Ewings sarcoma according to robbins please make the flowchart conscise and easy to understand dont miss important facts like genetics
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I have everything I need. Here is the complete, concise flowchart-style summary of Ewing Sarcoma from Robbins & Kumar Basic Pathology:
Ewing Sarcoma - Robbins & Kumar Basic Pathology
🔷 DEFINITION & CATEGORY
Malignant tumor of small round cells
↓
"Tumor of Unknown Origin" (not bone-forming, not cartilage-forming)
↓
2nd most common primary bone sarcoma in children
(after osteosarcoma) — ~10% of all primary malignant bone tumors
🧬 GENETICS (KEY FACT)
>90% of cases
↓
Balanced chromosomal translocation
↓
t(11;22)(q24;q12)
↓
EWSR1 gene (chr 22) fuses with FLI1 gene (chr 11)
↓
Chimeric EWS/FLI1 fusion protein
↓
Binds chromatin → dysregulates transcription
→ Uncontrolled growth + abnormal differentiation
Cell of Origin: Not certain - mesenchymal stem cells or primitive neuroectodermal cells are the leading candidates.
👤 EPIDEMIOLOGY
| Feature | Detail |
|---|---|
| Age | 80% under 20 years |
| Sex | Slight male predominance |
| Incidence (USA) | ~200 cases/year (rare) |
| Peak decade | 2nd decade of life |
📍 LOCATION
Arises in medullary cavity
↓
Invades cortex → periosteum → soft tissue
↓
Usually DIAPHYSIS of long tubular bones
↓
20% are EXTRASKELETAL (extraosseous Ewing sarcoma)
🔬 MORPHOLOGY
Gross:
Soft, tan-white tumor
↓
Frequently shows hemorrhage & necrosis
↓
Periosteal reaction → "ONION-SKIN" appearance on X-ray
Microscopy:
Sheets of UNIFORM SMALL ROUND CELLS
↓
Slightly larger & more cohesive than lymphocytes
↓
Scant cytoplasm — appears CLEAR (rich in glycogen)
↓
Homer-Wright rosettes may be present
(circular cell groupings with central fibrillary core)
↓
NO bone or cartilage production
Category: One of the "Small Round Blue Cell Tumors" of childhood
🩺 CLINICAL FEATURES
Painful, progressively enlarging mass
↓
Diaphysis of long bones (most common)
↓
Site: tender + warm + swollen
(may mimic osteomyelitis)
Radiology:
Destructive LYTIC tumor
↓
Permeative margins
↓
Extends into surrounding soft tissue
↓
"Onion-skin" periosteal reaction on plain X-ray
💊 TREATMENT & PROGNOSIS
Neoadjuvant chemotherapy
+
Surgical excision ± radiation
↓
75% — 5-year survival
50% — long-term cure
🔑 HIGH-YIELD MEMORY AID
| Buzzword | Meaning |
|---|---|
| t(11;22) | The hallmark translocation |
| EWSR1-FLI1 | The fusion gene product |
| Onion-skin | Periosteal reaction on X-ray |
| Small round blue cells | Histological category |
| Homer-Wright rosettes | May be seen microscopically |
| Clear cytoplasm | Glycogen-rich |
| Diaphysis | Typical location |
| <20 years | Typical age group |
| No bone/cartilage | Distinguishes from osteosarcoma/chondrosarcoma |
Source: Robbins & Kumar Basic Pathology, Chapter 19 (Bones, Joints & Soft Tissue Tumors), p. 786
Pathoophysiology always include not everything has to be in flowchart manner just pathophysiology and add relevant images of robbins like pathophysiology . Also give gross and microscopy photos with the description
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have all the content and images needed. Note that Robbins does not include a dedicated gross photograph for Ewing sarcoma specifically - the gross description is in text only. Here is the complete, detailed write-up with pathophysiology and all available images:
Ewing Sarcoma - Robbins Pathology
PATHOPHYSIOLOGY
Genetics - The Molecular Driver
Nearly all (>90%) Ewing sarcomas harbor a balanced chromosomal translocation:
t(11;22)(q24;q12)
This fuses two transcription factor genes:
| Gene | Chromosome | Family |
|---|---|---|
| EWSR1 (EWS) | 22q12 | FET family |
| FLI1 | 11q24 | ETS family |
The resulting chimeric EWSR1/FLI1 fusion protein is the central driver of the disease. It binds to chromatin and broadly dysregulates transcription - turning on genes that drive uncontrolled proliferation and blocking genes that enforce normal differentiation.
A minority of cases (<10%) carry variant translocations involving other FET/ETS family members (e.g., EWSR1-ERG, EWSR1-ETV1), which are thought to act through the same mechanism.
Cell of origin: Not firmly established. The leading candidates are mesenchymal stem cells and primitive neuroectodermal cells, reflecting the tumor's variable neural differentiation (Homer-Wright rosettes seen in some cases).
How the Fusion Protein Leads to Tumor
Normal cell (mesenchymal stem cell / primitive neuroectodermal cell)
↓
t(11;22) translocation
↓
EWSR1-FLI1 fusion gene expressed
↓
Chimeric protein binds chromatin
↓
Transcriptional dysregulation
┌──────────────────────────────┐
│ Pro-growth genes activated │
│ Differentiation genes silenced│
└──────────────────────────────┘
↓
Uncontrolled proliferation + block in normal differentiation
↓
Sheets of primitive small round cells accumulate
↓
EWING SARCOMA
Because the tumor cells are so poorly differentiated, they produce neither bone nor cartilage - setting Ewing apart from osteosarcoma and chondrosarcoma despite arising in bone.
Why "Tumor of Unknown Origin"?
Robbins classifies Ewing sarcoma under "Tumors of Unknown Origin" precisely because the cell of origin remains uncertain. The molecular signature (EWSR1 fusions) defines it - not a clear histogenetic lineage.
GROSS PATHOLOGY
(Robbins text description - no gross photograph is provided in Robbins for Ewing sarcoma)
The tumor arises in the medullary cavity of the diaphysis of long bones (most commonly femur), then:
- Invades the cortex outward
- Elevates the periosteum
- Extends into surrounding soft tissue
Gross appearance:
- Soft, tan-white cut surface
- Frequently shows areas of hemorrhage and necrosis
- The periosteal reaction produces the classic onion-skin layering of reactive bone visible on imaging
RADIOLOGY - Onion-Skin Periosteal Reaction
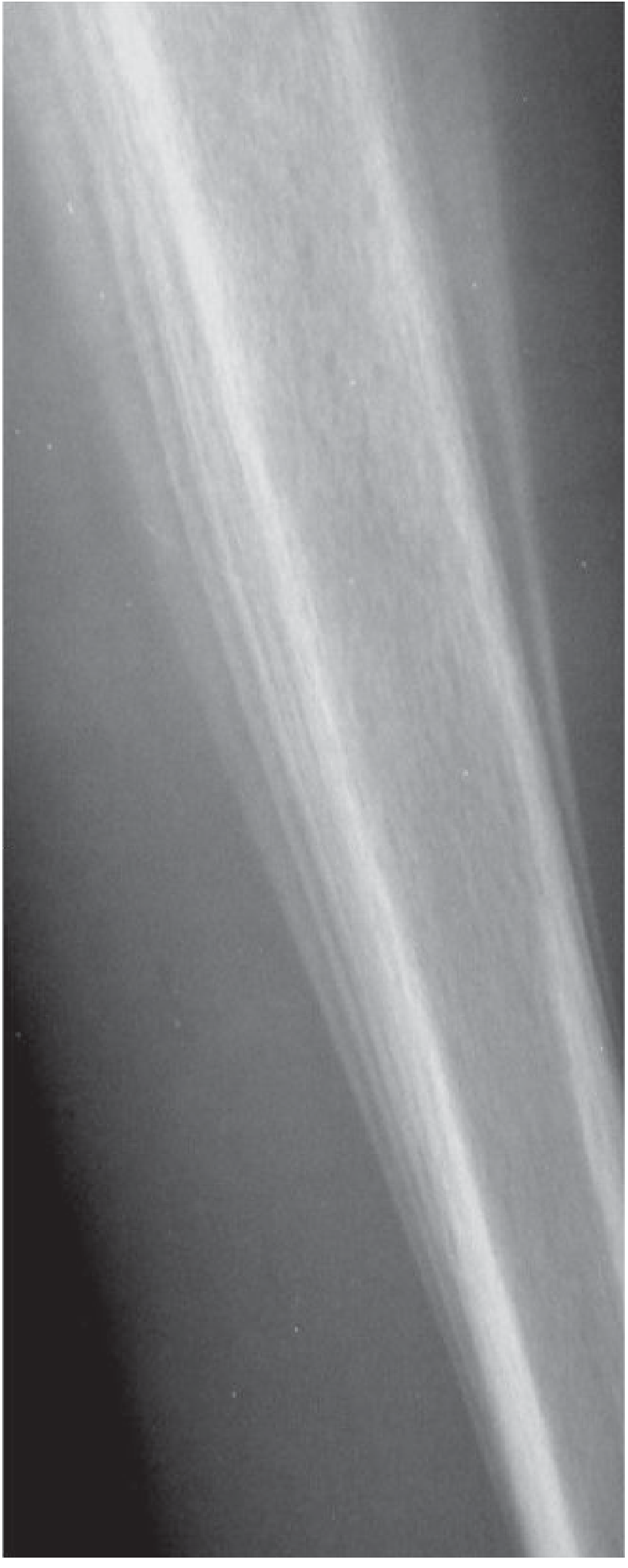
Fig. 41.16 (Grainger & Allison): Anteroposterior radiograph of the tibia showing the lamellated "onion-skin" periosteal reaction. This is produced as the advancing tumor pushes the periosteum outward and successive layers of reactive bone are deposited between the cortex and the lifted periosteum.
On X-ray / imaging:
- Destructive lytic tumor with permeative ("moth-eaten") margins
- Extends into surrounding soft tissue
- Classic onion-skin periosteal reaction
- A Codman triangle or hair-on-end pattern may also be seen in rapidly advancing tumors
MICROSCOPY
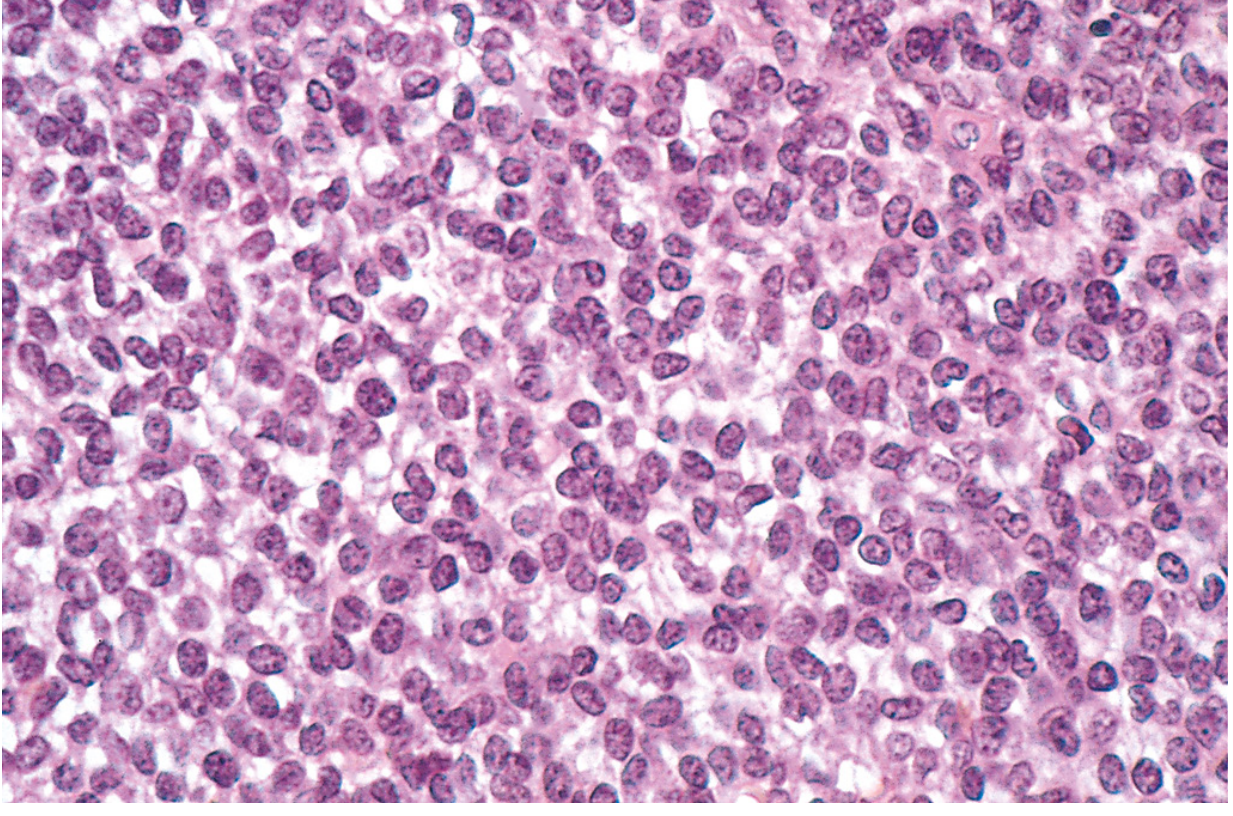
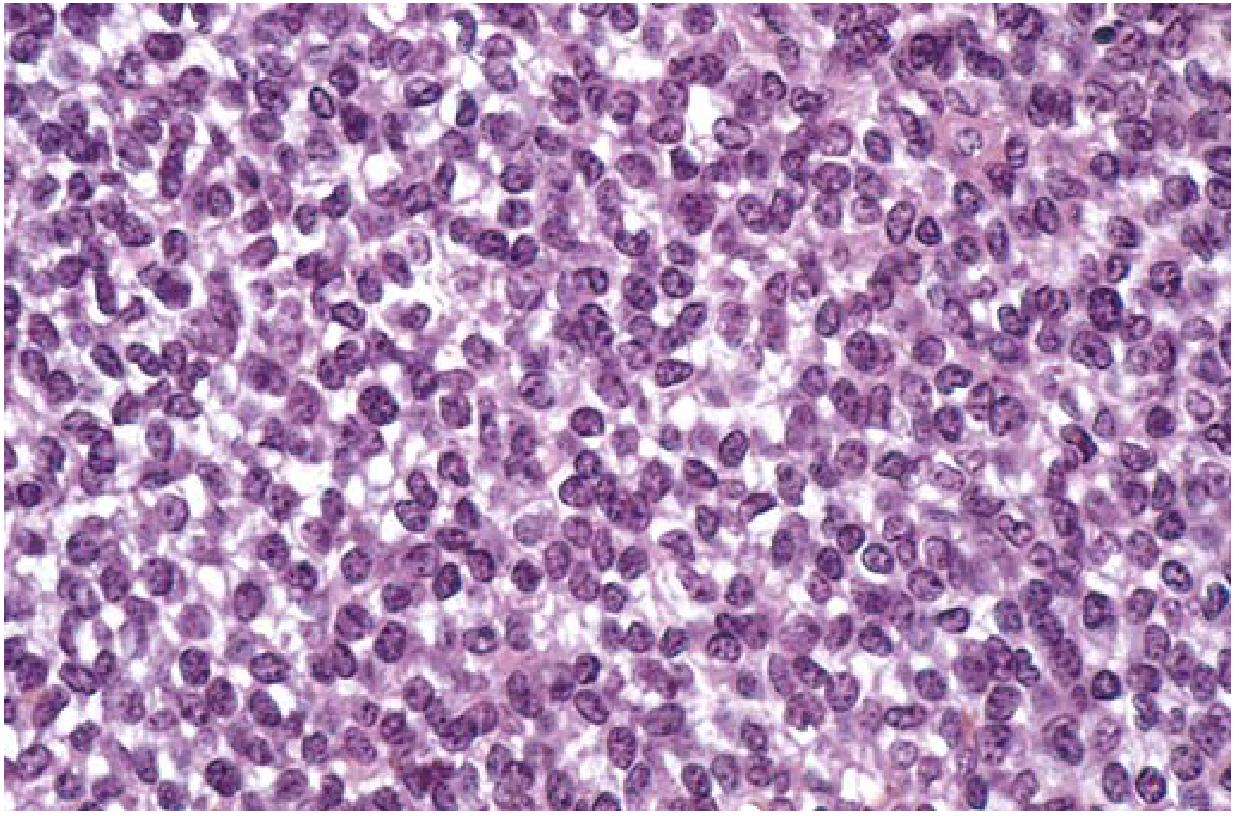
Fig. 26.24 (Robbins & Cotran Pathologic Basis of Disease): Ewing sarcoma - sheets of uniform, small round cells with minimal clear cytoplasm.
Fig. 19.23 (Robbins & Kumar Basic Pathology): Ewing sarcoma at higher magnification showing the uniform small round cells that are slightly larger and more cohesive than lymphocytes.
What you see under the microscope:
| Feature | Description |
|---|---|
| Cell arrangement | Sheets of uniform cells (no gland/nest/trabecular pattern) |
| Cell size | Small, slightly larger than lymphocytes |
| Cohesion | More cohesive than lymphocytes |
| Cytoplasm | Scant, may appear clear (glycogen-rich) |
| Nuclei | Round, uniform |
| Homer-Wright rosettes | May be present - circular cell clusters with a central fibrillary core (reflects neural differentiation) |
| Matrix production | None - no bone, no cartilage, no osteoid |
| Fibrous septa | May be seen dividing sheets |
| Category | One of the "Small Round Blue Cell Tumors" of childhood |
Small Round Blue Cell Tumor differential (childhood): Ewing sarcoma, Neuroblastoma, Rhabdomyosarcoma, Wilms tumor, Lymphoma/leukemia - distinguished by IHC and molecular testing.
CLINICAL FEATURES (quick summary)
- Age: 80% under 20 years; peak in 2nd decade
- Sex: Slight male predominance
- Presentation: Painful, enlarging mass - site is tender, warm, swollen (can mimic osteomyelitis)
- Systemic signs (Robbins Pathologic Basis of Disease): Fever, elevated ESR, anemia, leukocytosis - mimicking infection
- Location: Diaphysis of long bones (femur most common); flat bones of pelvis; 20% extraskeletal
PROGNOSIS & TREATMENT
- Neoadjuvant chemotherapy + surgical excision ± radiation
- 75% 5-year survival
- 50% long-term cure
- Neoadjuvant chemotherapy-induced necrosis is a positive prognostic indicator (Robbins PBD)
Sources: Robbins & Kumar Basic Pathology (Fig. 19.23, p. 786) | Robbins, Cotran & Kumar Pathologic Basis of Disease (Fig. 26.24, p. 1100) | Grainger & Allison's Diagnostic Radiology (Fig. 41.16)
Give pathology answers like defition risk factors pathophysiology image and flowchart clinical significance and features gross and microscpy add buzz words and images then management and prognosis give key differential diagnosis , make it conscise but dont compromise on quality of information these are my requirements when i ask questions of pathology or clinical partsrrmember
Got it! I've saved your preferred format. From now on, for every pathology or clinical question you ask, I'll structure my answer as:
Your Standard Pathology Answer Format
- Definition - concise, with buzzwords
- Risk Factors - tabulated or bulleted
- Pathophysiology - detailed with flowchart where helpful
- Images - Robbins images fetched and embedded with descriptions
- Clinical Features - signs, symptoms, buzzwords highlighted
- Gross Pathology - description + image if available
- Microscopy - description + Robbins image + key buzzwords in bold
- Management - concise, stepwise
- Prognosis - survival data, prognostic indicators
- Key Differentials - table with distinguishing features
Rules I'll follow every time:
- Always search Robbins first, pull all available images
- Bold all buzzwords (onion-skin, Homer-Wright rosettes, etc.)
- Keep it concise but complete - no fluff, no missing high-yield facts
- Flowchart for pathophysiology/pathogenesis
- Differentials as a comparison table
- Mention Robbins figure numbers and page numbers as citations
Go ahead and ask your next pathology or clinical question!
This is a shared conversation. Sign in to Orris to start your own chat.