Types of graft
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information to provide a thorough answer on types of grafts. Let me compile this.
Types of Graft
Grafts are classified by two major dimensions: (1) the relationship between donor and recipient (immunological classification) and (2) the tissue or composition of the graft itself.
1. By Donor–Recipient Relationship
| Type | Definition | Example |
|---|---|---|
| Autograft | Tissue taken from and returned to the same individual | Skin graft from thigh to burn wound |
| Isograft (Syngeneic graft) | Graft between genetically identical individuals | Identical twins; inbred mouse strains |
| Allograft (Homograft) | Graft between members of the same species but different genetic makeup | Human-to-human kidney transplant |
| Xenograft (Heterograft) | Graft between different species | Pig-to-human heart valve |
Autografts and isografts almost always survive indefinitely if adequately vascularized. Allografts require immunosuppression and HLA matching. Xenografts suffer severe immune rejection within 1 day to 5 weeks without specific therapy. — Guyton and Hall Textbook of Medical Physiology; Roitt's Essential Immunology
Most clinical transplants involve allografts; the most common is blood transfusion. There is growing interest in xenografts (e.g., pig organs) for expanding donor supply.
2. By Tissue/Composition
Skin Grafts
The most common surgical grafts, classified by depth of tissue harvested:
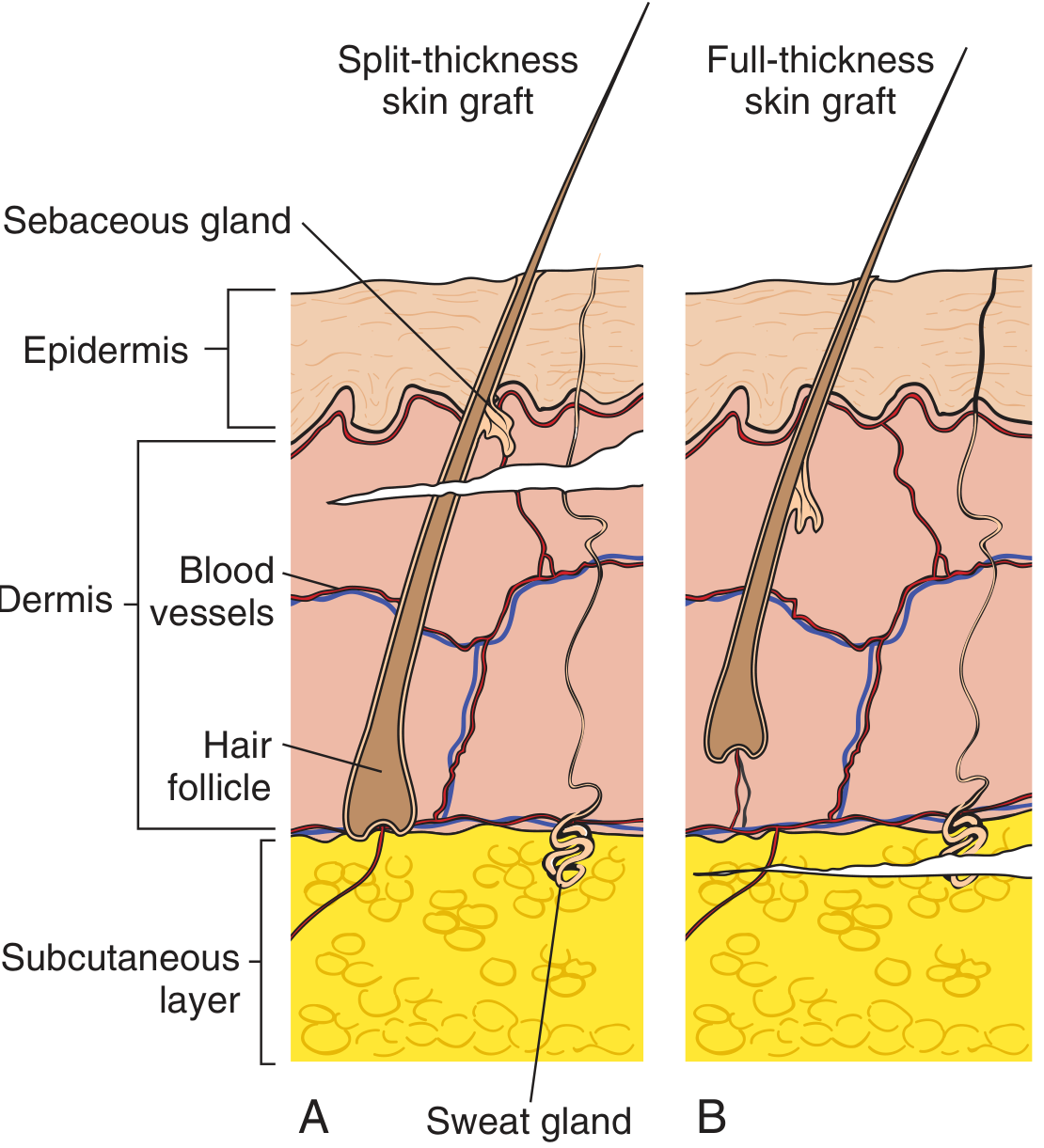
A. Split-Thickness Skin Graft (STSG)
- Contains epidermis + part of dermis
- Can be thin (0.005–0.010 inch), medium, or thick
- Can be meshed to cover large areas (e.g., burns)
- Advantages: donor site regenerates, requires less vascularity, heals faster
- Disadvantages: tends to contract, less cosmetically pleasing
B. Full-Thickness Skin Graft (FTSG)
- Contains epidermis + full dermis
- Harvested by sharp scalpel dissection
- Advantages: resists contracture, better cosmetic match, more durable
- Disadvantages: needs well-vascularized bed, limited donor site; used for smaller defects in cosmetically important areas (face, nose, temple)
— Pfenninger and Fowler's Procedures for Primary Care; Sabiston Textbook of Surgery
Other Major Graft Types by Tissue
| Graft Type | Composition | Clinical Use |
|---|---|---|
| Bone graft | Cancellous, cortical, or vascularized bone | Fracture nonunion, spinal fusion |
| Nerve graft | Peripheral nerve segment | Nerve gap repair |
| Vascular graft | Autologous vein (e.g., saphenous) or synthetic | Bypass surgery (CABG, peripheral arterial) |
| Tendon graft | Autologous tendon (e.g., patellar, hamstring) | ACL reconstruction |
| Corneal graft (keratoplasty) | Donor cornea | Corneal blindness |
| Composite graft | Two or more tissue types (e.g., skin + cartilage) | Ear/nose reconstruction |
| Hematopoietic stem cell graft | Bone marrow or peripheral stem cells | Leukemia, lymphoma |
| Organ grafts | Kidney, liver, heart, lung, pancreas, intestine | End-stage organ failure |
3. Major Transplanted Organs & Tissues (Annual Numbers, US)
| Organ/Tissue | Deceased Donor | Living Donor |
|---|---|---|
| Blood | — | ~14 million units |
| Skin | — | ~48,000 |
| Cornea | 47,000 | — |
| Hematopoietic stem cells | — | 18,000 |
| Kidney | 11,161 | 5,732 |
| Liver | 6,203 | 252 |
| Heart | 2,531 | — |
| Lung | 1,922 | 1 |
| Pancreas | 256 | — |
| Intestine | 108 | 1 |
— Roitt's Essential Immunology
4. Key Immunological Concepts
- HLA (Human Leukocyte Antigen) matching is critical for allograft survival — 6 HLA antigens per person drawn from ~150 variants
- Rejection mechanisms: hyperacute (antibody-mediated, minutes), acute (T-cell mediated, days–weeks), chronic (months–years)
- Immunosuppression is required for all non-syngeneic allografts
- Graft-versus-Host Disease (GvHD): occurs when immunocompetent donor lymphocytes attack the recipient's tissues (especially in hematopoietic stem cell transplants)
This is a shared conversation. Sign in to Orris to start your own chat.