Parathyroid scan
Reading File
Finding Sources
Finding Sources
Searching the Web
parathyroid scan sestamibi scintigraphy nuclear medicine technique interpretation
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Parathyroid Scan (Sestamibi Scintigraphy)
Overview
A parathyroid scan is a nuclear medicine imaging technique used to localize hyperfunctioning parathyroid tissue - primarily in primary hyperparathyroidism (PHPT) before surgery. The principal agent is technetium-99m sestamibi (99mTc-MIBI), originally developed for cardiac imaging and serendipitously found to accumulate in parathyroid adenomas.
Radiopharmaceutical & Mechanism
- Agent: 99mTc-sestamibi (a lipophilic cationic compound)
- Uptake: Diffuses passively across cell membranes and accumulates in mitochondria
- Both thyroid and parathyroid tissue take up sestamibi, but parathyroid adenomas (rich in oxyphil cells with high mitochondrial content) retain the tracer significantly longer
- Normal parathyroid glands are too small to be visualized on any form of scintigraphy
- Comparison of early images (10 min) and delayed images (2 hours) after injection reveals the parathyroid focus as persisting activity after thyroid washout
Imaging Modalities (Progression)
1. Planar Sestamibi Scintigraphy
- Traditional two-dimensional anterior-posterior (and sometimes lateral) views
- Provides limited anatomical detail
- Sensitivity: ~71-79% for single adenomas
- Negative result in 12-25% of patients
2. SPECT (Single Photon Emission Computed Tomography)
- 3-dimensional rotating images with higher resolution
- Better detection of deep cervical and ectopic glands
- Sensitivity: 87-91% for single adenomas; overall 92-98%
- Limited sensitivity for multigland disease (MGD)
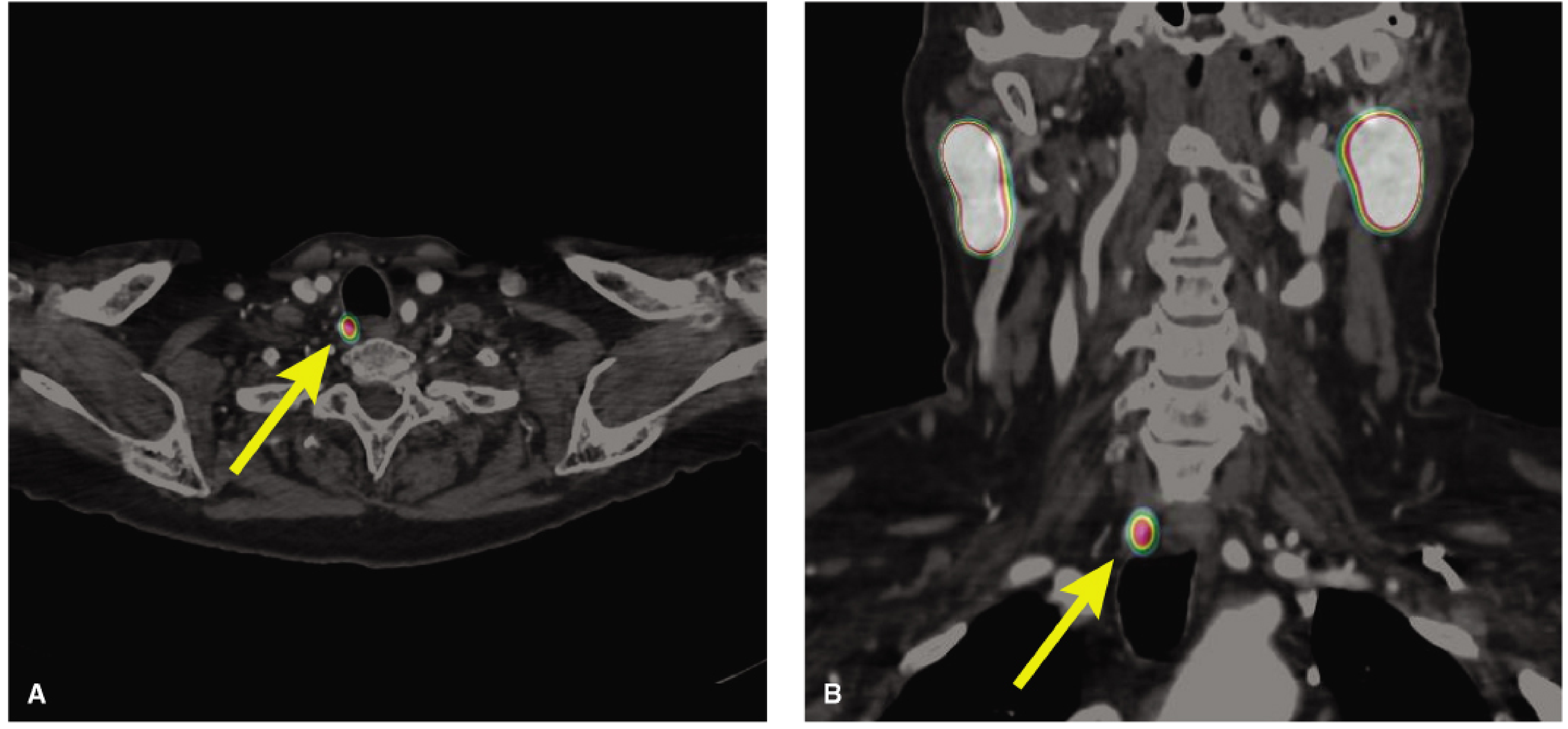
3. Sestamibi SPECT/CT (Current Gold Standard)
- Fuses SPECT functional data with CT anatomical data
- Sensitivity: up to 96% for single adenomas
- Up to 60% more accurate than SPECT alone for MGD
- Delivers significantly less radiation than 4D-CT when using attenuated CT windows
Below: Sestamibi SPECT/CT showing an enlarged, hyperdescended right superior parathyroid gland (yellow arrow) - transverse view (A) and coronal view (B):
4. Subtraction (Dual Isotope) Scintigraphy
- Useful when thyroid pathology (nodular goitre) complicates interpretation
- Patient receives sestamibi (thyroid + parathyroid uptake) AND a thyroid-specific tracer (¹²³I or 99mTc-pertechnetate)
- Computer software subtracts the thyroid image, revealing parathyroid tissue
- Limitation: motion artefact can degrade image quality
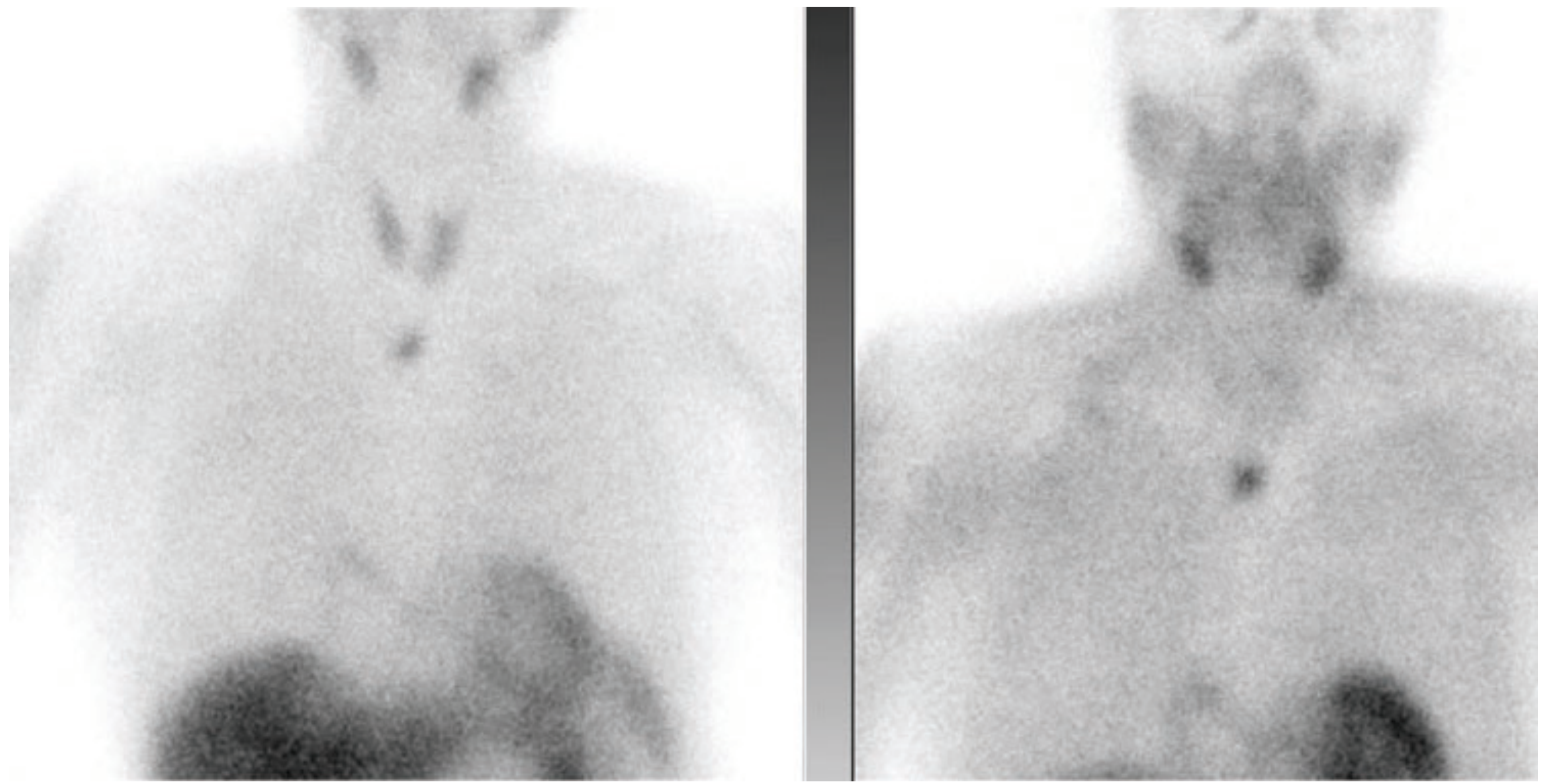
Classic Scan Finding
Below: Dual-phase planar sestamibi scan showing an ectopic parathyroid gland in the mediastinum - the left panel (early phase) shows both thyroid and parathyroid uptake; the right panel (delayed phase) shows persistent focal activity in the mediastinum after thyroid washout:
Predictive Factors for Scan Result
| Positive Scan | Negative Scan |
|---|---|
| High oxyphil cell content (>20%) | Thyroid nodules present |
| Vitamin D deficiency | Multigland disease |
| High PTH levels | Adenoma weight <600 mg |
| High calcium levels | Calcium channel blocker use |
(Scott-Brown's Otorhinolaryngology, Vol. 1, p. 882)
Causes of False Negative / Limitations
- Multigland disease (MGD): Major shortcoming - in one study, none of 15 patients with MGD were identified preoperatively
- Small gland size (<600 mg)
- Coexisting thyroid disease (nodules, goitre)
- Superior gland location (tends to be smaller)
- Calcium channel blockers: Interfere with sestamibi uptake by parathyroid cells
- Low oxyphil cell content
Indications
- Preoperative localization in primary hyperparathyroidism before first-time surgery
- Preoperative planning for minimally invasive parathyroidectomy (MIP) - requires concordant imaging
- Ectopic gland localization (mediastinal, intrathyroidal, retroesophageal) - sestamibi is superior to ultrasound for mediastinal glands
- Reoperative parathyroid surgery (with fine-cut CT windows)
- Localizing autotransplanted glands in the forearm
Intraoperative Use (Radioguided Surgery)
99mTc-sestamibi can be injected preoperatively and a handheld gamma probe used intraoperatively to confirm excision of the hyperfunctioning gland. However, most experts consider this superseded by intraoperative PTH (ioPTH) monitoring, as it carries the same limitations as preoperative scintigraphy (particularly poor MGD detection). - Fischer's Mastery of Surgery, 8th ed., p. 1129
Comparison with Other Localizing Studies
| Study | Sensitivity (Single Adenoma) | Key Advantage |
|---|---|---|
| Ultrasound | ~76% | No radiation, inexpensive, real-time |
| Planar sestamibi | 71-79% | Whole-body survey |
| SPECT | 87-98% | 3D, ectopic detection |
| SPECT/CT | up to 96% | Best anatomic correlation |
| 4D-CT | ~73% (by quadrant) | Useful when scintigraphy negative/discordant |
4D-CT is reserved for discordant or negative conventional studies and reoperative cases, but carries up to 50-fold higher thyroid radiation dose than scintigraphy.
Sources:
- Fischer's Mastery of Surgery, 8th ed., pp. 1128-1130
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1, pp. 882-884
- Goldman-Cecil Medicine, p. (block 39 - Hyperparathyroidism diagnosis)
Aal indications for parathyroid scan
Finding Sources
Finding Sources
Searching the Web
parathyroid sestamibi scan all indications guidelines 2024
Finding Sources
Finding Sources
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC8263421
Reading File
Finding Sources
Reading File
Finding Sources
I now have enough comprehensive material from textbooks and the EANM guidelines. Here is the complete answer:
All Indications for Parathyroid Scan (Sestamibi Scintigraphy)
1. Primary Hyperparathyroidism (pHPT) - Preoperative Localization
This is the principal and most common indication.
- Before minimally invasive parathyroidectomy (MIP): Sestamibi scintigraphy (ideally SPECT/CT) is required to confirm single-gland disease and localize the adenoma to guide a focused, limited unilateral approach. MIP is considered when at least one preoperative study identifies a single suspicious gland.
- Before bilateral cervical exploration (BCE): Even when BCE is planned, preoperative imaging helps the surgeon anticipate gland position and reduces operative time.
- Important caveat: Imaging has no role in diagnosing pHPT or deciding whether to operate - it is purely to assist surgical planning in a patient already committed to surgery. (Fischer's Mastery of Surgery, 8th ed., p. 1163)
2. Ectopic Parathyroid Gland Localization
- Mediastinal adenomas (present in ~15% of persistent/recurrent cases) are frequently missed by ultrasound but detected on sestamibi scan, which surveys the whole body including the chest
- Retroesophageal / paratracheal / intrathyroidal locations
- Ectopic glands within the thyrothymic ligament or within the thymus
- Scan field of view should extend from the neck to the base of the heart to capture all possible ectopic sites
3. Persistent or Recurrent Hyperparathyroidism (Reoperative Surgery)
- After failed first parathyroid exploration, sestamibi scintigraphy is a first-line re-localization study alongside neck ultrasound
- In re-exploration, combined imaging (SPECT/CT + ultrasound ± 4D-CT ± MRI) is often required
- Fine-cut CT windows on SPECT/CT can be specifically used to assess candidacy for reoperation
- Invasive studies (selective arteriography, venous sampling) are only used if non-invasive localization has failed (Pye's Surgical Handicraft, p. 342)
4. Secondary Hyperparathyroidism (sHPT) - Selected Cases
- Routine preoperative scintigraphy is not standard for sHPT (bilateral open exploration is usually performed for renal HPT)
- However, sestamibi scan is indicated in sHPT when:
- Planning revision surgery after failed prior parathyroidectomy for sHPT
- Detecting ectopic or supernumerary glands (which influence the surgical plan)
- Identifying the gland with the lowest MIBI uptake that may be partially autografted or preserved
- Combination of cervical ultrasound + dual-tracer scintigraphy is recommended for localization in renal HPT undergoing surgery (EANM Practice Guidelines 2021)
5. Tertiary Hyperparathyroidism
- After renal transplantation, persistent autonomous hyperparathyroidism may require parathyroidectomy
- Sestamibi scan is used preoperatively for localization, particularly in re-exploration scenarios
6. Parathyroid Carcinoma - Preoperative Mapping
- When parathyroid carcinoma is suspected (very high PTH, palpable neck mass), scintigraphy helps map the primary lesion and identify potential metastatic or recurrent disease, though sensitivity is limited
7. Intraoperative Radioguided Parathyroidectomy
- 99mTc-sestamibi is injected preoperatively and a handheld gamma probe is used intraoperatively to confirm complete resection of the hyperfunctioning gland
- Particularly used when standard localization is uncertain or in reoperative cases
- Most centers now prefer this as an adjunct to intraoperative PTH (ioPTH) monitoring rather than as the primary guidance tool (Current Surgical Therapy 14e)
8. Autotransplanted Parathyroid Tissue - Function Assessment
- After total parathyroidectomy with forearm autotransplantation (for sHPT), sestamibi can localize functioning transplanted tissue in the forearm if hypercalcaemia recurs
- Confirms the autograft is hyperfunctioning and guides surgical re-excision
9. When Concordant Localization Is Needed for MIP Decision
- Patients with negative or discordant results on ultrasound: sestamibi scan is used as the second-line imaging modality
- Patients in whom a single-gland focus is identified concordantly on both ultrasound and sestamibi are the best candidates for MIP without bilateral exploration
Conditions Where Parathyroid Scan Is NOT Indicated
| Situation | Reason |
|---|---|
| Diagnosing hyperparathyroidism | Diagnosis is biochemical (PTH + calcium) - imaging does not diagnose PHPT |
| Routine asymptomatic PHPT managed conservatively | No surgical plan = no need to localize |
| Routine primary sHPT (renal HPT) without reoperation | Bilateral open exploration is standard; scan adds little |
| MEN1 patients (4-gland hyperplasia confirmed) | Will need BCE regardless; scan unlikely to change management |
Sources:
- Fischer's Mastery of Surgery, 8th ed., pp. 1163-1164
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1, pp. 882-884
- Pye's Surgical Handicraft, 22nd ed., p. 342
- EANM Practice Guidelines for Parathyroid Imaging (2021) - European Association of Nuclear Medicine
Protocol for parathyroid imaging
Finding Sources
Finding Sources
Searching the Web
parathyroid sestamibi SPECT CT protocol imaging technique 2023 2024 guidelines
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC8263421
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading Web Page
https://eanm.org/wp-content/uploads/2024/06/EANM_2005_tech_g…
Excellent - rich protocol data from EANM, SNMMI and textbooks. Now compiling the comprehensive answer:
Protocol for Parathyroid Imaging
Step 1 - Patient Preparation
Clinical Checks (Before Booking)
- Confirm biochemical diagnosis of hyperparathyroidism (elevated PTH + hypercalcaemia) - imaging is only for localization, not diagnosis
- Review previous neck surgery notes and pathology reports
- Check for pregnancy / breastfeeding (absolute contraindications to radionuclide imaging)
- Check renal function if 4D-CT is being considered (contrast agent)
Drug Withholding
| Drug/Class | Action |
|---|---|
| Calcium channel blockers | Withhold if possible - reduce sestamibi uptake by parathyroid cells and decrease sensitivity |
| Thyroid medication (levothyroxine, antithyroids) | Withhold 4-6 weeks before imaging if using dual-tracer/subtraction technique (under referring clinician guidance) |
| Iodine-containing drugs (amiodarone, Lugol's solution, iodinated contrast, propylthiouracil, corticosteroids, antihistamines) | May need withdrawal before dual-tracer study; seek clinician advice |
| Lithium | Note: associated with multigland disease; affects scan interpretation |
- Exception: If the patient is on thyroid hormone replacement, do NOT withdraw - instead switch to dual-phase sestamibi (rather than dual-tracer) to avoid hypothyroidism
- If total thyroidectomy has been performed: subtraction technique is not applicable - use dual-phase sestamibi only
Patient Positioning
- Patient supine with a sandbag placed under the shoulders to extend the neck - exactly as positioned on the operating table - under the gamma camera
- Neck hyperextension improves separation of thyroid from parathyroid tissue on images
- Patient must remain completely still especially during dual-tracer studies (motion artefact is the main source of error)
- Claustrophobic patients or those unable to remain still may require sedation
Step 2 - Radiopharmaceuticals
| Agent | Route | Dose (Adults) | Energy | Half-Life | Effective Dose |
|---|---|---|---|---|---|
| 99mTc-sestamibi (MIBI) | IV | 400-900 MBq (EANM) / 740-1110 MBq (SNMMI) | 140 keV | 6.04 h | 0.007 mSv/MBq |
| 99mTc-tetrofosmin | IV | 400-900 MBq | 140 keV | 6.04 h | 0.0063 mSv/MBq |
| 99mTc-pertechnetate | IV | 74-150 MBq | 140 keV | 6.04 h | 0.016 mSv/MBq |
| ¹²³I-iodide | Oral | 7.5-20 MBq | 159 keV | 13.2 h | 0.22 mSv/MBq |
- Dose adjusted based on patient body mass and whether SPECT is planned
- 99mTc-tetrofosmin dual-phase is NOT recommended - it washes out too rapidly from parathyroid tissue to give reliable delayed images
Step 3 - Imaging Protocols
Protocol A: Dual-Phase 99mTc-Sestamibi (Standard / Most Widely Used)
Mechanism: Sestamibi washes out from normal thyroid faster than from hyperfunctioning parathyroid (which has mitochondria-rich oxyphil cells) - comparison of early vs delayed images reveals the retained focus.
Acquisition:
- IV injection of 99mTc-sestamibi (400-900 MBq)
- Early images: 10-15 min post-injection
- Delayed images: 90-150 min post-injection (some centres use 2-3 hours)
- Both phases: large field of view from skull base to base of heart (to capture ectopic mediastinal glands)
- Views: anterior + right and left anterolateral planar images
Camera settings:
- Large field-of-view gamma camera
- Low-Energy High-Resolution (LEHR) collimators
- Energy window: 140 ± 10 keV
- Matrix size: 128×128 (minimum) or 256×256 (preferred)
When to use: First-line standard protocol; preferred for patients on thyroid hormone replacement
Protocol B: Dual-Phase Sestamibi + SPECT/CT (Current Best Practice)
This is the recommended standard per EANM 2021 guidelines - SPECT/CT with sestamibi is superior to planar or stand-alone SPECT.
Additional to Protocol A:
- After early or delayed planar images, perform SPECT/CT acquisition
- SPECT covers neck + upper mediastinum (skull base to heart base)
- CT: use lowest CT dose compatible with the purpose (attenuation correction CT at ~30 mA is sufficient for most cases; fine-cut diagnostic CT at ~120 mA for reoperative cases)
- Fusion of SPECT functional data with CT anatomical data on workstation
- Sensitivity: up to 96% for single adenomas; 88% patient-based pooled detection rate (EANM meta-analysis, 23 papers, 1236 patients)
- SPECT alone (without CT): sensitivity 92-98%
Protocol C: Dual-Tracer Subtraction Scintigraphy
When to use: When thyroid nodules or goitre are present (reduces thyroid background interference); when dual-phase technique gives ambiguous results.
Two sub-options:
C1: 99mTc-sestamibi / 99mTc-pertechnetate subtraction
- Option 1 (pertechnetate first):
- Inject 99mTc-pertechnetate → wait 30 min → acquire 10-min thyroid image
- Inject 99mTc-sestamibi → acquire 10-min image 10 min later
- Computer-subtract pertechnetate (thyroid) from sestamibi (thyroid + parathyroid)
- Option 2 (sestamibi first):
- Acquire early sestamibi image
- Inject pertechnetate → immobilize patient 15-30 min → acquire 10-min image
- Computer-subtract
C2: 99mTc-sestamibi / ¹²³I-iodide subtraction
- ¹²³I given orally (uptake imaging at 4-6 hours or next day)
- Then sestamibi injected IV; early image at 10-15 min
- Digital subtraction of ¹²³I thyroid image from sestamibi image
- Recommend 2-3 day waiting period between tracers to reduce administered activity/radiation
- Without iodine saturation for the thyroid scan
Key limitation: Motion artefact between the two acquisition sessions degrades image quality - patient must be completely immobilized. A neck brace or head holder helps.
Protocol D: PET/CT with ¹⁸F-Choline or ¹¹C-Methionine (Emerging)
Indications: Failed/inconclusive conventional scintigraphy; reoperative cases; small glands below SPECT/CT detection threshold.
¹⁸F-Fluorocholine (FCH) PET/CT:
- Higher spatial resolution than SPECT
- Shorter imaging time (~1 hour total)
- Avoid vigorous exercise before scan (increases muscle uptake)
- No standardized dose/protocol yet per EANM 2021
- Increasingly used in Europe as second-line or even first-line at specialist centres
¹¹C-Methionine PET/CT:
- Requires on-site cyclotron (limits availability)
- Useful in negative/equivocal sestamibi cases
Step 4 - Image Interpretation
Dual-Phase Sestamibi
- Positive: Focal area of retained activity at delayed phase that was present on early phase - site of hyperfunctioning parathyroid
- True positive pattern: Focus persists or becomes relatively more prominent at 2 hours compared to surrounding thyroid
- False negative: Small gland (<600 mg), rapid washout, thyroid nodule obscuring the focus, calcium channel blockers
SPECT/CT Interpretation
- Report should specify:
- Which images showed the lesion (early, delayed, or both)
- Location: Mediastinum vs thyroid bed (upper/lower pole, ectopic); laterality (right/left)
- Depth and relationship to surrounding structures (enabled by CT)
- Any confounding factors (patient motion, thyroid nodules, prior thyroidectomy)
- Whether SPECT or SPECT/CT was used
- CT parameters used (kVp, mA, pitch, beam width, scan length)
Subtraction Scans
- Residual activity after thyroid subtraction = parathyroid focus
- Limitation: Motion artefact can create false positives or obscure true positives
Step 5 - Radiation Dosimetry Summary
| Radiopharmaceutical | Highest dose organ | Organ dose (mGy) | Effective dose (mSv) |
|---|---|---|---|
| 99mTc-sestamibi (900 MBq) | Gallbladder | ~35 | ~6.3 |
| 99mTc-pertechnetate (150 MBq) | Upper large intestine | ~8.6 | ~2.0 |
| ¹²³I-iodide (20 MBq, 35% uptake) | Thyroid | ~90 | ~4.4 |
Sestamibi SPECT/CT delivers significantly less radiation to the thyroid than 4D-CT (which exposes the thyroid to up to 50× the dose of scintigraphy).
Step 6 - Reporting Checklist
A complete parathyroid scan report should include:
- Patient demographics and clinical indication
- Radiopharmaceutical(s) used, dose, route, and order of administration
- Timing of image acquisition after injection
- Imaging type: planar / SPECT / SPECT-CT
- Projections acquired and region imaged (neck, mediastinum)
- CT parameters (kVp, mA, pitch, beam width, scan length) if CT used
- Presence/absence and location of focal retained activity
- Laterality and depth in relation to thyroid/anatomical landmarks
- Study limitations (motion, thyroid disease, prior surgery)
- Correlation with ultrasound findings if available
Quick Protocol Decision Tree
Primary hyperparathyroidism confirmed biochemically
|
Is thyroid gland intact?
| |
YES NO (total thyroidectomy)
| |
Is thyroid disease present? Dual-phase sestamibi only
| |
YES NO
| |
Dual-tracer Dual-phase sestamibi
subtraction + SPECT/CT (standard)
+ SPECT/CT
|
All negative or discordant?
|
4D-CT or ¹⁸F-Choline PET/CT
Sources:
- EANM Practice Guidelines for Parathyroid Imaging (2021)
- SNMMI Practice Guideline for Parathyroid Scintigraphy 4.0
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 1, pp. 882-884
- Fischer's Mastery of Surgery, 8th ed., pp. 1128-1130
This is a shared conversation. Sign in to Orris to start your own chat.