normal impulse arrives via the His-Purkinje system. This creates ventricular fusion complexes in sinus rhythm and can mediate reentrant tachycardias.
ECG Changes (in sinus rhythm):
- Short PR interval (<120 ms) - bypasses AV nodal delay
- Delta wave - slurred initial upstroke of the QRS (slow cell-to-cell conduction from accessory pathway insertion)
- Wide QRS (>120 ms) - due to ventricular pre-excitation + fusion
- Pseudo-ST and T-wave changes - discordant T waves secondary to abnormal depolarization
- During tachycardia: Narrow-complex (orthodromic AVRT, most common) or wide-complex irregular (AF with pre-excitation - dangerous, can degenerate to VF)
(From Tintinalli's Emergency Medicine; Pfenninger and Fowler's Procedures for Primary Care)
ECG Image - WPW Syndrome:
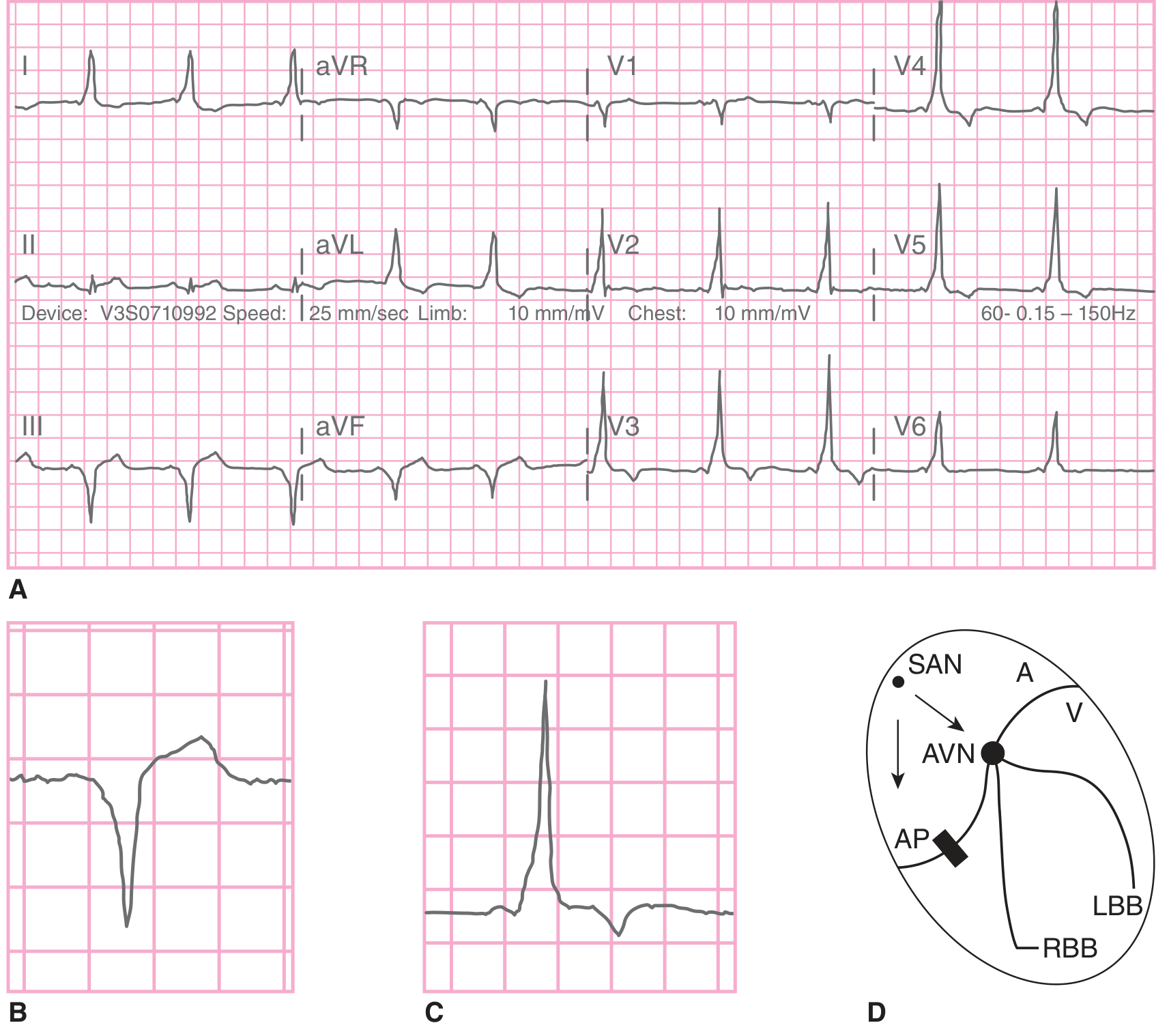
A: 12-lead ECG in WPW sinus rhythm. B: Single complex showing widened, slurred QRS with delta wave. C: Normal QRS for comparison. D: Cardiac impulse travels both via accessory pathway (AP) and AV node simultaneously, creating fusion complexes. - Tintinalli's Emergency Medicine
7. Acute Pericarditis
Pathophysiology: Inflammation of the pericardium causes diffuse epicardial injury current. The atria are also involved (explaining PR changes). Unlike STEMI, the injury is diffuse (not territorial).
ECG Changes (4 stages):
- Stage 1 (hours-days): Diffuse concave ("saddle-shaped") ST elevation in almost all leads (I, II, III, aVF, V2-V6) + PR depression (most sensitive marker); aVR shows reciprocal ST depression + PR elevation
- Stage 2: ST and PR return toward baseline
- Stage 3: T-wave inversions (after ST normalizes)
- Stage 4: ECG returns to normal
Key distinction from STEMI: Pericarditis - diffuse, concave ST elevation, PR depression, no reciprocal ST depression (except aVR), no Q waves. STEMI - convex/localized ST elevation, reciprocal ST depression, Q wave formation.
(From Fuster and Hurst's The Heart 15th Ed; Braunwald's Heart Disease)
ECG Image - Acute Pericarditis:
Stage I acute pericarditis: Diffuse ST-segment elevation (concave upward) with concordant PR-segment depression in multiple non-territory-specific leads. aVR shows simultaneous ST depression and PR elevation - the reciprocal hallmark. - Fuster and Hurst's The Heart 15th Ed
8. Hypertrophic Cardiomyopathy (HCM)
Pathophysiology: Asymmetric septal or concentric left ventricular hypertrophy increases myocardial mass, increases voltage, and alters depolarization/repolarization patterns. The markedly abnormal ECG often raises the clinical suspicion in young patients.
ECG Changes:
- Left ventricular hypertrophy (LVH) criteria: Sokolow-Lyon (S in V1 + R in V5/V6 ≥35 mm), Cornell voltage, or Romhilt-Estes criteria
- Deep, narrow Q waves in lateral (I, aVL, V5-V6) and inferior leads - from abnormal septal depolarization (characteristic "pseudo-infarct" pattern)
- T-wave inversions - especially in lateral leads; giant T-wave inversions in apical HCM (Yamaguchi syndrome: ≥10 mm in V4-V5)
- Left atrial enlargement (P mitrale)
- Poor R-wave progression, nonspecific ST-T changes
- Atrial fibrillation in ~20% of cases
(From Tintinalli's Emergency Medicine; Goldman-Cecil Medicine)
9. Ventricular Tachycardia (VT)
Pathophysiology: Rapid, sustained ventricular ectopic activity arising below the Bundle of His. Most commonly occurs in structural heart disease (post-MI scar, cardiomyopathy). Wide QRS because conduction uses slow myocyte-to-myocyte spread rather than the fast His-Purkinje system.
ECG Changes:
- Wide QRS complex (≥120 ms), rate 100-250 bpm
- Regular rhythm in monomorphic VT
- AV dissociation - P waves march through independently at slower rate (pathognomonic when present)
- Fusion beats - QRS morphology intermediate between sinus and VT (diagnostic)
- Capture beats - normal narrow QRS interrupting VT (diagnostic)
- Left axis deviation in most VT
- Concordance - all precordial leads either all positive or all negative (positive concordance suggests WPW; negative concordance = strong VT indicator)
- Polymorphic VT / Torsades de Pointes: QRS complexes twist around the isoelectric line; associated with long QT interval
Differentiating VT from SVT with aberrancy (Brugada criteria):
- Absence of RS complex in all precordial leads → VT
- RS interval >100 ms → VT
- AV dissociation → VT
- Morphology criteria (LBBB-like or RBBB-like pattern inconsistent with true bundle branch block) → VT
(From Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22E)
10. Atrial Flutter
Pathophysiology: A macro-reentrant circuit in the right atrium (usually involving the cavotricuspid isthmus in typical flutter) produces regular atrial activity at 250-350 beats/min. The AV node typically conducts at 2:1, giving a ventricular rate of ~150 bpm.
ECG Changes:
- "Sawtooth" flutter (F) waves at 250-350/min - most prominent in leads II, III, aVF, and V1
- Regular or regularly irregular ventricular rhythm (depends on AV conduction ratio: 2:1, 3:1, 4:1, or variable)
- Ventricular rate ~150 bpm in 2:1 block (classic presentation)
- Flutter waves may be hidden within QRS or T waves - look in inferior leads or use carotid sinus massage/adenosine to slow AV conduction and reveal flutter waves
- Normal QRS morphology (unless aberrant conduction)
- Negative F waves in inferior leads = typical (counterclockwise) flutter; positive F waves = atypical (clockwise/reverse typical) flutter
Clinical note: A ventricular rate of exactly 150 bpm should always prompt search for concealed flutter waves beneath the T waves.
(From Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22E)
Quick Reference Summary Table
| # | Condition | Key ECG Finding | Rate/Rhythm |
|---|---|---|---|
| 1 | STEMI | ST elevation ≥1mm, Q waves, reciprocal ST depression | Normal or sinus tachycardia |
| 2 | NSTEMI/UA | ST depression, T-wave inversions (Wellens' sign) | Usually normal sinus |
| 3 | Atrial Fibrillation | No P waves, fine f waves, irregularly irregular RR | 100-160 bpm uncontrolled |
| 4 | Heart Block | Progressive PR prolongation → dropped beats → AV dissociation | Bradycardia |
| 5 | Bundle Branch Block | Wide QRS ≥120 ms; RSR' in V1 (RBBB), notched R in I/aVL (LBBB) | Normal unless tachycardia |
| 6 | WPW | Short PR, delta wave, wide QRS | Can trigger SVT/AF |
| 7 | Acute Pericarditis | Diffuse saddle ST elevation, PR depression; no reciprocal changes | Usually sinus tachycardia |
| 8 | HCM | LVH criteria, deep septal Q waves, giant T inversions (apical HCM) | Variable |
| 9 | Ventricular Tachycardia | Wide QRS, AV dissociation, fusion beats, axis deviation | 100-250 bpm |
| 10 | Atrial Flutter | Sawtooth F waves 250-350/min, regular or regularly irregular QRS | ~150 bpm (2:1 block) |
Sources:
- Ganong's Review of Medical Physiology, 26th Ed (conduction system, MI ECG changes)
- Harrison's Principles of Internal Medicine 22E (ischemia ECG, ST elevation causes)
- Goldman-Cecil Medicine (bundle branch block, VT, AV block)
- Guyton and Hall Textbook of Medical Physiology (atrial fibrillation)
- Tintinalli's Emergency Medicine (STEMI, WPW, cardiomyopathies)
- Fuster and Hurst's The Heart, 15th Ed (acute pericarditis)
- The Washington Manual of Medical Therapeutics (AV conduction disturbances)
- Braunwald's Heart Disease (pericarditis, accessory pathways)
Rheumatic heart disease full note
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
rheumatic heart disease pathophysiology Jones criteria management 2024 guidelines
Reading File
Reading File
Reading File
Reading File
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.