Hi
Hey! How can I help you today?
Shoulder joint
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive content. Here is a full anatomical overview of the shoulder joint:
Shoulder Joint - Anatomy & Structure
Overview
The shoulder joint is the most mobile joint in the human body, permitted by a "large ball-small socket" bony arrangement. It is technically composed of four articulations that work together:
- Glenohumeral joint - the true ball-and-socket joint (main articulation)
- Sternoclavicular joint - the only true bony connection between the upper limb and axial skeleton
- Acromioclavicular (AC) joint - a plane/gliding joint with a fibrocartilaginous disc
- Scapulothoracic joint - a functional articulation (no true synovial joint)
- Campbell's Operative Orthopaedics, 15th Ed. 2026
Bony Anatomy
The glenohumeral joint has been compared to a "golf ball on a tee" - the large humeral head articulates against (not truly within) the small, shallow glenoid cavity of the scapula. Key measurements:
| Feature | Value |
|---|---|
| Humeral head articular arc | ~160 degrees |
| Radius of curvature (humeral head) | ~25 mm |
| Glenoid depth (superoinferior) | ~9 mm (with labrum) |
| Glenoid depth (anteroposterior) | ~5 mm (with labrum) |
| Neck-shaft angle (humeral) | 45° ± 5° |
| Glenoid height | 30-48 mm |
The glenoid surface radius of curvature is 2-3 mm larger than that of the humeral head, creating a slightly conforming but not constrained joint.
- Campbell's Operative Orthopaedics, 15th Ed.
Glenoid Labrum
The fibrocartilaginous glenoid labrum rings the glenoid cavity and is critical for joint stability:
- Deepens the glenoid socket by 50%
- Increases glenoid surface area to 75% of humeral head vertically and 57% horizontally
- Acts as a "bumper" against humeral head translation
- Important anatomic variants include the sublabral foramen (anterosuperior) and the Buford complex (absent anterosuperior labrum + cord-like middle glenohumeral ligament, present in ~1.5% of shoulders)
Joint Capsule & Ligaments
The capsule is loose and voluminous, allowing wide range of motion, and does not restrict movement until the extremes. It is thin posteriorly and reinforced anteriorly by the glenohumeral ligaments.
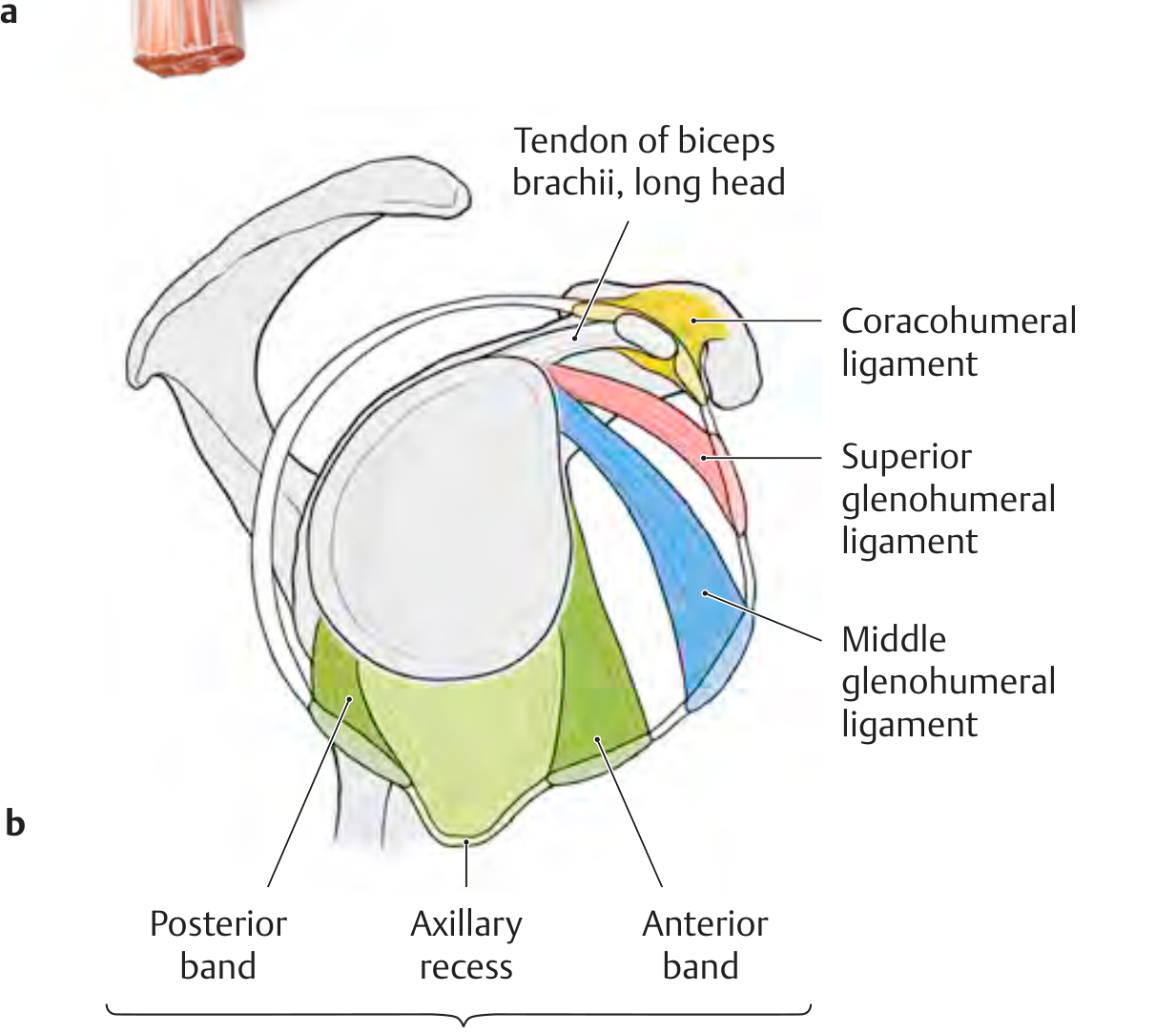
Glenohumeral Ligaments - Function Summary
| Ligament | Function |
|---|---|
| Coracohumeral ligament (CHL) | Restrains inferior translation and external rotation of adducted arm; stabilizes biceps tendon in bicipital groove |
| Superior GHL (SGHL) | Primary restraint to inferior subluxation at 0° abduction; also restrains anterior/posterior stress at 0° |
| Middle GHL (MGHL) | Restrains anterior translation at 45° abduction; absent in up to 30% of shoulders |
| Inferior GHL - anterior band | Main restraint to anterior and inferior translation with arm at 90° abduction + external rotation ("position of apprehension") |
| Inferior GHL - posterior band | Restrains posterior/inferior translation with arm at 90° abduction + internal rotation |
The inferior glenohumeral ligament complex (IGHLC) forms a "hammock-type sling" - with external rotation, the anterior band tightens and the posterior band fans out, and vice versa.
- Miller's Review of Orthopaedics, 9th Edition; THIEME Atlas of Anatomy
Muscles
Extrinsic Muscles (control scapular movement)
- Rhomboids
- Levator scapulae
- Trapezius
- Serratus anterior
Intrinsic Muscles (control glenohumeral joint)
- Rotator cuff (SITS): Supraspinatus, Infraspinatus, Teres minor, Subscapularis
- Deltoid
- Pectoralis major
- Teres major
- Latissimus dorsi
- Biceps brachii
Rotator Cuff Role
The rotator cuff does two things simultaneously:
- Compresses the humeral head into the glenoid (centering effect)
- Fixes the fulcrum against which the deltoid can contract to elevate the arm
The key force couple is subscapularis (anterior) vs. infraspinatus + teres minor (posterior), which keeps the humeral head centered even with superior cuff tears.
Stability - Static vs Dynamic
| Stabilizer Type | Structures |
|---|---|
| Static | Bony anatomy, glenoid labrum, glenohumeral ligaments, capsule, negative intra-articular pressure |
| Dynamic | Rotator cuff muscles, biceps tendon, scapulothoracic mechanics |
The bony architecture provides minimal intrinsic stability - most stability comes from the surrounding soft tissues. This is why the shoulder is the most commonly dislocated large joint in the body.
Sternoclavicular Joint (for context)
-
Double gliding joint with an articular disc
-
The only true joint connecting the upper extremity to the axial skeleton
-
Rotates 30° during shoulder motion
-
Posterior sternoclavicular ligament is the strongest structure and primary restraint to anteroposterior instability
-
Miller's Review of Orthopaedics, 9th Ed.
Would you like to go deeper into any specific aspect - such as the rotator cuff in detail, bursae, blood supply/nerve supply, or clinical relevance (e.g., dislocations, impingement)?
This is a shared conversation. Sign in to Orris to start your own chat.