Central venous pressure and it's importance
Reading File
Finding Sources
Searching PubMed
"central venous pressure"[MeSH Terms] AND "hemodynamic monitoring"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive material from multiple authoritative textbooks plus the CVP waveform image. Let me compile a thorough response.
Central Venous Pressure (CVP)
Definition
Central venous pressure is the blood pressure measured in the great veins (superior or inferior vena cava) close to the right atrium. Because there are no valves between the vena cava and the right atrium, CVP is a good approximation of right atrial pressure and, by extension, an estimate of right ventricular end-diastolic pressure (preload).
- Fishman's Pulmonary Diseases and Disorders, p. 2593
Normal Values
| Setting | CVP Range |
|---|---|
| Normal healthy adult | 2-8 mmHg (approximately 3-10 cmH2O) |
| Target in sepsis (Surviving Sepsis Campaign) | 8-12 mmHg |
| Adequate volume resuscitation | Return to +5 cmH2O |
CVP is measured in mmHg with electronic transducers or cmH2O with water manometers. These are not interchangeable (1 mmHg ≈ 1.36 cmH2O).
CVP Waveform
The CVP waveform reflects cardiac events and is best interpreted alongside a simultaneous ECG:
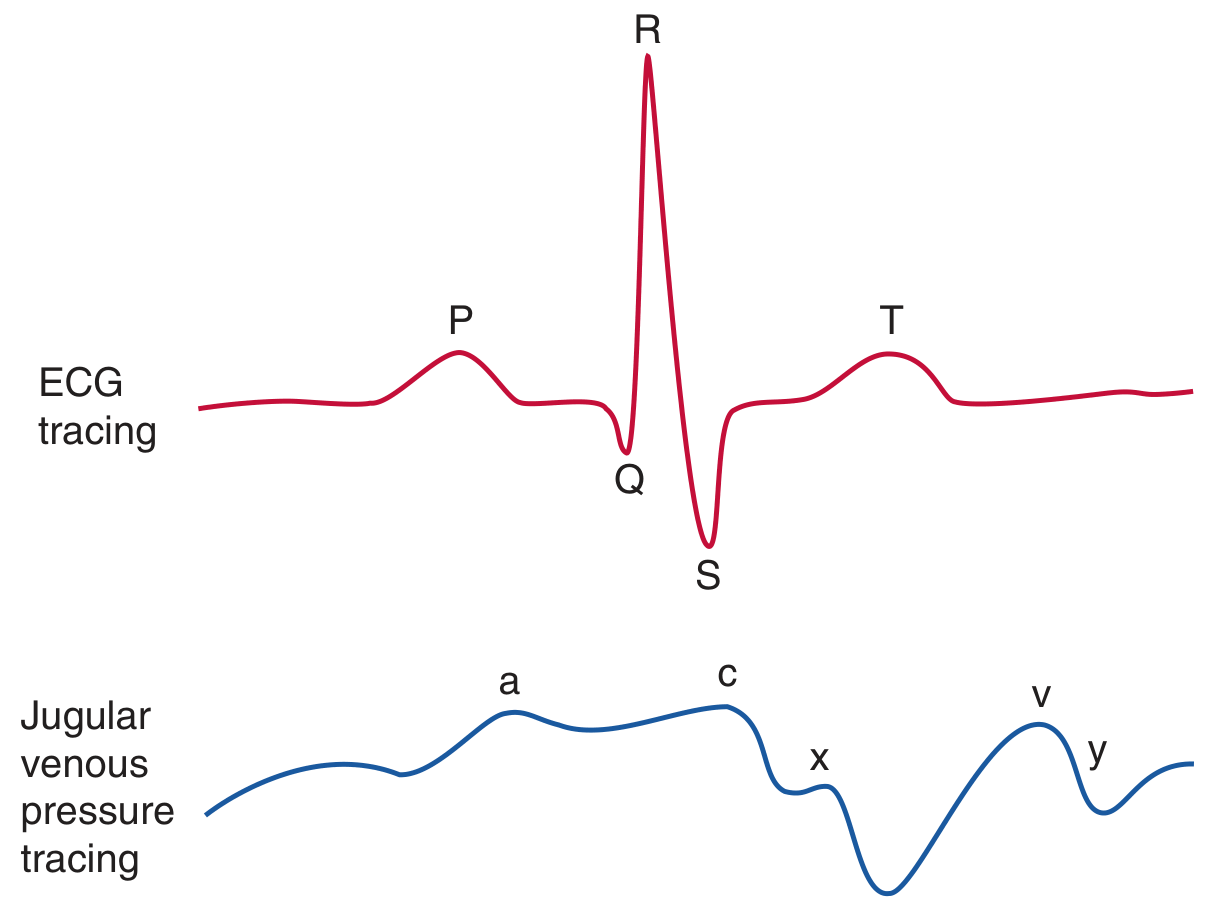
Figure: CVP waveform (blue) correlated with ECG (red) - Fishman's Pulmonary Diseases and Disorders
| Component | Mechanism | ECG Timing |
|---|---|---|
| a wave | Right atrial contraction | After P wave |
| c wave | Tricuspid valve bulging into RA during early ventricular systole | End of QRS |
| x descent | Atrial relaxation | Before T wave |
| v wave | Atrial filling while tricuspid valve is closed | End of T wave |
| y descent | Tricuspid valve opens, RA empties into RV | Before next P wave |
CVP is measured at the base of the c wave at end-expiration for accuracy.
Waveform Abnormalities
| Finding | Condition |
|---|---|
| Large v wave | Tricuspid regurgitation / RV failure |
| Attenuated y descent | Cardiac tamponade |
| Prominent y descent | Pericardial constriction or RV overload |
- Fishman's Pulmonary Diseases, p. 2592-2593
Physiological Basis and Determinants
CVP is the back pressure to systemic venous return. It is determined by multiple interacting factors:
Blood Volume & Venous Return
- Total circulating blood volume
- Venous return from periphery
- Cardiac output
Compliance of the Central Compartment
- Vascular tone (vasoconstriction raises CVP; vasodilation lowers it)
- Right ventricular compliance
Cardiac Factors
- Myocardial disease (cardiomyopathy, MI)
- Pericardial disease (tamponade, constrictive pericarditis)
- Tricuspid valve disease (stenosis, regurgitation)
- Dysrhythmias (junctional rhythm, atrial fibrillation)
The venous system holds roughly two-thirds of total circulating blood volume and acts as a capacitance reservoir. CVP reflects how well this system is filling the right heart.
- Tintinalli's Emergency Medicine, p. 32-2
- Mulholland & Greenfield's Surgery, p. 564
Clinical Importance and Uses
1. Volume Status Assessment
CVP is one of the most reliable guides to adequacy of fluid replacement when cardiac function is normal. Return of CVP to normal (+5 cmH2O) in the presence of normal cardiac function generally indicates adequate transfusion/resuscitation.
Peripheral vasoconstriction can maintain arterial blood pressure even when the volume deficit is not fully corrected - CVP will more accurately reveal this under-filled state and prevent premature anaesthesia (which abolishes vasoconstriction and can precipitate cardiovascular collapse).
- Pye's Surgical Handicraft, p. 39
2. Differentiating Shock Types
| Shock Type | CVP |
|---|---|
| Hypovolemic | Low |
| Distributive (septic, anaphylactic) | Low |
| Obstructive (PE, tamponade) | High |
| Cardiogenic | High |
A CVP < 5 mmHg in a young trauma patient with ongoing hemorrhage = hypovolemic shock warranting volume resuscitation. However, these are generalizations - always interpret in clinical context.
- Mulholland & Greenfield's Surgery, p. 564
3. Dynamic Fluid Challenge (the correct way to use CVP)
CVP should not be used as a single static number. The proper approach is a fluid challenge:
- Administer a fluid bolus of 250-500 mL rapidly over 5-10 minutes
- Observe the CVP response:
| CVP Response | Interpretation |
|---|---|
| Rise of 2-5 cmH2O, drifts back in 10-20 min | Normal - adequate cardiac response |
| No change in CVP | Patient is "empty" - needs more fluid |
| Large, sustained rise in CVP | High preload with cardiac insufficiency or volume overload |
- Bailey & Love's Surgery, p. 40
4. Procedural Indications (Central Venous Catheter)
CVP monitoring is one of the primary indications for central venous cannulation, alongside:
-
Vasoactive drug administration
-
Hyperalimentation / TPN
-
Transvenous cardiac pacing
-
Temporary hemodialysis
-
Pulmonary artery catheterization
-
Aspiration of venous air emboli
-
Chemotherapy / agents irritating to peripheral veins
-
Rapid fluid infusion via large cannulas
-
Miller's Anesthesia, p. 4792
Measurement Technique
-
A central venous catheter (CVC) tip should be positioned at the cavoatrial junction - approximately 2 cm caudal to the carina on chest X-ray
-
Connect one CVC lumen to a pressure transducer
-
The transducer must be leveled to the phlebostatic axis (4th intercostal space, mid-axillary line) and zeroed to atmospheric pressure
-
Read at end-expiration to eliminate respiratory variation
-
Mulholland & Greenfield's Surgery, p. 564
Limitations of CVP - Critical Perspective
This is an area where modern evidence has substantially revised older thinking:
-
Poor marker of preload: CVP is a poor reflection of left or right ventricular end-diastolic volume. Ventricular compliance can change minute to minute in shock.
-
Poor predictor of fluid responsiveness: Numerous studies show CVP cannot reliably predict whether a patient will respond to fluids. Consensus guidelines now recommend against using static CVP to guide fluid responsiveness assessment - dynamic variables (pulse pressure variation, stroke volume variation) are preferred.
-
There is no single "correct" CVP: Some shocked patients need a CVP of 5 cmH2O, others may need 15 cmH2O or higher. The number must be interpreted in clinical context.
-
Influenced by non-volume factors: Positive pressure ventilation, PEEP, pleural pressure, and increased pulmonary vascular resistance all elevate CVP without reflecting true volume overload.
-
CVP most useful at extremes: A very low CVP helps exclude right heart failure; a very high CVP suggests it. Intermediate values are unreliable for decision-making.
-
Surviving Sepsis goal (8-12 mmHg) questioned: Several investigators have found no survival benefit to targeting this CVP goal, and the concept has been challenged in recent sepsis guidelines.
- Fishman's Pulmonary Diseases, p. 2592-2593
- Mulholland & Greenfield's Surgery, p. 564
- Bailey & Love's Surgery, p. 40
CVP vs. Pulmonary Artery Catheter (PAC)
Where CVP reflects right-sided filling pressures, a PAC provides pulmonary artery wedge pressure (PCWP), which approximates left atrial pressure and left ventricular preload. PAC use has declined markedly with the rise of non-invasive alternatives (Doppler ultrasound, pulse contour analysis, indicator dilution). PAC is most useful when myocardial damage coincides with hypovolemia, major surgery, or severe sepsis.
Summary Table
| Feature | Detail |
|---|---|
| Normal range | 2-8 mmHg / 3-10 cmH2O |
| Represents | Right atrial pressure / RV preload |
| Measurement site | Cavoatrial junction |
| Measured at | End-expiration, base of c wave |
| Key waveform components | a, c, x, v, y |
| Main clinical uses | Fluid resuscitation guidance, shock differentiation, monitoring |
| Key limitation | Poor predictor of fluid responsiveness |
| Modern recommendation | Use dynamic over static CVP assessment |
CVP remains a useful bedside tool when interpreted dynamically and in the full clinical context - its greatest value is at its extremes and as part of a fluid challenge, not as a standalone static number.
This is a shared conversation. Sign in to Orris to start your own chat.