Ventilation-perfusion ratio.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Here is a thorough breakdown of the ventilation-perfusion (V/Q) ratio, drawn from Costanzo Physiology, Guyton & Hall, and Murray & Nadel's Textbook of Respiratory Medicine.
Ventilation-Perfusion (V/Q) Ratio
Definition
The V/Q ratio is the ratio of alveolar ventilation (VA, in L/min) to pulmonary blood flow/perfusion (Q, in L/min). Matching ventilation to perfusion is the fundamental requirement for efficient gas exchange - it is useless for alveoli to be ventilated but not perfused, or perfused but not ventilated.
- Costanzo Physiology, p. 233
Normal Value
- Normal V/Q = 0.8
- At rest: alveolar ventilation ~4 L/min, pulmonary blood flow ~5 L/min
- At this ratio: PaO2 = 100 mm Hg, PaCO2 = 40 mm Hg
- If V/Q changes (due to altered ventilation, altered perfusion, or both), gas exchange becomes suboptimal
How V/Q Determines Alveolar Gas Composition
The PO2, PCO2, and PN2 in any gas-exchanging unit are uniquely determined by three factors:
- The ventilation-perfusion ratio
- The composition of inspired gas and mixed venous blood
- The slopes and positions of the relevant blood-gas dissociation curves
When the V/Q ratio increases (more ventilation relative to perfusion), alveolar PO2 rises and PCO2 falls. When V/Q decreases, alveolar PO2 falls and PCO2 rises.
- Guyton & Hall Medical Physiology, p. 517
Regional Distribution of V/Q in the Upright Lung
Both ventilation and blood flow vary by gravity in the upright lung, but blood flow varies more steeply than ventilation. This creates a V/Q gradient from apex to base.
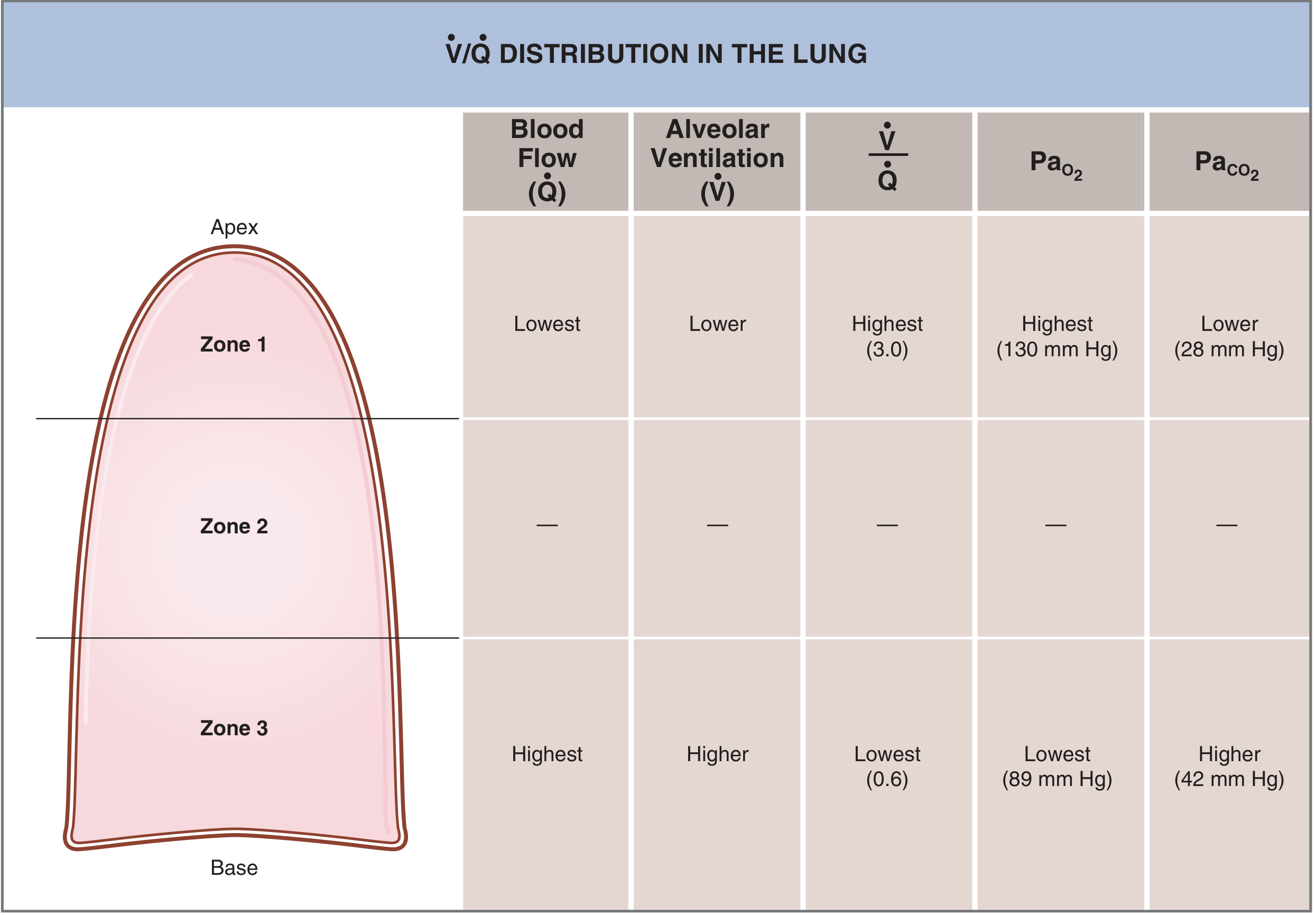
| Zone | Blood Flow | Ventilation | V/Q | PaO2 | PaCO2 |
|---|---|---|---|---|---|
| Zone 1 (Apex) | Lowest | Lower | Highest (~3.0) | 130 mm Hg | 28 mm Hg |
| Zone 2 (Mid) | Intermediate | Intermediate | ~1.0 | ~108 mm Hg | ~39 mm Hg |
| Zone 3 (Base) | Highest | Higher | Lowest (~0.6) | 89 mm Hg | 42 mm Hg |
Why? At the apex, blood flow falls more than ventilation, so V/Q is high (physiological dead space tendency). At the base, blood flow increases more than ventilation, so V/Q is low (physiological shunt tendency). The average across the whole lung = 0.8.
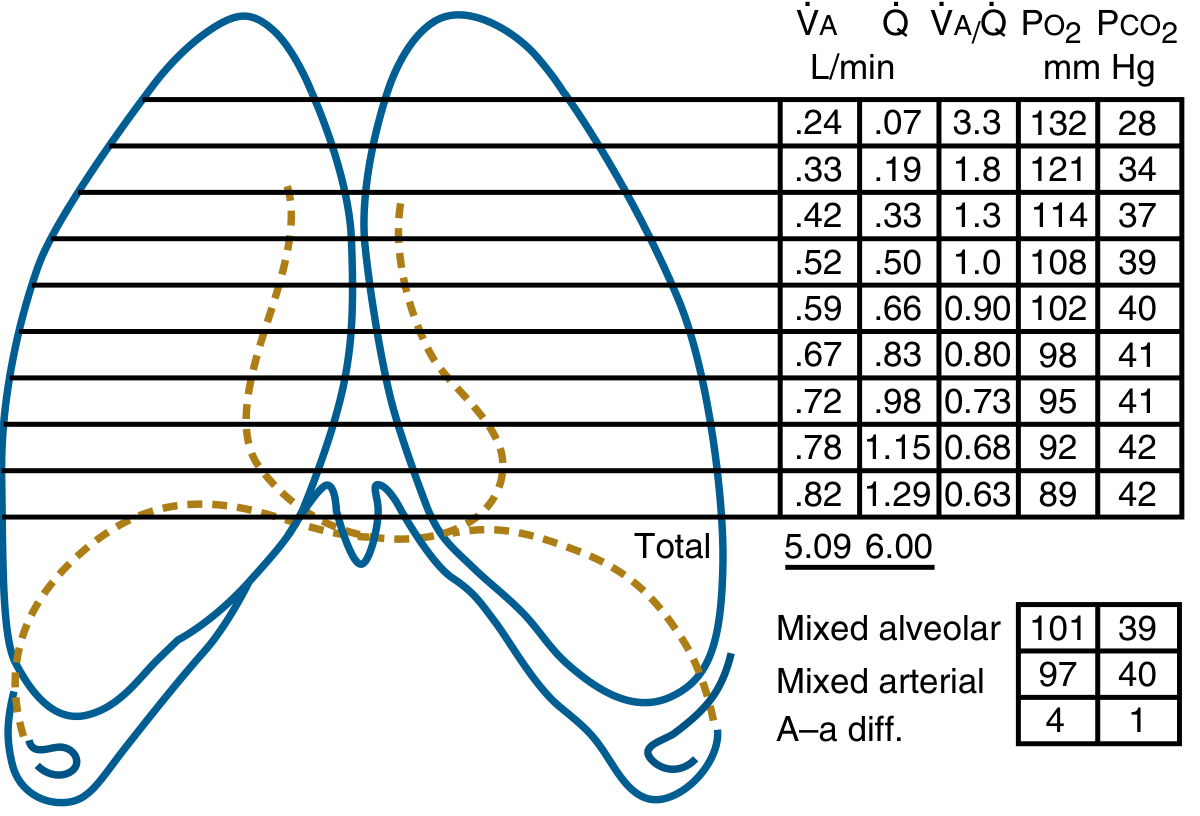
The regional differences in PaO2 are much greater (apex to base range ~40 mm Hg) than the differences in PaCO2 (range ~14 mm Hg). Overall, normal gravitational V/Q inequality reduces arterial PO2 by only about 4 mm Hg from what a perfectly homogeneous lung would achieve.
- Murray & Nadel, p. 240-241; Costanzo Physiology, p. 234
The regional data from 9 lung slices (Murray & Nadel):
V/Q Extremes and Defects
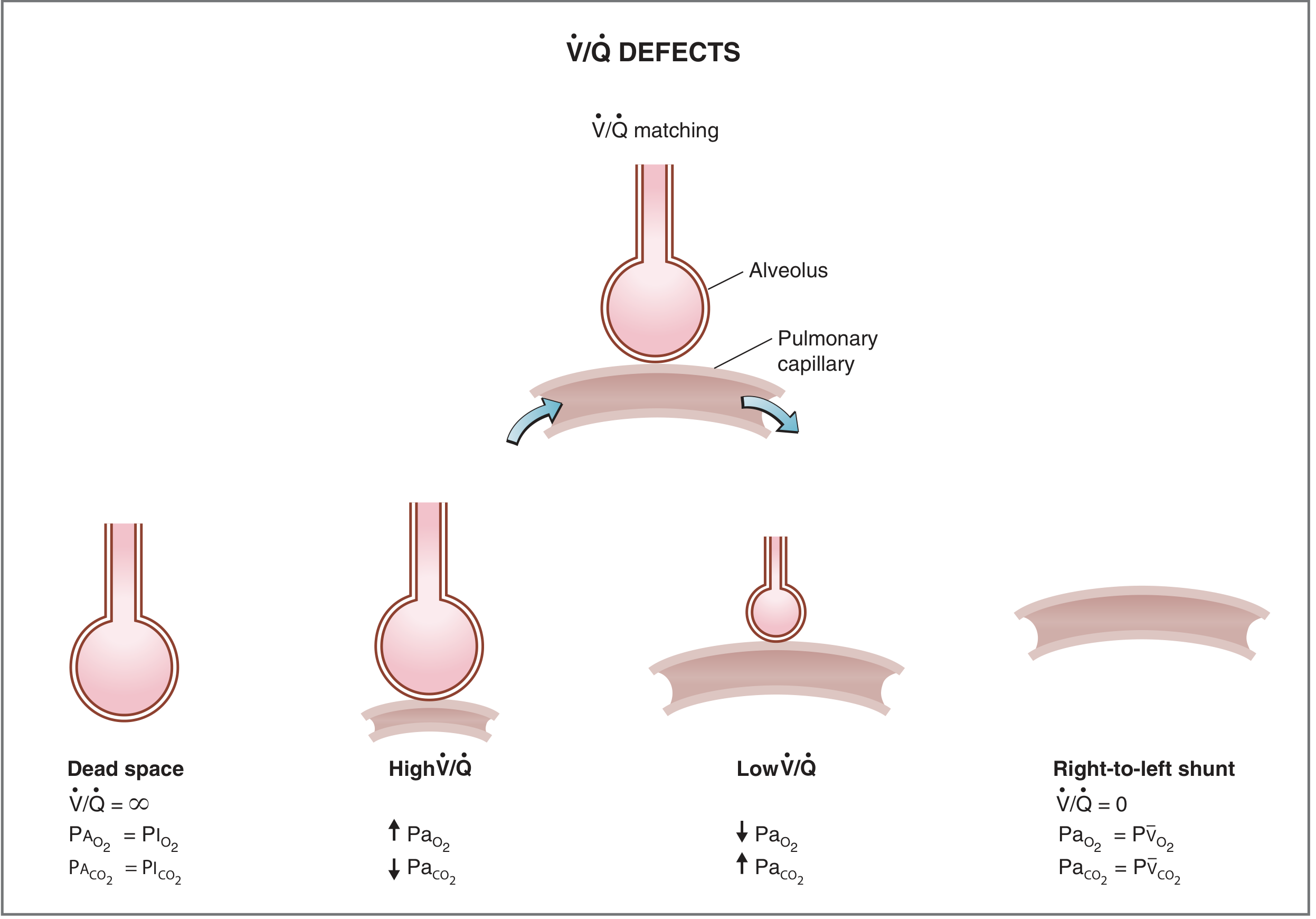
1. Dead Space (V/Q = ∞)
- Ventilation with no perfusion
- Alveolar gas equilibrates with inspired air (not blood)
- PAO2 = 150 mm Hg, PACO2 = 0 mm Hg
- No gas exchange is possible
- Clinical example: Pulmonary embolism
2. High V/Q
- Ventilation is high relative to perfusion (reduced blood flow, but some flow still present)
- PaO2 is high, PaCO2 is low
- Represents wasted ventilation (physiological dead space)
3. Low V/Q
- Perfusion is high relative to ventilation (reduced airflow, but some airflow still present)
- PaO2 is low, PaCO2 is high
- Blood leaves poorly oxygenated
4. Right-to-Left Shunt (V/Q = 0)
- Perfusion with no ventilation
- Alveolar gas equilibrates with mixed venous blood
- PaO2 = 40 mm Hg, PaCO2 = 46 mm Hg (venous values)
- No gas exchange is possible
- Clinical examples: Airway obstruction, right-to-left cardiac shunt
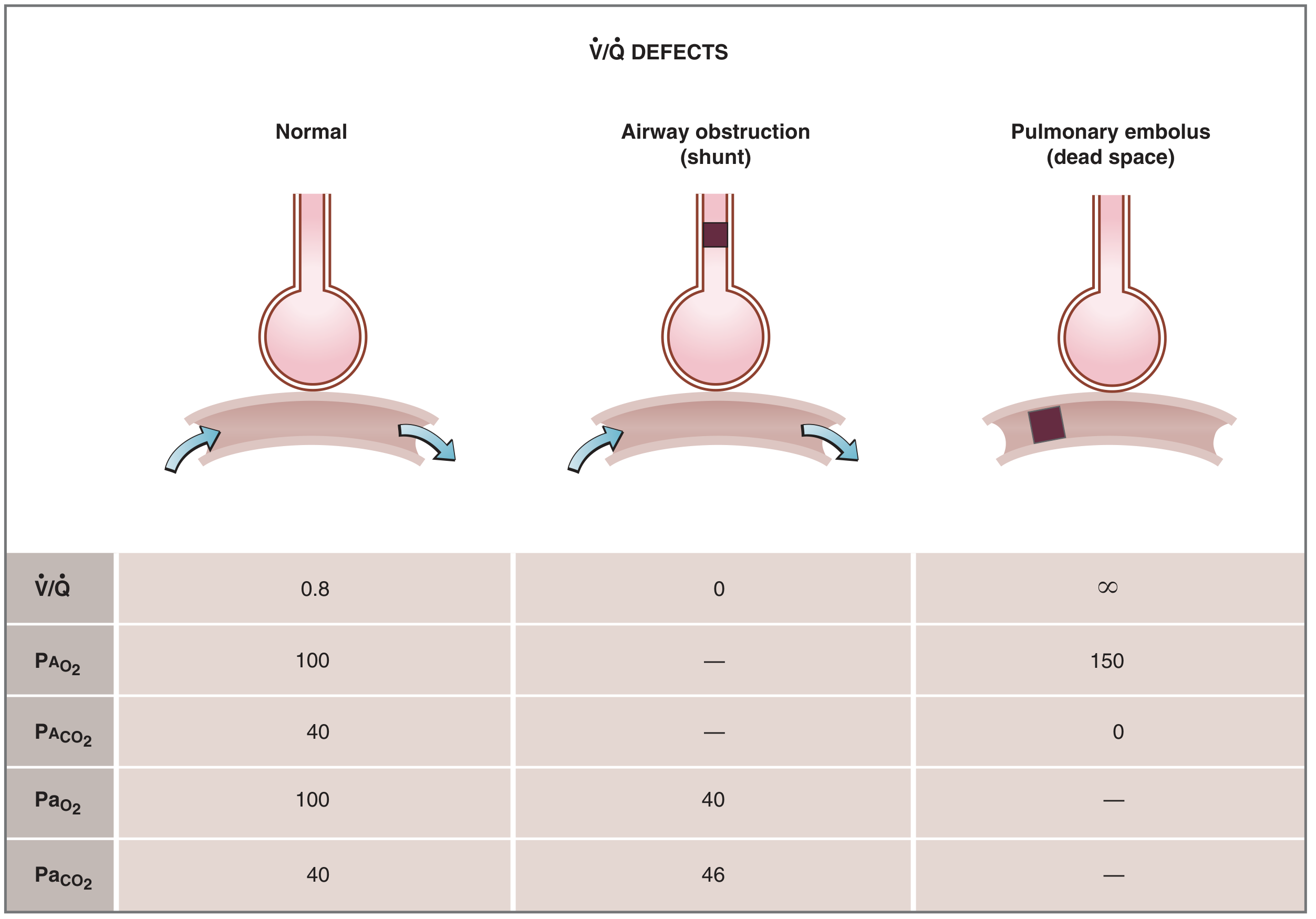
V/Q Mismatch in Disease
| Condition | Mechanism | V/Q Effect |
|---|---|---|
| Pulmonary embolism | Blocked blood flow | V/Q → ∞ (dead space) |
| Airway obstruction (mucus plug, bronchospasm) | Blocked airflow | V/Q → 0 (shunt) |
| Pneumonia/atelectasis | Alveoli filled/collapsed, no airflow | V/Q → 0 (shunt) |
| COPD/emphysema | Both obstruction (V/Q → 0) AND destroyed walls (V/Q → ∞) | Mixed dead space + shunt |
| Normal upright lung | Gravitational gradient | 0.6 (base) to 3.0 (apex) |
In COPD, some obstructed alveoli have V/Q near zero (physiological shunt), while adjacent destroyed alveolar walls cause V/Q near infinity (physiological dead space). Both decrease lung effectiveness, sometimes to as little as one-tenth of normal - making this the most prevalent cause of pulmonary disability.
- Guyton & Hall, p. 520
Key Clinical Points
- V/Q mismatch is the most common cause of hypoxemia in pulmonary disease
- Shunt (V/Q = 0) does not respond well to supplemental O2, because the affected alveoli never receive oxygen regardless of FiO2
- Dead space (V/Q = ∞) raises the alveolar-arterial (A-a) gradient and increases the work of breathing
- The A-a O2 gradient is the classic bedside tool for detecting V/Q inequality: normal A-a diff = ~4 mm Hg (as shown in the regional data above); elevated in shunt, dead space, and diffusion defects
- Arterial PCO2 is a poor indicator of V/Q inequality (too sensitive to ventilation level); arterial PO2 is more informative
- Multiple inert gas elimination technique (MIGET) - developed by Wagner et al. - is the gold standard research method for quantifying the full distribution of V/Q ratios in a lung
Sources: Costanzo Physiology 7th ed. | Guyton and Hall Textbook of Medical Physiology | Murray & Nadel's Textbook of Respiratory Medicine
Can you tell me all the, um, reasoning questions that are asked in university exams of first year MBBS in the topic respiratory physiology? Please.
Asking for Preferences
Finding Sources
Searching the Web
1st year MBBS respiratory physiology reasoning questions India NMC university exam "give reasons"
Reading Web Page
https://medical.iqcity.in/wp-content/uploads/2021/03/1st-Pro…
Searching the Web
first MBBS physiology respiratory system "explain why" "give reasons" university question bank India
I now have all the material I need. Let me compile the comprehensive list.
Reasoning Questions - Respiratory Physiology (1st Year MBBS, NMC/India Pattern)
These are "Give Reasons / Explain Why / Applied" type questions drawn from university question banks, past papers (IQ City, MGMUHS, and others), and the NMC CBME syllabus. They are organized topic-wise across the full respiratory physiology curriculum.
1. Mechanics of Breathing
-
Why is intrapleural pressure always negative? (Lung elastic recoil always tends to pull lung away from chest wall - the pleural space is a closed cavity maintained below atmospheric pressure to keep lungs expanded.)
-
Why does the diaphragm move downward during inspiration despite being a dome-shaped muscle? (Diaphragm contraction flattens the dome, increasing thoracic volume vertically.)
-
Why does expiration at rest require no muscular effort but forced expiration does? (Quiet expiration is passive - driven by elastic recoil of lungs and chest wall. Forced expiration recruits internal intercostals and abdominal muscles.)
-
Why does intrapleural pressure become more negative during inspiration? (Thoracic volume increases, lung recoil resists expansion - creating a larger pressure gradient.)
-
Why do premature babies develop Respiratory Distress Syndrome (IRDS/Hyaline Membrane Disease)? (Surfactant is produced after 28-32 weeks; deficiency increases surface tension, causing alveolar collapse - atelectasis.)
-
Why does surface tension tend to collapse alveoli, and how does surfactant prevent this? (Laplace's law: P = 2T/r; surfactant reduces surface tension, especially in small alveoli, preventing collapse.)
-
Why don't small alveoli empty into large alveoli (alveolar instability)? (Surfactant lowers surface tension more in small alveoli than large ones, equalizing pressures - prevents emptying by Laplace's law.)
-
Why is lung compliance reduced in pulmonary fibrosis? (Fibrotic tissue is stiffer - requires more pressure to achieve the same volume change.)
-
Why is lung compliance increased in emphysema? (Destruction of elastic tissue in alveolar walls reduces elastic recoil, making lungs easier to distend.)
-
Why is the FRC the resting position of the lungs? (At FRC, outward recoil of chest wall and inward recoil of lungs balance - net force is zero.)
2. Lung Volumes and Capacities
-
Why can't residual volume (RV) be measured by simple spirometry? (RV is the air that remains after maximum forced expiration - it cannot be exhaled out, so spirometry cannot detect it. Requires helium dilution or body plethysmography.)
-
Why is FRC increased in emphysema? (Loss of elastic tissue reduces inward lung recoil - the balance point between lung and chest wall shifts outward, increasing resting lung volume.)
-
Why is there a barrel-shaped chest in emphysema? (Chronically increased Total Lung Capacity due to air trapping and over-inflation pushes chest wall permanently outward.)
-
Why is FEV1/FVC ratio decreased in obstructive lung disease but normal or increased in restrictive lung disease? (In obstruction, airflow is limited (FEV1 falls more than FVC). In restriction, both FVC and FEV1 fall proportionally - ratio preserved or raised.)
-
Why is timed vital capacity (FEV1) a better test of airway obstruction than simple VC? (FVC measures volume, but obstruction impedes flow rate - FEV1 captures the rate of emptying, revealing airflow limitation even when total volume is preserved.)
3. Ventilation-Perfusion (V/Q) Ratio
-
Why is V/Q ratio higher at the apex and lower at the base of the lung in the upright position? (Gravity reduces blood flow more at the apex than ventilation - blood flow decreases more steeply apex to base than ventilation does.)
-
Why is PO2 higher and PCO2 lower at the lung apex compared to the base? (Higher V/Q at the apex means relatively more ventilation per unit blood flow - more O2 is delivered per unit blood, and CO2 is better washed out.)
-
Why is pulmonary embolism an example of dead space and not shunt? (PE blocks perfusion to ventilated alveoli - V/Q → ∞ (dead space). Shunt is the opposite - perfusion without ventilation.)
-
Why does hypoxemia in shunt not respond to 100% O2 therapy? (In complete shunt, V/Q = 0 - the shunted blood never reaches ventilated alveoli, so increasing FiO2 cannot oxygenate it.)
-
Why does V/Q mismatch cause hypoxemia more readily than hypercapnia? (CO2 has a steeper, more linear dissociation curve and higher diffusion capacity; the body can compensate by increasing ventilation to well-ventilated areas to eliminate CO2, but cannot compensate for O2 due to the flat portion of the oxyhemoglobin curve.)
4. Diffusion and Gas Exchange
-
Why is CO2 diffusion capacity 20 times more than O2, yet CO2 is not diffusion-limited? (CO2 is ~20x more soluble in tissue fluid, making its diffusion very rapid. It is not diffusion-limited under normal conditions.)
-
Why is CO used to measure diffusing capacity of lungs (DLCO)? (CO has an extremely high affinity for Hb (~240x that of O2) - its partial pressure in pulmonary capillary blood remains near zero, ensuring the entire pressure gradient is maintained across the membrane throughout the capillary.)
-
Why is O2 transfer perfusion-limited under normal conditions? (O2 equilibrates between alveolar air and capillary blood in the first one-third of the capillary transit time - so transfer is limited by how much blood flows, not by diffusion.)
-
Why does O2 transfer become diffusion-limited during heavy exercise at high altitude? (Capillary transit time is shortened by increased cardiac output + low alveolar PO2 flattens the diffusion gradient - equilibration is not completed before blood leaves the capillary.)
-
Why is the partial pressure of O2 in alveolar air (PAO2) less than in inspired air? (Alveolar air is diluted by residual CO2 from blood and water vapor; O2 is continuously extracted.)
5. Oxygen Transport
-
Why is the O2-Hb dissociation curve sigmoid-shaped? (Cooperative binding - each O2 bound to Hb increases the affinity of remaining heme groups for the next O2 molecule.)
-
Why does the O2-Hb dissociation curve shift to the right (Bohr effect)? (Increase in PCO2, H+, temperature, or 2,3-DPG reduces Hb's affinity for O2 - facilitates unloading at tissues.)
-
Why is 2,3-DPG increased in chronic anemia and at high altitude? (Compensatory mechanism - increased 2,3-DPG shifts the curve right, promoting O2 unloading to tissues when O2 supply is reduced.)
-
Why does CO poisoning cause more severe hypoxia than anemic hypoxia of the same degree? (CO binds Hb 240x more avidly than O2, and the remaining Hb shifts its curve to the left (Haldane effect) - reducing both O2 carrying capacity AND O2 release to tissues.)
-
Why is O2 therapy not very useful in anemic hypoxia? (In anemic hypoxia, PaO2 and % saturation are already normal - there are simply fewer Hb molecules. Dissolved O2 increases only slightly with therapy and cannot compensate for the loss of Hb-bound O2.)
-
Why is cyanosis absent in CO poisoning despite severe hypoxia? (Cyanosis requires >5 g/dL of reduced (deoxygenated) Hb in capillaries. In CO poisoning, Hb is bound to CO (carboxyhemoglobin - cherry red), not reduced Hb, so the skin appears red, not blue.)
-
Why does cyanosis not occur in severe anemia even with hypoxia? (Total Hb is too low - even if a large proportion is deoxygenated, the absolute amount of reduced Hb rarely exceeds the 5 g/dL threshold needed to produce visible cyanosis.)
6. Carbon Dioxide Transport
-
Why is most CO2 transported as bicarbonate and not dissolved? (CO2 is converted to HCO3- by carbonic anhydrase in RBCs - this is far more efficient than simple dissolution and accounts for ~70% of CO2 transport.)
-
Why does RBC swell (increase in size) in venous blood compared to arterial blood? (In tissues, CO2 enters RBCs → carbonic anhydrase converts it to H+ + HCO3-. HCO3- exits into plasma via chloride shift (Cl- enters). Water follows osmotically → RBC swells.)
-
Why is PCO2 more important than PO2 in stimulating central chemoreceptors? (Central chemoreceptors respond to changes in CSF H+ (pH) - CO2 crosses the blood-brain barrier freely and lowers CSF pH; O2 does not cross easily. Peripheral chemoreceptors respond to both.)
-
Why does the Haldane effect facilitate CO2 transport in venous blood? (Deoxygenated Hb (deoxy-Hb) binds CO2 as carbamino compounds more readily and also buffers H+ better than oxy-Hb - so CO2 loading in tissues is enhanced.)
7. Regulation of Respiration
-
Why does apnea occur after voluntary hyperventilation? (Hyperventilation washes out CO2, lowering PaCO2 below the apneic threshold - the central chemoreceptor stimulus is removed, so breathing stops until CO2 rebuilds.)
-
Why does increased pulmonary ventilation continue even after exercise has stopped? (Lactic acid produced during exercise continues to be metabolized, generating CO2 - elevated CO2 and H+ continue to stimulate chemoreceptors even post-exercise. Also, body temperature remains elevated briefly.)
-
Why do peripheral chemoreceptors (carotid and aortic bodies) respond to PO2, not O2 content? (Chemoreceptor cells detect dissolved O2 tension (PO2), not total O2 content - hence they do not respond to anemia but do respond to hypoxic hypoxia.)
-
Why is ventilation NOT stimulated in anemic hypoxia? (PaO2 is normal in anemia - peripheral chemoreceptors respond to low PO2, not low Hb content. Since PO2 is preserved, there is no chemoreceptor drive to increase ventilation.)
-
Why does a patient with COPD (chronic CO2 retention) depend on hypoxic drive for breathing? (Chronic hypercapnia desensitizes central chemoreceptors (they reset to the higher PCO2 baseline). The only remaining respiratory stimulus is hypoxemia via peripheral chemoreceptors - this is the "hypoxic drive." Giving high-flow O2 removes this drive → respiratory depression.)
-
Why does the Hering-Breuer reflex prevent over-inflation of the lungs? (Stretch receptors in bronchi and bronchioles fire when lungs are over-inflated - signals travel via vagus to inhibit the inspiratory center, terminating inspiration.)
-
Why is breathing periodic (Cheyne-Stokes) in some conditions? (In heart failure or CNS damage, there is increased circulation time and sluggish chemoreceptor response - the system over-shoots, alternately over-ventilating and under-ventilating in a cyclic pattern.)
8. Hypoxia and Related Conditions
-
Why does high altitude cause hyperventilation? (Low barometric pressure → low PAO2 → low PaO2 → peripheral chemoreceptors stimulated → increased ventilation.)
-
Why does hyperventilation at high altitude cause respiratory alkalosis initially? (CO2 is blown off faster than it is produced, lowering PaCO2 and raising blood pH.)
-
Why does acclimatization at high altitude involve increased 2,3-DPG? (Increased 2,3-DPG shifts the O2-Hb curve to the right, enhancing O2 unloading to tissues at low PO2.)
-
Why is pulmonary vasoconstriction seen in hypoxia (opposite to systemic circulation)? (Hypoxic pulmonary vasoconstriction (HPV) diverts blood away from poorly ventilated alveoli to better-ventilated regions - optimizing V/Q matching. Systemic vessels dilate in hypoxia to increase O2 delivery.)
-
Why does drowning cause hypoxia even if water is removed? (Fresh water drowning: hypotonic water absorbed → dilutes surfactant + enters alveoli → diffuse alveolar collapse. Salt water drowning: hypertonic water draws plasma into alveoli → pulmonary edema. Both impair gas exchange.)
-
Why is histotoxic hypoxia not corrected by O2 therapy? (In cyanide/CO poisoning, mitochondrial cytochrome oxidase is blocked - cells cannot use O2 even if PaO2 is normal. The defect is in utilization, not delivery.)
-
Why does asphyxia cause both hypoxia and hypercapnia simultaneously? (Complete cessation of breathing stops both O2 intake and CO2 elimination - both accumulate/deplete simultaneously.)
9. Lung Function Tests (Applied)
-
Why is PEFR (Peak Expiratory Flow Rate) reduced in asthma? (Bronchoconstriction increases airway resistance, reducing the maximum expiratory flow rate at the beginning of forced expiration.)
-
Why is FEV1/FVC ratio decreased in COPD but Total Lung Capacity is increased? (Airway obstruction traps air → increases RV and TLC. The obstruction impedes expiratory flow (reduces FEV1) more than it reduces total volume (FVC), so the ratio falls.)
-
Why does a patient with pulmonary fibrosis show a restrictive pattern on spirometry? (Fibrosis stiffens the lung, reducing all lung volumes (FVC, TLC, RV) proportionally - FEV1/FVC ratio is normal or increased.)
Format in Exams (NMC CBME Pattern)
Per the NMC CBME guidelines, reasoning questions appear as:
- BAQ (Brief Answer Questions, 3 marks each): "Give reason / Explain why..." - 3 BAQs per paper will be reasoning questions
- SAQ (Short Answer Questions, 5 marks): Applied/clinical reasoning integrated
- Viva voce: All of the above applied orally
The most frequently repeated topics in past papers are: Bohr effect, Haldane effect, surfactant, V/Q ratio, apnea after hyperventilation, cyanosis in CO poisoning vs anemia, hypoxic drive in COPD, 2,3-DPG, and FEV1/FVC in obstructive vs restrictive disease.
Sources: IQ City Medical College 10-year question paper compilation | MGMUHS CBME Physiology Curriculum 2023-24 | Costanzo Physiology | Guyton & Hall | Ganong's Review of Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.