Alcohol
Asking for Preferences
Reading File
Finding Sources
Searching PubMed
"alcohol" AND "health effects"
Searching the Web
alcohol health effects risks 2025 WHO evidence
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to write a thorough answer. Let me compile it all.
Health Effects & Risks of Alcohol (Ethanol)
What It Is
Ethyl alcohol (ethanol) is the psychoactive ingredient in fermented and distilled beverages. Common alcohol content by volume: beer 2-10%, wine 8-15.5%, spirits (whisky, gin, rum) ~40-43%. One "standard drink" = a 12 oz beer, a 4 oz glass of wine, or a 1.25 oz shot of 80-proof liquor.
- Katzung's Basic and Clinical Pharmacology, 16th Edition, p. 625
- Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology, p. 653
How the Body Processes It
- Rapidly absorbed from the GI tract; peak blood levels reached in 45-90 minutes
- Absorption is slowed by food (especially fats and proteins), and faster on an empty stomach
- ~90% is oxidised in the liver; the remaining 10% is excreted by the kidneys and lungs
- Elimination follows zero-order kinetics (a fixed amount per hour, ~15-18 mg/100 mL blood/hour, regardless of dose)
- The main pathway: ethanol → acetaldehyde (via alcohol dehydrogenase) → acetate. Acetaldehyde is itself toxic and responsible for much of the organ damage.
- Parikh's Textbook, p. 653; Washington Manual of Medical Therapeutics
Acute Effects (Intoxication)
Acute intoxication produces mental status changes, slurred speech, motor impairment, and cerebellar dysfunction. Severe overdose (especially with other CNS depressants) can impair airway protective reflexes and respiration.
Ethanol acts by:
- Enhancing inhibitory GABA-A receptor signalling
- Suppressing excitatory NMDA glutamate receptor signalling
This combination produces CNS depression - sedation, disinhibition, coordination failure, and at high doses, coma.
- Washington Manual of Medical Therapeutics
Alcohol Withdrawal
When a chronic heavy drinker abruptly stops, rebound CNS excitation causes a withdrawal syndrome. The timeline is shown below:
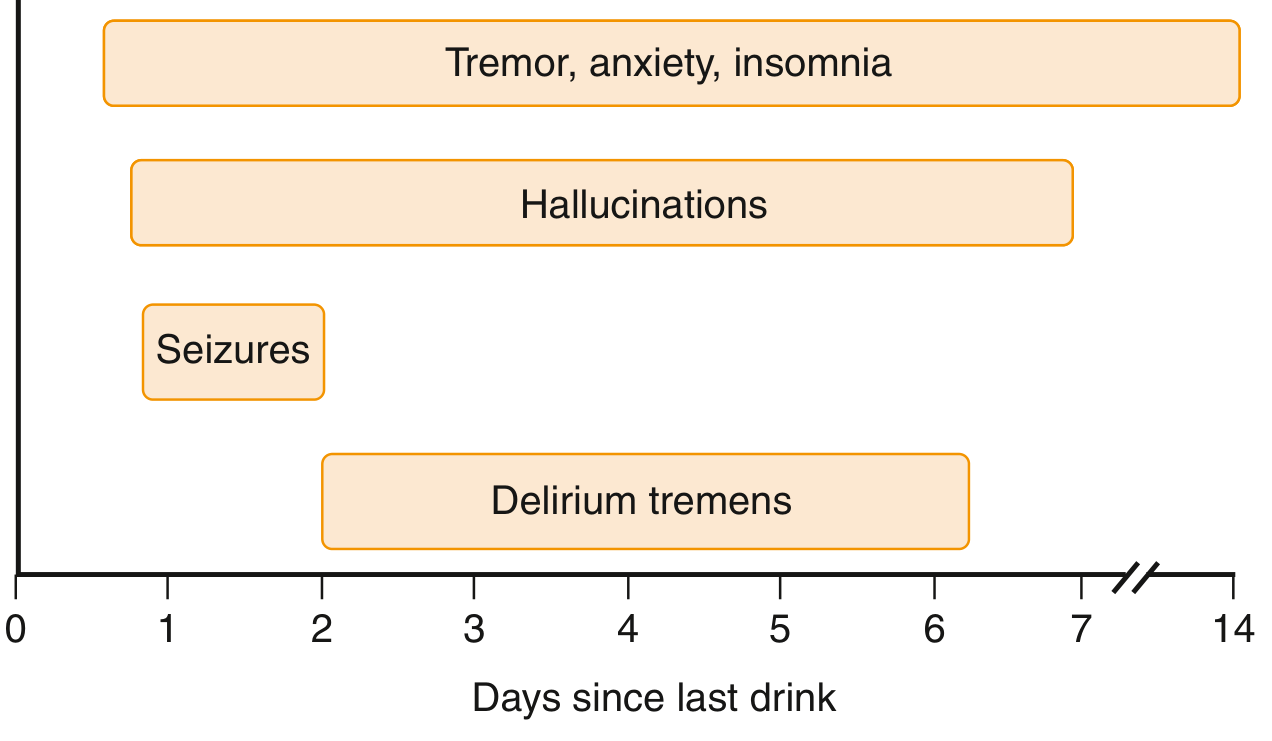
Delirium tremens is the most severe manifestation: disorientation, confusion, hallucinations, diaphoresis, fever, and tachycardia. It typically begins 2-4 days after the last drink and can be fatal.
- Goldman-Cecil Medicine, p. 3779
Chronic Health Effects
Chronic heavy drinking affects virtually every major organ system:
1. Liver (Most Common)
Liver disease is the most common medical complication. An estimated 15-30% of chronic heavy drinkers eventually develop severe liver disease. The progression is:
Fatty liver (reversible) → Alcoholic hepatitis → Cirrhosis → Liver failure
Alcohol is the leading cause of cirrhosis and liver transplantation in the US. Women are more susceptible than men. Concurrent hepatitis B or C infection dramatically increases the risk. Cirrhosis leads to portal hypertension and esophageal varices, which can rupture causing life-threatening bleeding.
- Katzung's Basic and Clinical Pharmacology, p. 625
2. Nervous System
- Cognitive impairment: ranges from mild memory problems to severe dementia resembling Alzheimer's disease
- Wernicke encephalopathy: confusion, ataxia, oculomotor abnormalities - caused by thiamine (B1) deficiency
- Korsakoff syndrome: amnesia and confabulation, also due to thiamine deficiency
- Peripheral neuropathy: paresthesias, numbness, weakness, chronic pain
- Cerebellar degeneration (in a small proportion): presents as unsteady gait
- Goldman-Cecil Medicine; Katzung's Basic and Clinical Pharmacology
3. Cardiovascular System
- Alcoholic cardiomyopathy - dilated cardiomyopathy presenting as heart failure
- Hypertension
- Atrial fibrillation ("holiday heart" syndrome)
- Increases risk of chronic heart failure and myocardial infarction
Note on moderate drinking: There is epidemiological evidence of a J-shaped relationship where moderate consumption may reduce coronary heart disease risk (by raising HDL cholesterol and increasing tissue plasminogen activator). However, a 2024-2026 Burden of Proof meta-analysis found J- or U-shaped relationships for ischemic heart disease and ischemic stroke, but emphasises that high levels of consumption are harmful across all outcomes.
- Katzung's Basic and Clinical Pharmacology, p. 627
4. Cancer Risk
Alcohol is a Group 1 carcinogen (IARC). It increases the risk of cancers of the:
- Head and neck (lip, oral cavity, pharynx, larynx)
- Oesophagus
- Liver (hepatocellular carcinoma)
- Colorectum
- Breast
- Stomach, pancreas, prostate
The 2024 Mendelian randomisation systematic review (PMID 39574800) provides genetic causal evidence linking alcohol to these cancers, supporting a dose-response relationship even at low-to-moderate drinking levels.
5. Gastrointestinal Tract
- Chronic pancreatitis: alcohol is the most common cause in the Western world - it directly damages pancreatic acinar cells and promotes protein plug and stone formation
- Gastritis with increased protein/blood loss
- Small intestine injury: diarrhoea, weight loss, vitamin deficiencies
- Malabsorption of water-soluble vitamins (especially B vitamins) is severe
6. Endocrine & Metabolic
- Hypoglycaemia: from impaired hepatic gluconeogenesis
- Ketosis: from increased cortisol and growth hormone-driven lipolysis
- Gynecomastia and testicular atrophy in men (sex hormone imbalance)
- Fluid/electrolyte imbalances: ascites, oedema, hypokalemia
7. Blood
- Folic acid deficiency anaemia (most common haematologic disorder)
- Iron-deficiency anaemia (from GI bleeding)
- Haemolytic syndromes
- Bone marrow suppression (reduced proliferation of all cell types)
8. Immune System
Chronic alcohol suppresses immune function, increasing susceptibility to:
- Pneumonia and lower respiratory infections
- Tuberculosis
- Post-injury infections
- Katzung's Basic and Clinical Pharmacology
9. Fetal Alcohol Syndrome (FAS)
Alcohol is a leading cause of preventable intellectual disability and congenital malformation. FAS features:
- Intrauterine growth retardation
- Microcephaly
- Poor coordination
- Flattened midface
- Minor joint anomalies
- Congenital heart defects and intellectual disability in severe cases
Ethanol rapidly crosses the placenta. The fetal liver lacks alcohol dehydrogenase, so the fetus cannot clear it. The mechanism involves apoptotic neurodegeneration and aberrant neuronal/glial migration.
- Katzung's Basic and Clinical Pharmacology, p. 628
Current Evidence Update (2025-2026)
A comprehensive Burden of Proof analysis (Nature Health, 2026) reviewed 843 cohort and case-control studies across 20 health outcomes and found:
- Increased risk at any level for 10+ cancers, pancreatitis, cirrhosis, lower respiratory infections, tuberculosis, and atrial fibrillation
- J/U-shaped relationships for type 2 diabetes, Alzheimer's disease, ischaemic heart disease, and stroke
- High consumption is harmful across all 20 outcomes without exception
Per Johns Hopkins researchers (Nov 2025), public awareness of alcohol's cancer risk still significantly lags the science. The US Surgeon General issued an advisory in 2025 recommending that alcoholic beverages carry cancer warning labels.
Summary Table
| System | Key Harms |
|---|---|
| Liver | Fatty liver → hepatitis → cirrhosis → liver failure |
| Nervous system | Dementia, Wernicke/Korsakoff, neuropathy, cerebellar degeneration |
| Cardiovascular | Cardiomyopathy, hypertension, atrial fibrillation |
| Cancer | Head/neck, oesophagus, liver, colorectum, breast, stomach, pancreas |
| GI tract | Pancreatitis, gastritis, malabsorption, vitamin deficiencies |
| Endocrine | Hypoglycaemia, sex hormone disruption, electrolyte imbalance |
| Blood | Anaemia (folate/iron), haemolysis, bone marrow suppression |
| Immune | Increased infection risk (pneumonia, TB) |
| Fetus | Fetal alcohol syndrome, intellectual disability, malformations |
Sprain
Reading File
Finding Sources
Searching PubMed
"sprain" AND "ligament injury" AND management
Searching the Web
sprain definition classification grading treatment 2025
Reading File
Finding Sources
Searching PubMed
"ankle sprain" AND rehabilitation
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have rich, comprehensive information. Let me compile the full answer.
Sprain - Complete Overview
Definition
A sprain is a complete or partial tear of a ligament - the fibrous connective tissue that connects bone to bone and stabilises joints. This distinguishes it from a strain, which is an injury to a muscle or tendon (muscle-to-bone connection).
Sprains occur when a joint is forced beyond its normal range of motion, stretching or tearing the ligament at the joint or at its bony insertion/origin.
- Swanson's Family Medicine Review, p. 844
Classification by Grade
Sprains are universally graded I through III based on the extent of ligament disruption:
| Grade | Ligament Damage | Signs & Symptoms | Weight Bearing |
|---|---|---|---|
| I | Microscopic tears only; ligament intact | Tenderness, minimal swelling, no laxity | Possible with minimal pain |
| II | Partial tear | Moderate swelling, ecchymosis, some pain, little or no instability | Difficult |
| III | Complete rupture | Severe swelling, prominent ecchymosis, no endpoint on stress testing | Usually impossible |
Joint stability - not just pain - is the primary determinant of treatment planning.
- Tintinalli's Emergency Medicine, p. 1233; Swanson's Family Medicine Review
Most Common Sites
1. Lateral Ankle (Most Common Overall)
The anterior talofibular ligament (ATFL) is the single most commonly injured ligament in the body. The mechanism is typically inversion with plantarflexion - the foot rolls inward and downward. The three lateral ankle ligaments in order of injury frequency:
- ATFL - restricts anterior talar translation; torn in plantarflexed inversion
- CFL (calcaneofibular ligament) - restricts inversion; torn in dorsiflexed inversion
- PTFL (posterior talofibular ligament) - restricts posterior translation; rarely torn in isolation
Textbook of Family Medicine, 9e
2. Medial Ankle (Deltoid Ligament)
Isolated medial (deltoid) ligament sprains are rare. When present, they are usually associated with a fibular fracture or tibio-fibular syndesmosis tear from an eversion injury. Always suspect a Maisonneuve fracture (proximal fibula) if there is significant medial malleolus tenderness with negative ankle radiographs.
- Tintinalli's Emergency Medicine
3. Knee (Medial Collateral Ligament - MCL)
Mechanism: a blow to the lateral side of the knee. Presents with medial-side swelling and laxity on valgus stress testing. Lachman test is negative (that tests the ACL).
4. Thumb (Ulnar Collateral Ligament - "Skier's Thumb")
UCL sprain of the 1st MCP joint. Grade III tears may require surgery. Initial treatment: thumb spica splint.
- Swanson's Family Medicine Review
5. Wrist, Shoulder (AC Joint), and others
Acromioclavicular joint sprains are graded using the Rockwood classification: Grade I (ligament sprain, no displacement) through Grade III+ (complete disruption with clavicle elevation).
- Grainger & Allison's Diagnostic Radiology
Clinical Assessment
History
- Mechanism of injury (inversion? eversion? twisting?)
- Audible "pop" (suggests complete tear)
- Ability to bear weight immediately after
Physical Examination
- Inspection: oedema, ecchymosis, deformity
- Palpation: localise tenderness to specific ligaments and bony landmarks
- Stress testing:
- Anterior drawer test - translates talus forward; tests ATFL integrity
- Talar tilt test - inverts talus; tests CFL integrity
- Compare to the uninjured side for excursion and endpoint feel
When to X-Ray: Ottawa Ankle Rules
X-ray is required if there is pain in the malleolar zone AND any one of the following:
- Bone tenderness along the distal 6 cm of the posterior tibia or tip of medial malleolus
- Bone tenderness along the distal 6 cm of the posterior fibula or tip of lateral malleolus
- Inability to bear weight both immediately after injury AND in the clinic (4 steps)
The Ottawa Rules have ~99% sensitivity for ruling out fractures and significantly reduce unnecessary radiographs.
- Rheumatology, 2-Volume Set (Elsevier)
Treatment
Immediate: PRICE Protocol (first 24-72 hours)
Protection - Rest - Ice - Compression - Elevation
- Ice reduces swelling and pain; apply for 20 min, several times daily
- Compression bandage (elastic/tubular) limits oedema
- Elevation above the level of the heart
Functional Rehabilitation (evidence-based preference over immobilisation)
Current evidence favours early functional treatment over casting/immobilisation. Patients return to mobility 4.6 to 7.1 days sooner with functional rehabilitation vs. immobilisation:
Phase 1 (0-24 hours): PRICE protocol
Phase 2 (48-72 hours onward): Active range of motion and strengthening exercises begin. Early weight bearing hastens healing and return to activity. An ankle support brace is preferred over a cast.
Phase 3 (ongoing): Endurance training, sport-specific drills, and proprioceptive/balance training - this is essential to prevent chronic ankle instability.
For severe (Grade III) sprains, a below-knee cast or Aircast produces faster early recovery than a tubular bandage alone, though outcomes at 9 months are equivalent.
- Goldman-Cecil Medicine; Tintinalli's Emergency Medicine
Medications
- NSAIDs (e.g. ibuprofen, naproxen) for pain and swelling
- Corticosteroid injections are not indicated in acute sprain management
Surgery
Rarely required for sprains. Indications include:
- Grade III with persistent instability after conservative management
- Chronic ankle instability unresponsive to physiotherapy
- Associated osteochondral lesion or avulsion fracture
Complications of Untreated/Severe Sprains
- Chronic ankle instability - recurrent giving-way, the most common long-term complication
- Osteochondral defects of the talus or tibia
- Avulsion fracture (e.g. at the base of the 5th metatarsal - often missed)
- Peroneal tendon subluxation - must be distinguished from lateral ligament sprain
- Post-traumatic arthritis (long term)
If ankle pain becomes chronic after a sprain, always consider ligament rupture, osteochondral lesion, or avulsion fracture, and proceed with CT (bony) or MRI (soft tissue) imaging.
- Rheumatology, 2-Volume Set
Sprains vs. Strains - Quick Reference
| Feature | Sprain | Strain |
|---|---|---|
| Structure injured | Ligament (bone-to-bone) | Muscle or tendon (muscle-to-bone) |
| Mechanism | Joint overstretched/twisted | Muscle overloaded or overstretched |
| Common sites | Ankle, knee, wrist, thumb | Hamstring, quadriceps, calf, lower back |
| Stress test | Often positive (laxity) | Negative (no joint laxity) |
Recent Evidence (2025)
A 2025 systematic review on return to sport after lateral ankle sprain (PMID 41385332) found that neuromuscular training and proprioception work are the most evidence-backed strategies for safe return to sport. A 2025 network meta-analysis on chronic ankle instability (PMID 39741454) showed that combined physical therapy approaches (balance + strengthening + manual therapy) outperform single-modality treatment for function and stability.
This is a shared conversation. Sign in to Orris to start your own chat.