Portal hypertension pathology
Reading File
Finding Sources
Searching PubMed
"portal hypertension" pathophysiology
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive, well-illustrated answer. Here is the full response:
Portal Hypertension - Pathology
Definition and Pressure Thresholds
Portal hypertension is defined as a sustained elevation in portal venous pressure. Clinically, it is assessed using the hepatic venous pressure gradient (HVPG) - the difference between wedged and free hepatic venous pressures, measured by hepatic vein catheterization:
- Normal HVPG: up to 5 mmHg
- Clinically significant portal hypertension: HVPG >10-12 mmHg (threshold for ascites and other manifestations)
- High mortality risk: HVPG >16 mmHg
- Treatment failure / acute variceal bleeding mortality: HVPG >20 mmHg
(Sleisenger & Fordtran's Gastrointestinal and Liver Disease)
Classification by Site of Resistance
The standard anatomic classification divides causes into three levels (Harrison's, 22e):
Prehepatic
Obstruction before the blood enters the liver:
- Portal vein thrombosis (most common prehepatic cause)
- Splenic vein thrombosis
- Massive splenomegaly / Banti's syndrome
Intrahepatic (>95% of all cases)
Further subdivided by level within the liver:
| Sub-level | Causes |
|---|---|
| Presinusoidal | Schistosomiasis, congenital hepatic fibrosis, primary biliary cholangitis (early), nodular regenerative hyperplasia, sarcoidosis |
| Sinusoidal | Cirrhosis (any etiology - alcoholic, viral, NAFLD/NASH, autoimmune), alcoholic hepatitis, amyloidosis, massive fatty change, infiltrative malignancy |
| Postsinusoidal | Hepatic sinusoidal obstruction syndrome (venoocclusive disease) |
Posthepatic
Obstruction of hepatic venous outflow:
- Budd-Chiari syndrome (hepatic vein outflow obstruction)
- Inferior vena caval webs
- Constrictive pericarditis / severe right-sided heart failure / restrictive cardiomyopathy
Note: Alcohol-associated cirrhosis often causes increased resistance at presinusoidal, sinusoidal, AND postsinusoidal levels simultaneously, so rigid anatomic classification does not always apply. - Sleisenger & Fordtran's
Pathophysiology
The mechanism of portal hypertension is dual: increased intrahepatic resistance + increased portal blood flow from a hyperdynamic circulation.
1. Increased Intrahepatic Resistance (Structural + Functional)
In cirrhosis, two components operate together:
Structural (fixed) component:
- Progressive collagen deposition and regenerative nodule formation distort sinusoidal architecture
- Parenchymal nodules physically compress sinusoids and disrupt normal blood flow patterns
- Sinusoidal remodeling and arterio-portal anastomoses within fibrous septa impose arterial pressures on the low-pressure portal venous system
Dynamic (functional) component:
- Contraction of hepatic stellate cells (HSCs) and hepatic endothelial cells increases vascular tone
- Altered sinusoidal endothelial cell function:
- Decreased nitric oxide (NO) production (despite NO overproduction in the splanchnic bed - a key paradox)
- Increased release of endothelin-1, angiotensinogen, and eicosanoids
- The net result is intrahepatic vasoconstriction superimposed on structural obstruction
(Robbins, Cotran & Kumar Pathologic Basis of Disease)
2. Increased Portal Blood Flow (Hyperdynamic Circulation)
Portal hypertension triggers release of vasodilating mediators - principally NO, but also prostacyclin, TNF-alpha, carbon monoxide, and endogenous endocannabinoids - predominantly into the splanchnic circulation.
This produces:
- Splanchnic arterial vasodilation → decreased splanchnic vascular resistance
- Increased splanchnic arterial inflow → increased venous efflux back into the portal system
- The portal pressure is thus maintained and amplified even as shunts develop
The arterial vasodilatation theory (1988) describes the resulting systemic consequences:
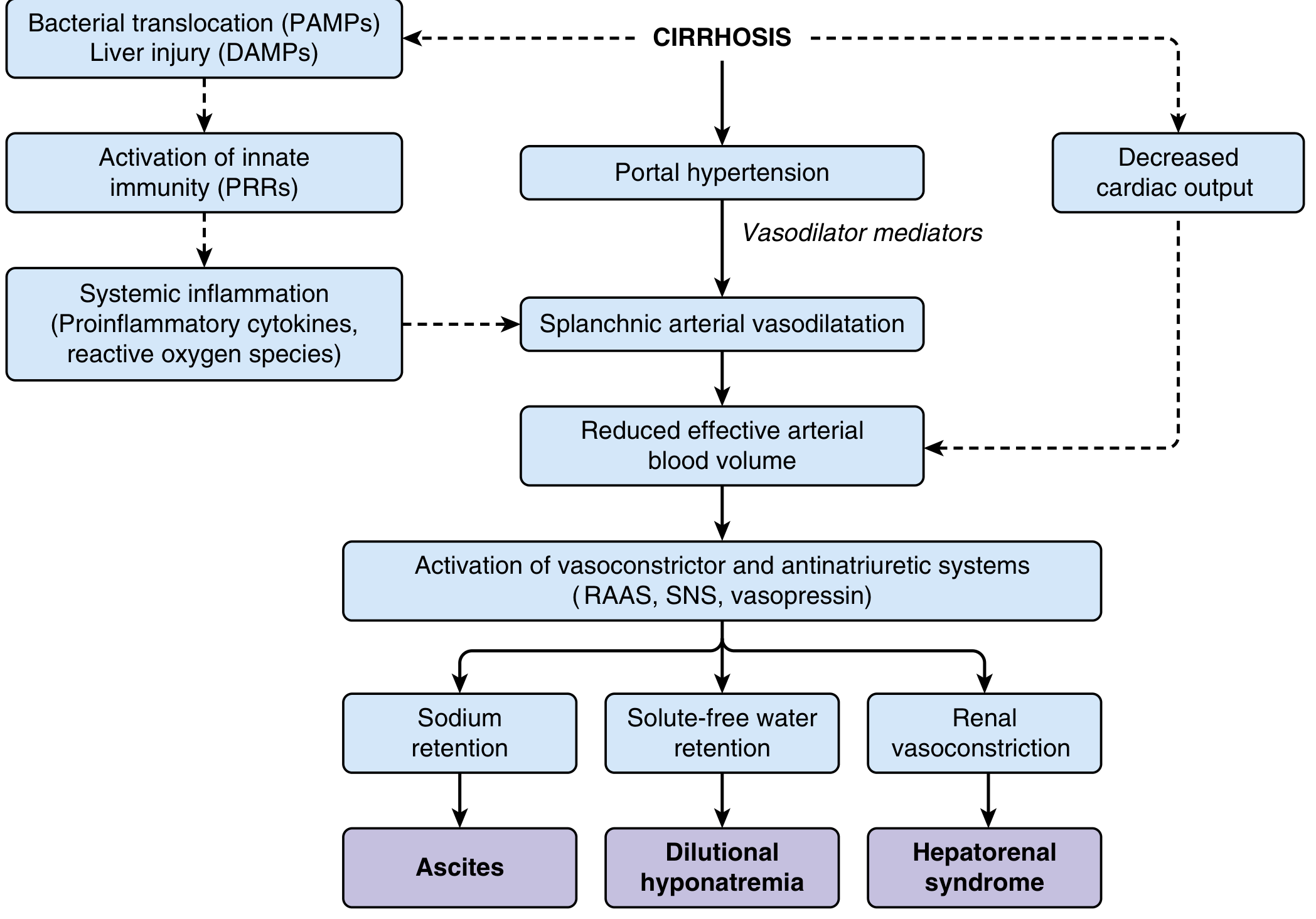
Early cirrhosis: Moderate splanchnic vasodilation is compensated by increased cardiac output; arterial pressure is maintained.
Advanced cirrhosis: Intense splanchnic vasodilation creates effective arterial hypovolemia (intravascular blood volume "insufficient" for the enlarged vasodilated arterial circuit). Cardiac output also falls. Compensatory activation of:
- RAAS (renin-angiotensin-aldosterone) → sodium retention → ascites
- Sympathetic nervous system (SNS) → renal vasoconstriction
- Vasopressin (ADH) (late stage) → solute-free water retention → dilutional hyponatremia
At the extreme, renal vasoconstriction reduces GFR → hepatorenal syndrome (HRS).
Simultaneously, systemic inflammation is driven by:
- PAMPs from bacterial translocation (gut dysbiosis in cirrhosis)
- DAMPs from injured hepatocytes
- Activation of innate immunity via pattern recognition receptors (PRRs)
- Release of proinflammatory cytokines and reactive oxygen species → further circulatory impairment
Four Major Consequences of Portal Hypertension
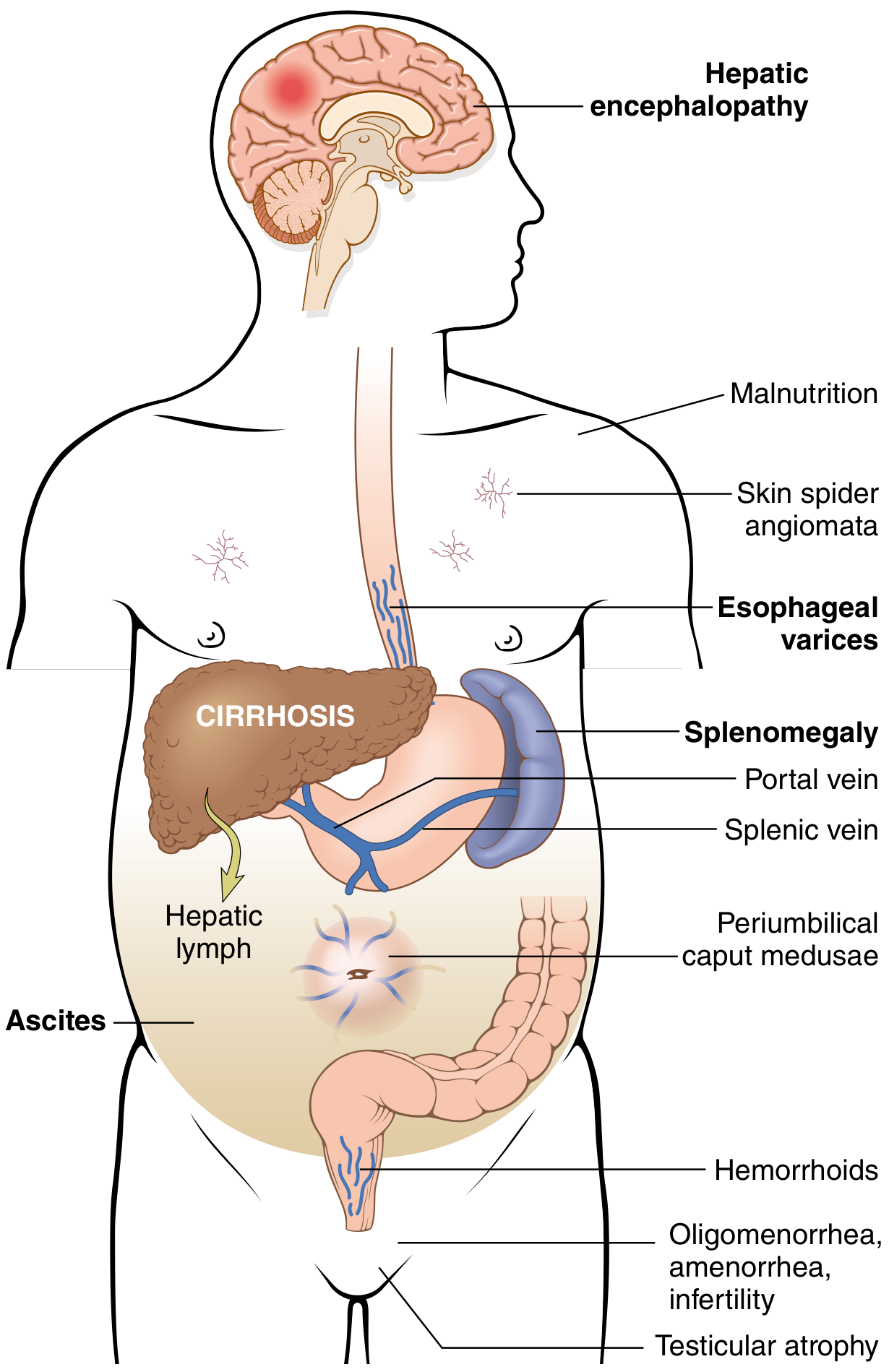
1. Ascites
- Clinically detectable at >500 mL accumulation
- Fluid is serous, protein <3 g/dL, SAAG (serum-ascites albumin gradient) ≥1.1 g/dL
- Pathogenesis: sinusoidal hypertension + hypoalbuminemia + increased hepatic lymph flow + splanchnic vasodilation
- Longstanding ascites can track through transdiaphragmatic lymphatics → right-sided hepatic hydrothorax
2. Portosystemic Venous Shunts (Varices)
Chronic portal hypertension causes dilation and remodeling of pre-existing portal-systemic anastomoses at 4 principal sites:
| Site | Clinical Manifestation |
|---|---|
| Esophagogastric junction | Esophageal/gastric varices - most dangerous |
| Periumbilical / abdominal wall | Caput medusae (dilated subcutaneous veins radiating from umbilicus) |
| Rectum | Hemorrhoids |
| Retroperitoneum | Retroperitoneal varices |
Esophageal varices develop in ~40% of advanced cirrhotics. About one-third of patients with varices will bleed; each bleeding episode carries ~30% mortality. About 1/3 of histologically confirmed cirrhotics have varices; 5-15% per year develop new ones. (Robbins; Harrison's)
Risk factors for variceal bleeding include: Child-Pugh/MELD score severity, HVPG >12 mmHg, varix size and location, red wale signs, cherry red spots, and tense ascites.
3. Congestive Splenomegaly
- Longstanding portal hypertension causes passive congestion of the spleen
- Splenic weight can reach up to 1000 g (5-6x normal)
- Leads to hypersplenism: sequestration of blood elements in the expanded splenic red pulp → thrombocytopenia, leukopenia, and sometimes pancytopenia
- Thrombocytopenia is often the earliest laboratory clue to portal hypertension
4. Hepatic Encephalopathy
- Portal blood bypasses the liver through portosystemic shunts
- Toxic metabolites (notably ammonia, NH₃) that normally are cleared/detoxified by the liver enter the systemic circulation
- Crossing the blood-brain barrier causes neuropsychiatric dysfunction ranging from subtle cognitive changes to frank delirium and coma
Pulmonary Complications
Two distinct pulmonary syndromes arise in advanced portal hypertension:
| Syndrome | Mechanism | Key Feature |
|---|---|---|
| Hepatopulmonary syndrome | Dilation of intrapulmonary capillaries/precapillaries (up to 500 µm) → right-to-left shunting → V/Q mismatch | Hypoxemia worse in upright position (orthodeoxia); occurs in up to 30% of cirrhotics |
| Portopulmonary hypertension | Pulmonary arterial hypertension in the setting of portal hypertension | Dyspnea on exertion; right heart strain on echo |
(Robbins Pathologic Basis of Disease)
Additional Systemic Complications (Sleisenger & Fordtran's)
- Hepatorenal syndrome - extreme renal vasoconstriction
- Dilutional hyponatremia - ADH-driven free water retention
- Spontaneous bacterial peritonitis (SBP) - seeding of ascitic fluid
- Coagulopathy - impaired synthetic function + hypersplenism
- Hypogonadism - oligomenorrhea, amenorrhea, testicular atrophy
- Hepatic hydrothorax - transdiaphragmatic fluid migration (usually right-sided)
Assessment
- HVPG measurement (hepatic vein catheterization): gold standard for pressure quantification
- Liver stiffness by transient elastography (FibroScan): non-invasive surrogate; values >20 kPa suggest high-risk varices; can be overestimated post-prandially, in hepatic inflammation, cholestasis, or right heart failure
- Endoscopy: screening for varices at diagnosis of compensated cirrhosis, then every 2-3 years
- CT/MRI: nodular liver contour, portal vein dilation, intraabdominal collaterals, splenomegaly
- Labs: thrombocytopenia (often the first sign), hypoalbuminemia, coagulopathy
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease | Harrison's Principles of Internal Medicine 22e | Sleisenger & Fordtran's Gastrointestinal and Liver Disease | Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.