Please teach me tuning fork test to learn memorise and understand fully everything on it (Ent)
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything I need from multiple authoritative ENT textbooks. Let me compile a comprehensive, well-structured teaching resource.
Tuning Fork Tests in ENT - Complete Guide

1. Foundations - Why Tuning Forks?
A tuning fork examination is part of every routine neurotologic exam. It can be done at the bedside or in the office, requires no equipment, and gives immediate information about the type of hearing loss (conductive vs. sensorineural). Tuning forks are especially important:
- When formal audiometry is unavailable
- To confirm audiometric findings before surgery (especially stapedectomy)
- When there is a masking dilemma on audiometry
- When cochlear viability is uncertain
"The importance of both the Weber and Rinne tests cannot be overemphasized as they may confirm or refute audiometric test results." - Shambaugh Surgery of the Ear
2. Which Frequency Fork to Use?
| Frequency | Use | Notes |
|---|---|---|
| 512 Hz | Best overall - preferred | Gold standard; avoids somatosensory vibration artifact |
| 256 Hz | Also acceptable; good sensitivity | May be felt as vibration rather than heard |
| 1024 Hz | Less reliable | Decays too quickly |
| 128 Hz | NOT recommended for hearing tests | Felt as vibration - confuses patient, compromises results |
Key activation rule: Strike the fork gently against your elbow (soft surface) - NOT against a table or hard object. Hard surface striking produces harmonics and overtones that corrupt the pure tone and make the test unreliable. A correctly activated fork at the ear canal generates ~70 dBA.
3. THE RINNE TEST
Purpose
Compares air conduction (AC) vs. bone conduction (BC) in the same ear.
Procedure (Loudness Comparison Method - preferred)
- Activate the 512 Hz fork (strike gently on elbow)
- Place the base firmly on the mastoid behind the pinna (bone conduction)
- Then move the fork to 2 cm in front of the ear canal (air conduction)
- Ask: "Which position sounds louder?"
(Alternative: threshold method - hold fork by ear until no longer heard, then move to mastoid. Less reliable.)
Interpretation
| Result | Meaning | What it tells you |
|---|---|---|
| AC louder than BC = Positive Rinne (+) | Normal | Normal hearing OR sensorineural hearing loss (SNHL) |
| BC louder than AC = Negative Rinne (-) | Abnormal | Conductive hearing loss (CHL) in the tested ear |
| AC = BC (equivocal) | Uninterpretable | Up to 10% of patients with 11-40 dB air-bone gap |
Memory Trick
"Positive = normal. Negative Rinne = bad."
- + Rinne: Air is better → normal pathway → SNHL or normal
- - Rinne: Bone is better → middle ear problem → CHL
How sensitive is the Rinne test?
| Air-bone gap (dB) | Detection rate (256 Hz fork) |
|---|---|
| 10-20 dB | ~50% sensitivity |
| 20-30 dB | ~70% sensitivity |
| >30 dB | ~90% sensitivity |
The test only reliably detects CHL above 20-30 dB air-bone gap. A negative Rinne with a 512 Hz fork implies a conductive loss of 20 dB or worse.
The False Positive Rinne (Critical Trap!)
If testing a profoundly deaf ear, bone conduction from the mastoid crosses the skull and is picked up by the opposite (better) cochlea. This makes BC appear better than AC in the dead ear → false negative Rinne (reads as CHL when cochlea is actually dead/SNHL).
This is also called a "Dead Ear" false negative or pseudo-conductive pattern. This is why the Stenger test (below) and masking are important in unilateral profound loss.
To mask when needed: use a Barany noise box (generates sufficient masking noise by air conduction in the non-test ear). Tragal rubbing or paper rustling produce insufficient noise.
4. THE WEBER TEST
Purpose
A test of lateralization - determines which ear a centrally-placed vibration is heard in.
Procedure
- Activate the 512 Hz fork
- Place the stem firmly on the midline of the skull - any of these points:
- Forehead (most common)
- Nasofrontal suture
- Bridge of nose
- Incisor teeth / mandibular symphysis
- Vertex of skull
- Ask: "Do you hear this in the left ear, right ear, or equally in the middle?"
Interpretation
| Patient hears sound... | Interpretation |
|---|---|
| Midline / equally both ears | Normal hearing, OR equal hearing loss bilaterally |
| In the poorer/bad ear | That ear has conductive hearing loss |
| In the better/good ear | The opposite (poorer) ear has sensorineural hearing loss |
Why does CHL lateralize to the bad ear? (The physiology explained)
When the middle ear is blocked (fluid, ossicular problem), external noise cannot reach the cochlea. This removes the masking effect of environmental sound in that ear. The bone-conducted tone becomes relatively louder in the conductive-loss ear because there is less competing background noise. Think of it like covering one ear in a noisy room - that covered ear actually hears internal sounds more clearly.
Memory Trick
"Weber Worst" for CHL - sound goes TO the worst (conductive) ear.
"Weber Better" for SNHL - sound goes to the BETTER ear.
Clinical Limitation
Scott-Brown's notes the Weber test has low sensitivity and specificity and is "marginally better than chance" with only ~33% accuracy for reliably distinguishing CHL from SNHL. It is only interpretable when hearing loss is unilateral or asymmetric. It adds little value when you already know from otoscopy that the middle ear is abnormal.
5. THE BING TEST
Purpose
Tests for the occlusion effect - determines if a conductive hearing loss component is present.
Physiological Basis
In normal hearing, closing the ear canal augments bone-conducted sound (the occlusion effect). In CHL, this augmentation is already happening due to the conductive block - so additionally occluding the canal produces no further change.
Procedure
- Activate the fork and place its base on the mastoid process
- While the patient listens, alternately open and close the ear canal with your finger (or have patient do it)
- Ask: "Does the sound get louder when I close the ear?"
Interpretation
| Result | Finding |
|---|---|
| Positive Bing (+) = sound gets louder when canal closed | Normal hearing OR SNHL (occlusion effect present) |
| Negative Bing (-) = sound stays the same when canal closed | Conductive hearing loss (no occlusion effect) |
Memory Trick
"Positive Bing = Ping!" - the sound bounces up, you hear more. Negative Bing = no change = conductive problem.
Clinical Note
The Bing test has lower sensitivity and specificity than the Rinne test and frequently suggests CHL in patients with normal hearing. It is less commonly performed but useful as a confirmatory test.
6. THE SCHWABACH TEST
Purpose
Compares the patient's bone conduction to a normal-hearing examiner's bone conduction. Tests cochlear reserve.
Prerequisite
The examiner must have confirmed normal hearing.
Procedure
- Activate the fork, place on the patient's mastoid
- When the patient no longer hears it, immediately move the fork to the examiner's mastoid
- Note whether the examiner can still hear it
(Repeat the reverse: start on examiner, transfer to patient)
Interpretation
| Result | Meaning |
|---|---|
| Normal Schwabach - both stop hearing at ~same time | Normal hearing |
| Diminished/Shortened Schwabach - patient stops first | Sensorineural hearing loss (impaired cochlea) |
| Prolonged/Extended Schwabach - patient hears longer | Conductive hearing loss (bone conduction enhanced due to blocked middle ear) |
Memory Trick
"SNHL = Short Schwabach" (cochlea damaged, dies sooner).
"CHL = Long Schwabach" (sound trapped in, lasts longer).
7. THE STENGER TEST (Functional/Malingering Loss)
Purpose
Detects functional (non-organic/feigned) hearing loss in a patient claiming unilateral or significantly asymmetric hearing loss.
Principle - Stenger Phenomenon
When two identical tones are presented simultaneously to both ears, a normal person only perceives the louder one (from the ear where it is physically louder). A malingerer cannot acknowledge hearing the tone in their "bad" ear without admitting they can hear it.
Procedure
- Present a tone at a soft level (10 dB above threshold) to the better ear
- Simultaneously present the same tone at a louder level to the "bad" ear
- A truly deaf person (in bad ear) only hears through the good ear and responds
- A malingerer hears the louder tone in the "bad" ear but, to maintain the pretense, suppresses their response
Interpretation
- Negative Stenger (patient responds) = hearing loss is genuine
- Positive Stenger (patient does not respond even though good ear stimulus is audible) = functional/feigned hearing loss
A speech Stenger may be performed using spondee words (at SRT level) in place of pure tones.
8. ABC TEST (Absolute Bone Conduction Test)
Purpose
Compares patient's bone conduction to the examiner's (like Schwabach, but the examiner occludes their own ear to enhance their threshold).
Procedure
- Activated fork placed on patient's mastoid until no longer heard
- Then placed on examiner's mastoid (examiner's ear closed with finger to improve sensitivity)
- Compare duration of hearing
Used mainly to distinguish SNHL from CHL - less commonly performed in modern practice.
9. COMPLETE COMPARISON TABLE
| Test | Fork Placement | What it Tests | Normal | CHL | SNHL |
|---|---|---|---|---|---|
| Rinne | Mastoid vs. ear canal | AC vs. BC in same ear | Positive (AC>BC) | Negative (BC>AC) | Positive (AC>BC) |
| Weber | Midline skull | Lateralization | Midline | Lateralizes to worse ear | Lateralizes to better ear |
| Bing | Mastoid + canal occlusion | Occlusion effect | Positive (louder) | Negative (no change) | Positive (louder) |
| Schwabach | Patient vs. examiner mastoid | BC vs. normal BC | Equal duration | Prolonged (patient hears longer) | Shortened (patient stops first) |
| Stenger | Both ears simultaneously | Functional loss | Responds | N/A | Positive = feigned loss |
10. CLINICAL SCENARIOS - How to Apply the Tests Together
Scenario A: Right-sided Otitis Media with Effusion (CHL)
- Weber: Lateralizes to the RIGHT (worse ear)
- Rinne Right: Negative (BC > AC)
- Rinne Left: Positive (AC > BC)
- Bing Right: Negative (no occlusion effect)
- Schwabach: Prolonged
Scenario B: Left-sided Acoustic Neuroma (SNHL)
- Weber: Lateralizes to the RIGHT (better ear)
- Rinne Left: Positive (AC > BC - but both reduced)
- Rinne Right: Positive (normal)
- Schwabach: Diminished/Shortened
Scenario C: Dead Right Ear (Profound SNHL - risk of false result!)
- Rinne Right: May appear negative (false!) - bone conduction crosses to left cochlea
- This is the False Negative Rinne / "Dead Ear" trap
- Solution: Mask the left (good) ear with a Barany box, or use the Stenger test
Scenario D: Bilateral symmetric hearing loss
- Weber: Midline (no lateralization - unhelpful)
- Rinne: Both positive (if SNHL) or both negative (if bilateral CHL)
- Weber cannot distinguish bilateral symmetric loss from normal
11. KEY MNEMONICS SUMMARY
| Mnemonic | What it helps you remember |
|---|---|
| "Rinne Negative = Not normal" | Negative Rinne = CHL |
| "Weber Worst" | Weber goes to WORST ear in CHL |
| "Weber Best" | Weber goes to BEST ear in SNHL |
| "Positive Bing = Ping!" (louder) | Normal/SNHL shows occlusion effect |
| "Short Schwabach = SNHL" | Damaged cochlea gives up first |
| "Long Schwabach = CHL" | Blocked middle ear prolongs BC |
| "Stenger Stops Sinners" | Positive Stenger = feigning |
12. LIMITATIONS & CLINICAL CONTEXT (What Examiners Expect You to Know)
-
Tuning fork tests do NOT replace audiometry - they do not quantify the magnitude of hearing loss.
-
256 Hz fork has the best sensitivity for Rinne, but 512 Hz is preferred to avoid confusing vibrotactile sensation with true hearing.
-
The Weber has the worst evidence base - Scott-Brown's explicitly states the Weber is only ~33% accurate. Use it as a screening tool, not a definitive test.
-
Masking is theoretically needed for all bone conduction tests (Barany box by air conduction), but in practice, only when the tested ear is known to be the worse ear and BC > AC.
-
Best clinical use of tuning forks: otoscopically normal ear + no audiometry available = to diagnose otosclerosis (negative Rinne in a normal-looking ear).
-
If the tympanic membrane is abnormal (effusion, perforation, cholesteatoma), there is by definition some CHL - tuning forks add minimal value. Audiometry is needed to quantify the air-bone gap.
Sources
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2, Ch. 73
- Shambaugh Surgery of the Ear
- KJ Lee's Essential Otolaryngology
- Cummings Otolaryngology Head & Neck Surgery
PTA audiogram
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I have everything I need. Now let me compile the comprehensive PTA audiogram teaching guide.
Pure Tone Audiometry (PTA) - Complete Guide
1. What is PTA?
Pure Tone Audiometry (PTA) is the gold standard bedside/clinic test for measuring hearing thresholds - the faintest sound a person can detect at each frequency. The results are plotted on a graph called the audiogram.
PTA measures:
- Air conduction (AC) - through headphones/insert earphones (tests the entire hearing system: outer + middle + inner ear)
- Bone conduction (BC) - through a bone oscillator on the mastoid (bypasses outer/middle ear, tests cochlea + auditory nerve directly)
By comparing AC and BC, you determine the type and degree of hearing loss.
2. The Audiogram - Reading the Graph
Axes
| Axis | What it shows | Range |
|---|---|---|
| X-axis (horizontal) | Frequency in Hz (logarithmic scale) | 125 - 8000 Hz |
| Y-axis (vertical) | Hearing level in dBHL (decibels Hearing Level) | -10 to 120 dBHL |
Key point about dBHL: 0 dBHL is NOT silence - it is the average threshold of a normal young adult at each frequency. The y-axis runs downward (worse hearing lower on the graph). Negative values (-5, -10 dBHL) mean better-than-average hearing.
Tested Frequencies
Standard octave frequencies: 250, 500, 1000, 2000, 4000, 8000 Hz
Inter-octave (added when steep slope suspected): 750, 1500, 3000, 6000 Hz
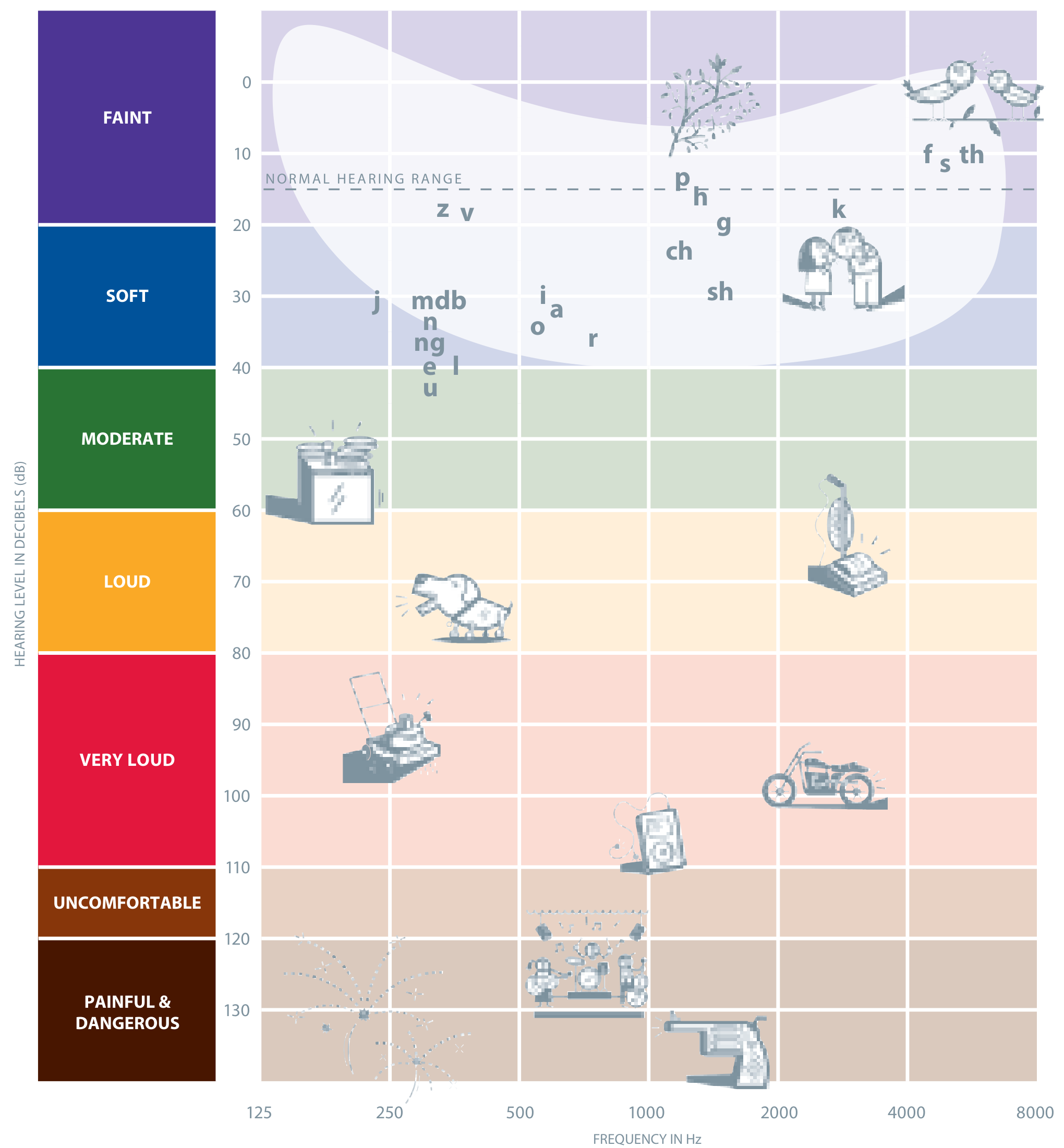
The "Speech Banana"
Speech sounds (vowels and consonants) fall between 250-8000 Hz and 20-60 dBHL. Any hearing loss in this zone affects speech understanding.
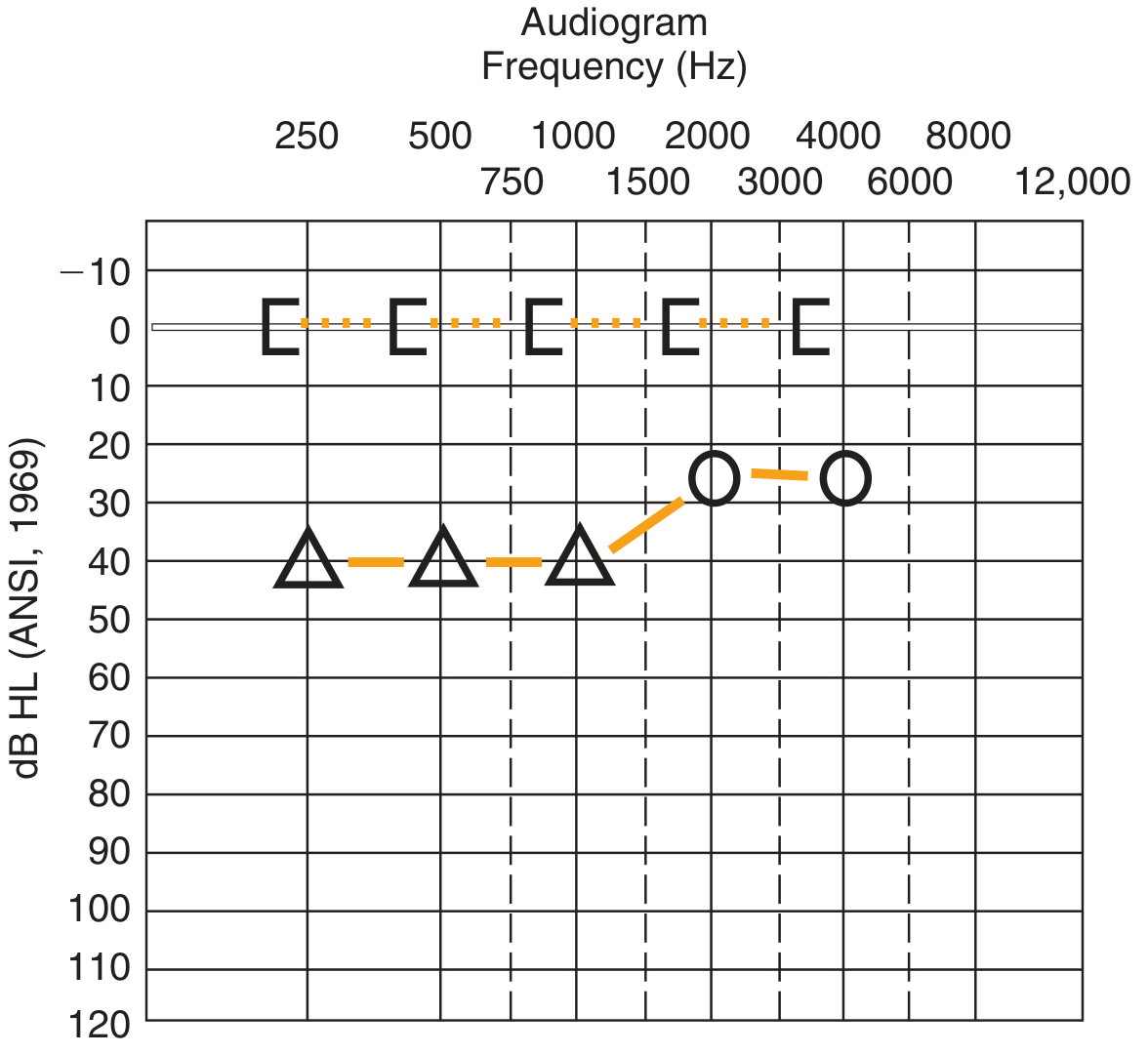
3. Audiogram Symbols - MUST MEMORISE
This is one of the most tested topics in ENT exams:
| Symbol | Colour | What it means |
|---|---|---|
| O (circle) | Red | Right ear - Air conduction (unmasked) |
| X (cross) | Blue | Left ear - Air conduction (unmasked) |
| △ (triangle) | Red | Right ear - Bone conduction (unmasked) |
| △ (triangle) | Blue | Left ear - Bone conduction (unmasked) |
| [ (square bracket facing right) | Red | Right ear - Bone conduction (masked) |
| ] (square bracket facing left) | Blue | Left ear - Bone conduction (masked) |
| ▲ (filled triangle) | Red | Right ear - AC masked |
| Points connected by solid lines | - | Right ear AC thresholds joined |
| Points connected by dashed lines | - | Bone conduction thresholds joined |
Memory trick for colours: Think of traffic lights - Red = Right, Blue = left (Blue starts with B, left has an L... or just remember "Blue is Left"). In the UK, AC for right = O (open circle), left = X (cross).
4. The Three Types of Hearing Loss - Audiogram Patterns
The Key Rule
Air-bone gap (ABG) = AC threshold minus BC threshold A gap of >10 dB at any frequency = significant ABG = conductive component present
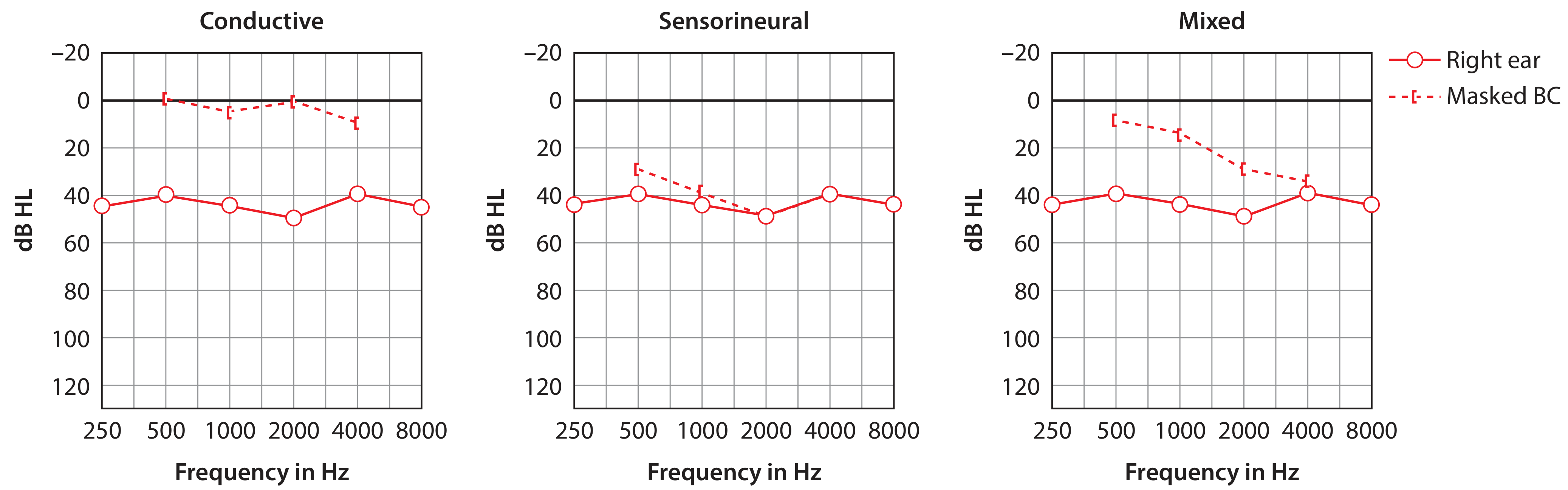
TYPE 1: Conductive Hearing Loss (CHL)
- AC: Elevated (thresholds down the graph)
- BC: Normal (at or near 0 dBHL)
- Air-bone gap: Present (>10 dB)
- Cause: Problem in outer or middle ear (wax, effusion, ossicular chain problem, perforation, otosclerosis)
- Max CHL possible: ~60 dBHL
TYPE 2: Sensorineural Hearing Loss (SNHL)
- AC: Elevated
- BC: Elevated equally to AC
- Air-bone gap: Absent (AC and BC run parallel or together)
- Cause: Cochlea (hair cells) or auditory nerve damage
- Examples: Noise-induced, presbycusis, Meniere's, acoustic neuroma, ototoxicity
TYPE 3: Mixed Hearing Loss
- AC: Elevated
- BC: Also elevated (but less than AC)
- Air-bone gap: Present (both are worse than normal, but there's still a gap between them)
- Cause: Combined middle ear + cochlear pathology (e.g., chronic otitis media with cochlear damage)
5. Degree of Hearing Loss
Shambaugh Classification (commonly used in ENT)
| Degree | Threshold Range (dBHL) |
|---|---|
| Minimal | 15 - 25 dB |
| Mild | 25 - 40 dB |
| Moderate | 40 - 55 dB |
| Moderately severe | 55 - 70 dB |
| Severe | 70 - 90 dB |
| Profound | > 90 dB |
British Society of Audiology (BSA) Classification
| Degree | Range |
|---|---|
| Mild | 21-40 dBHL |
| Moderate | 41-70 dBHL |
| Severe | 71-95 dBHL |
| Profound | ≥96 dBHL |
Normal: 0-25 dBHL (Cummings: 0-25 dB = normal)
How to Calculate: Pure Tone Average (PTA)
Average the AC thresholds at: 500 + 1000 + 2000 + 4000 Hz ÷ 4
(Some centres use 500, 1000, 2000 Hz only - the "Fletcher average")
6. Threshold Testing Method (How it's Done)
Standard modified Hughson-Westlake method:
- Start at 1000 Hz (most reliable frequency)
- Present a tone - if heard, decrease by 10 dB; if not heard, increase by 5 dB
- Threshold = lowest level heard on at least 2 out of 3 ascending presentations
- Test order: 1000 → 2000 → 4000 → 8000 → 1000 (re-check) → 500 → 250 Hz
- Test the better ear first
- Then repeat with bone conduction oscillator on mastoid
7. Masking - Critical Concept
Why is masking needed?
Bone conduction testing delivers sound that crosses the skull (interaural attenuation for BC is ~0 dB - i.e., essentially zero). So when you test the right ear by BC, the left cochlea can hear it too. This creates a shadow curve - a false threshold from the non-test ear.
Similarly, for air conduction there is ~40-65 dB of interaural attenuation, but if the test ear is much worse than the other, the sound still crosses over.
When to mask?
For bone conduction: Always (or whenever there is any asymmetry).
For air conduction: When the AC threshold in the test ear exceeds the BC threshold of the non-test ear by 40 dB or more.
How to mask?
Apply narrow-band noise to the non-test ear via the earphone, at a level sufficient to prevent it from hearing the test signal. The masked BC symbols are the bracket symbols [ ] instead of triangles.
The "Masking Dilemma"
When both ears have large air-bone gaps, masking the non-test ear may inadvertently mask the test ear through bone conduction - an insoluble clinical problem. In this situation, tuning forks are particularly valuable (this is one of their key roles in 2026 ENT practice).
8. The Pure Tone Average and Its Clinical Uses
Speech Reception Threshold (SRT) cross-check
The SRT (lowest level at which speech is recognised) should be within ±10 dB of the PTA. If not, suspect:
- Non-organic (functional) hearing loss
- Central auditory processing disorder
- Test reliability issues
Fletcher Index / PTA for Medicolegal Use
For disability assessment and hearing aid prescription:
PTA = (500 + 1000 + 2000 + 3000 Hz) ÷ 4 (or 500 + 1000 + 2000 alone in some systems)
9. Classic Audiogram Patterns You Must Know for Exams
| Pattern | Shape | Condition |
|---|---|---|
| Carhart notch | BC dip at 2000 Hz | Otosclerosis |
| Noise notch | AC dip at 4000 Hz | Noise-induced hearing loss (NIHL) |
| Cookie bite / U-shaped | Loss in mid-frequencies | Genetic hearing loss (Autosomal Dominant) |
| Rising (low-frequency loss) | Worse at low frequencies | Meniere's disease (early) |
| Flat loss | Equal at all frequencies | Various; congenital |
| Steeply sloping (ski-slope) | Much worse at high frequencies | Presbycusis, cochlear SNHL |
| Dead ear / no response | No symbol plotted (or use "NR") | Profound SNHL / anacusis |
Carhart Notch - Key Exam Fact
A BC dip specifically at 2000 Hz in an otherwise conductive pattern. It is a mechanical artefact of stapes fixation - when the ossicular chain is fixed (as in otosclerosis), the skull cannot resonate normally at 2 kHz during BC testing. It is NOT a true sensorineural component.
Proof: After successful stapedectomy, the Carhart notch disappears and the BC thresholds improve (on average ~12 dB at 0.5, 1, and 2 kHz). This is the Carhart effect - post-operative "over-closure" of the air-bone gap appears because the pre-op BC thresholds included the artefactual notch.
Noise-Induced Hearing Loss (NIHL) - 4 kHz Notch
Noise damages the basal turn of the cochlea (which processes high frequencies). The notch typically appears at 4000 Hz (sometimes 3000 or 6000 Hz) with relative recovery at 8000 Hz. AC and BC both show the notch (SNHL pattern - no air-bone gap).
10. Audiogram + Tuning Fork Cross-Reference
| Audiogram Finding | Tuning Fork Expected |
|---|---|
| AC elevated, BC normal (CHL) | Rinne negative; Weber to affected ear; Bing negative; Schwabach prolonged |
| AC = BC elevated (SNHL) | Rinne positive; Weber to better ear; Bing positive; Schwabach shortened |
| AC and BC elevated, gap present (Mixed) | Rinne negative; Weber variable (depends on which component dominates) |
| Carhart notch at 2000 Hz | Rinne negative (CHL is the dominant finding in otosclerosis) |
11. Quick Summary Cheat Sheet
AUDIOGRAM AT A GLANCE
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
X-axis: Frequency (Hz) - low (bass) LEFT → high (treble) RIGHT
Y-axis: Hearing Level (dBHL) - better ABOVE, worse BELOW
0 dBHL: Average normal threshold (not silence!)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
SYMBOLS: O = Right AC | X = Left AC (both unmasked)
[ = Right BC masked | ] = Left BC masked
△ = BC unmasked (either side)
Right = RED | Left = BLUE
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
TYPES:
CHL → AC down, BC normal → BIG GAP
SNHL → AC down, BC down equally → NO GAP
Mixed → AC down, BC down (less) → GAP still present
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
PATTERNS:
2 kHz BC notch = Carhart (otosclerosis)
4 kHz AC notch = Noise (NIHL)
Low-freq loss = Meniere's
Cookie bite = Autosomal dominant HL
Ski-slope = Presbycusis / cochlear SNHL
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
DEGREE (Shambaugh):
Mild 25-40 | Moderate 40-55 | Mod-severe 55-70
Severe 70-90 | Profound >90
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Sources: Scott-Brown's Otorhinolaryngology Vol 2 (Ch. 51); Cummings Otolaryngology (Ch. 134); Shambaugh Surgery of the Ear
PTA audiogram
Asking for Preferences
PTA audiogram
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.