Capnography
Reading File
Finding Sources
Finding Sources
Searching PubMed
capnography clinical monitoring
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
I now have rich, comprehensive material from multiple authoritative sources. Let me compile the full answer.
Capnography
Capnography is the continuous, non-invasive measurement and graphical display of CO2 concentration in exhaled gases throughout the respiratory cycle. It provides real-time breath-by-breath information about ventilation, perfusion, and metabolism.
Physiology
CO2 is produced by cellular metabolism, transported to the lungs via the blood, and expelled during exhalation. Because CO2 diffuses rapidly into the alveolar space, the concentration at the end of expiration - the end-tidal CO2 (ETCO2 or PetCO2) - closely approximates alveolar CO2, which itself approximates arterial PaCO2 (PaCO2) in patients with healthy lungs.
- In normal lungs: PaCO2 - ETCO2 gradient = 2-5 mmHg (arterial slightly higher)
- The gradient widens with increased dead space, ventilation-perfusion mismatch, low cardiac output, or pulmonary overdistension
- In disease states such as COPD, pulmonary embolism, or single-lung ventilation, ETCO2 significantly underestimates PaCO2, and an arterial blood gas is required for accurate CO2 assessment
The alveolar dead space fraction (AVDSf) can be estimated from capnography:
AVDSf = (PaCO2 - PetCO2) / PaCO2
This is a useful indicator of alveolar dead space and has been associated with mortality in pediatric patients with acute hypoxemic respiratory failure.
- Miller's Anesthesia, 10e, p. 11316-11317
The Capnogram Waveform
Time-based capnography is the most common form. It displays a characteristic square-wave pattern with five labeled phases:
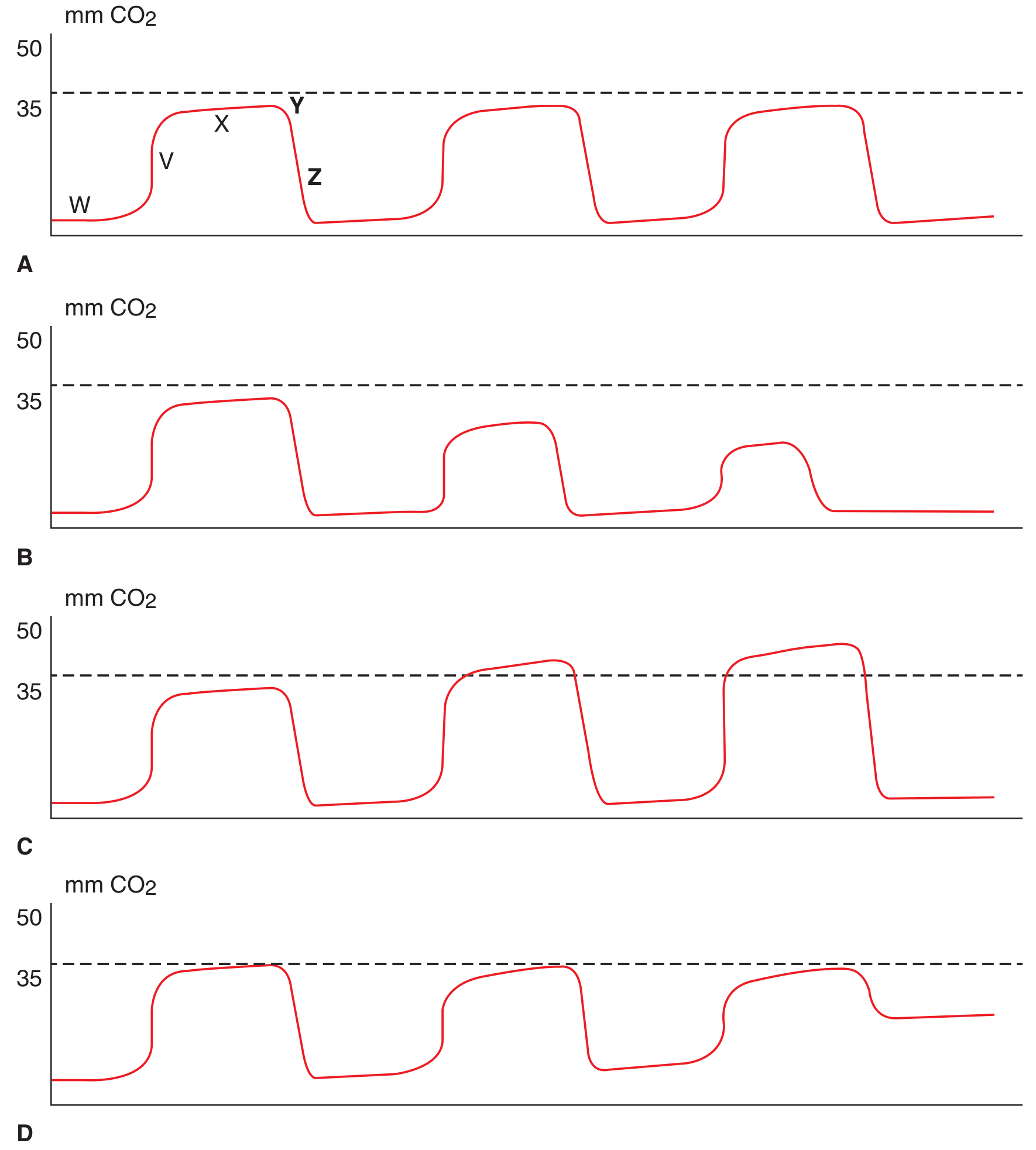
| Phase | Label | Description |
|---|---|---|
| W | Inspiratory baseline | CO2 near zero; fresh gas inhalation |
| V | Expiratory upstroke | Anatomic dead space gas exits first |
| X | Expiratory plateau | Alveolar gas; CO2 rises to plateau |
| Y | End-tidal point | Peak CO2 = ETCO2 value |
| Z | Inspiratory downstroke | Rapid fall as fresh gas enters |
Abnormal Waveform Patterns
| Pattern | Appearance | Clinical Cause |
|---|---|---|
| Apnea | Serially decreasing or absent waveforms | Respiratory arrest, apneic events |
| Hypoventilation | Upward trending plateau and ETCO2 | Opioid-induced respiratory depression, over-sedation |
| Rebreathing / Air trapping | Elevated baseline (CO2 > 0 during inspiration) | Exhausted CO2 absorber, COPD air trapping |
| Obstructive disease | Rising "shark-fin" upslope in expiratory phase | Bronchospasm, asthma, COPD |
- Tintinalli's Emergency Medicine, p. 122
Types of Capnography Systems
By Sampling Method
Mainstream (non-aspirating)
- CO2 sensor is placed directly in-line with the breathing circuit
- No gas is diverted - measures in real-time at the airway
- Larger and heavier; requires intubated patient
- More accurate; no sampling delay
Sidestream (aspirating)
- Aspirates 50-200 mL/min of gas from the circuit to a remote sensor
- Smaller, can be used in non-intubated patients (nasal cannula, face mask)
- Most commonly used in the operating room
- Potential for sampling errors: dilution by fresh gas, aspiration of water vapor, time delay
- In neonates, the sampling rate can approach or exceed minute ventilation, causing falsely low ETCO2 readings
By Display Type
Time-based capnography - CO2 vs. time; most common, more accurate at slower respiratory rates
Volumetric capnography - CO2 vs. exhaled volume; available on some ventilators; directly calculates dead space and helps set optimal PEEP; demonstrates response to bronchodilator therapy
- Barash Clinical Anesthesia, 9e, p. 2113; Miller's Anesthesia, 10e, p. 11316-11317
Clinical Applications
1. Confirming Endotracheal Tube Placement
The most reliable and immediate method. Multiple studies show 100% accuracy of waveform capnography for detecting correct ETT placement. Continuous waveform capnography is accurate even during cardiac arrest. An absent waveform after intubation indicates esophageal intubation.
- Roberts & Hedges' Clinical Procedures in Emergency, p. 435
2. Procedural Sedation and Analgesia (PSA)
Capnography is the single most important monitor for patients undergoing sedation:
- Detects hypoventilation and apnea before pulse oximetry - particularly when the patient is receiving supplemental oxygen, which can maintain SpO2 despite significant hypoventilation
- A meta-analysis (Waugh et al.) found cases of respiratory depression were 17.6 times more likely to be detected with capnography than without
- All episodes of apnea >20 seconds in MAC (monitored anesthesia care) cases were detected by capnography but not by the anesthesia provider
- In upper endoscopy patients, pulse oximetry detected only ~50% of apnea/disordered breathing episodes that capnography detected; hypoxemia (SpO2 <90%) developed an average of 45.6 seconds after the onset of airway-disordered breathing
- Particularly important in infants and toddlers, who have smaller functional residual capacity and higher oxygen consumption
ACEP gives capnography use during ED procedural sedation a Level B recommendation. The ASA recommends routine capnography for all patients undergoing moderate sedation.
- Barash Clinical Anesthesia, 9e, p. 2492-2493; Roberts & Hedges', p. 712
3. Cardiac Arrest and Resuscitation
ETCO2 is a powerful real-time marker of cardiac output during CPR:
| ETCO2 Value | Interpretation |
|---|---|
| Falls abruptly | Onset of cardiac arrest |
| Increases during CPR | Effective compressions delivering CO2 to lungs |
| Returns to physiologic levels | Return of spontaneous circulation (ROSC) |
| >20 mmHg at 20 min | Predicts higher chance of ROSC |
| <10 mmHg at 20 min | Predicts almost no chance of ROSC |
| Sudden rise | Early sign of ROSC |
| >12-15 mmHg | Indicates high-quality compressions |
The 2015 resuscitation guidelines recommend continuous waveform capnography for all intubated patients during resuscitation. ETCO2 <10 mmHg after 20 minutes should not be used alone to cease resuscitation efforts.
- Tintinalli's EM, p. 4115-4117; Roberts & Hedges', p. 415
4. Monitoring Ventilation in ICU / OR
- Continuous surrogate for PaCO2 in patients with healthy lungs
- Monitors respiratory rate directly from the airway (more reliable than impedance-based monitoring, which cannot distinguish chest wall movement from actual ventilation - important in obstructive apnea or laryngospasm)
- Volumetric capnography used to titrate PEEP and assess bronchodilator response
- In transcutaneous CO2 monitoring (TCOM) - used during high-frequency ventilation where capnography is less reliable
5. Detection of Air Embolism and Pulmonary Embolism
A sudden drop in ETCO2 without apnea signals a decrease in pulmonary blood flow (dead space increase), as occurs in PE or venous air embolism.
Important Limitations
| Limitation | Explanation |
|---|---|
| ETCO2 < PaCO2 | The gradient widens with dead space, low CO, V/Q mismatch |
| Inaccurate in COPD | Incomplete expiration causes air trapping; ETCO2 unreliable |
| Sidestream in neonates | Sampling rate can dilute or exceed minute ventilation, giving falsely low readings |
| Cuffless ETT | Gas leak causes ETCO2 to underestimate actual CO2 |
| Not a substitute for ABG | In PE, severe COPD, single-lung ventilation - ABG is necessary |
Recent Evidence
A 2024 systematic review and meta-analysis (Khanna et al., J Clin Anesth, PMID 38184918) confirmed that continuous capnography monitoring on hospital wards reduces postoperative respiratory failure and opioid-induced respiratory depression - supporting its use beyond the operating room and ICU.
Key takeaway: Capnography provides immediate, continuous, non-invasive insight into ventilation, airway patency, cardiac output, and pulmonary perfusion. Its greatest clinical value is detecting respiratory compromise before hypoxemia develops - making it indispensable during procedural sedation, intubation, and cardiac arrest resuscitation.
This is a shared conversation. Sign in to Orris to start your own chat.