Weaning off criteria
Reading File
Finding Sources
Searching PubMed
mechanical ventilation weaning criteria liberation
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough, well-structured answer. Here it is:
Weaning Off (Liberation from Mechanical Ventilation) Criteria
Weaning refers to the process of discontinuing mechanical ventilation. The modern preference is to frame this as active liberation rather than a slow passive wean - approaching removal of ventilator support passively can extend unneeded mechanical ventilation time by up to 40%.
Step 1: Daily Readiness Screening
Before attempting a spontaneous breathing trial (SBT), the following criteria should be met:
| Domain | Criterion |
|---|---|
| Underlying disease | Primary cause of respiratory failure has improved or resolved |
| Neurological | Awake, alert, and largely off sedation; able to follow commands |
| Oxygenation | FiO₂ ≤ 0.5 (≤40-50%), PEEP < 8 cmH₂O, SpO₂/SaO₂ > 88-90% |
| Ventilation | pH at patient baseline, PaCO₂ at baseline; minute ventilation < 10 L/min; RR < 30 breaths/min |
| Hemodynamics | Stable; no vasopressors or weaning off; no active myocardial ischemia |
| Secretions/Airway | Thin, manageable secretions; suctioning ≤ every 4 hrs; adequate cough; able to lift head off bed and hold for >5 sec |
Sources: Washington Manual of Medical Therapeutics; Harrison's Principles of Internal Medicine 22e; Morgan & Mikhail's Clinical Anesthesiology 7e
Step 2: Mechanical/Quantitative Weaning Parameters
These indices help predict readiness:
| Parameter | Threshold for Readiness |
|---|---|
| Rapid Shallow Breathing Index (RSBI = f/VT) | ≤ 100-105 breaths/min/L |
| Tidal volume (spontaneous) | > 5 mL/kg IBW |
| Vital capacity | > 10 mL/kg |
| Maximum inspiratory pressure (MIP / NIF) | < -25 cmH₂O (more negative = stronger) |
| Minute ventilation | < 10 L/min |
RSBI formula: RSBI = Respiratory rate (breaths/min) ÷ Tidal volume (L)
- RSBI > 105 accurately predicts weaning failure
- RSBI ≤ 105 is less reliable at predicting weaning success alone
- Sensitivity ~0.90 (good screening test); combine with other criteria for confirmation
Source: Morgan & Mikhail's Clinical Anesthesiology 7e, Table 58-5; Washington Manual
Step 3: Spontaneous Breathing Trial (SBT)
Once readiness criteria are met, proceed to an SBT:
- Duration: 30 to 120 minutes
- Method: Minimal pressure support (5-7 cmH₂O PSV) to compensate for ETT resistance, or T-piece trial
- The patient "passes" if: comfortable throughout, no distress, maintains acceptable SpO₂, stable RR and HR
SBT failure signs (stop trial if present):
- RR > 35 breaths/min
- SpO₂ < 90%
- HR/BP changes > 20% from baseline, or arrhythmias
- Agitation, diaphoresis, use of accessory muscles
- Worsening mental status
- PaCO₂ rise ≥ 10 mmHg or pH < 7.32
A single daily SBT is as effective as multiple daily trials. If the patient fails, provide 24 hours of full ventilator rest before retrying.
Step 4: Extubation Decision
Passing an SBT does not automatically mean the patient is safe to extubate. Additional checks:
- Cuff leak test: If laryngeal edema is suspected (angioedema, traumatic intubation), absence of cuff leak should preclude extubation; treat with IV corticosteroids for 12-24 hrs first
- Neurological safety: Intact airway reflexes, able to protect airway; a cooperative patient is ideal
- Note: ~10-23.5% of patients who pass all criteria still fail extubation
Weaning Algorithm (Harrison's 22e)
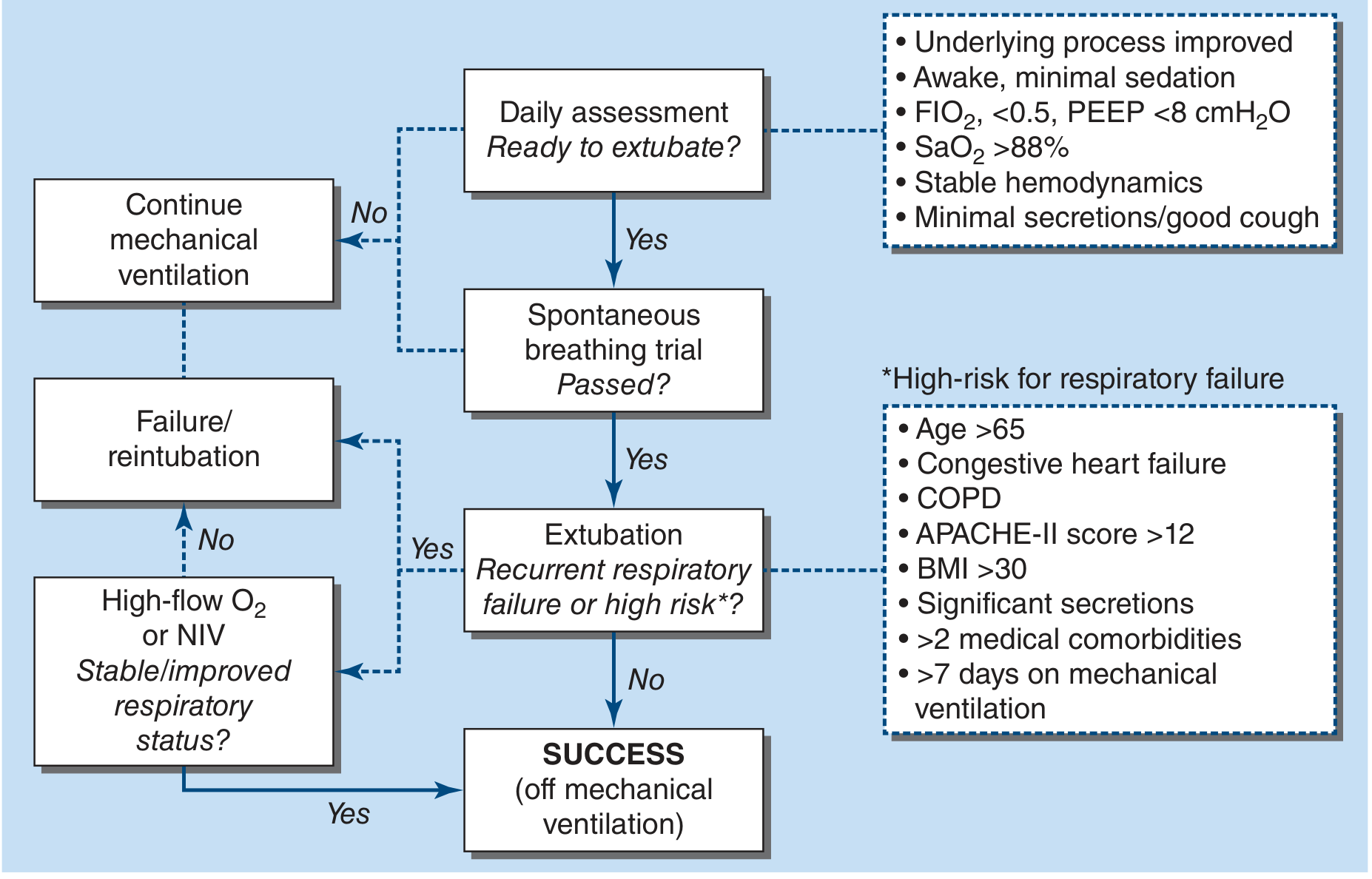
Figure: Daily assessment → SBT → Extubation. High-risk patients (age >65, CHF, COPD, APACHE-II >12, BMI >30, significant secretions, >2 comorbidities, >7 days on MV) should receive post-extubation NIV or high-flow oxygen.
SBT Methods Compared
| Method | Description | Evidence |
|---|---|---|
| T-piece trial | Patient disconnected from ventilator, breathes through humidified T-circuit | Weaning time 3x shorter vs. IMV |
| PSV trial | Low pressure support (5-10 cmH₂O) + PEEP 5 cmH₂O | Equivalent to T-piece in most studies |
| IMV reduction | Mandatory rate reduced gradually | Longest weaning time; may cause respiratory muscle fatigue; least preferred |
| Daily T-piece (single trial) | Once-daily 30-120 min trial | As effective as multiple daily trials; simpler |
Sources: Fishman's Pulmonary Diseases and Disorders; Washington Manual of Medical Therapeutics
Causes of Weaning Failure (to address before retrying)
- Worsening respiratory mechanics (increased resistance/stiffness during spontaneous breathing)
- Cardiovascular stress: increased right and left ventricular afterload, decreased O₂ delivery
- Rapid shallow breathing with dead-space hypercapnia
- Critical illness myopathy/polyneuropathy
- CHF or volume overload
- Delirium, malnutrition
- Electrolyte abnormalities: hypophosphatemia, hypokalemia, hypomagnesemia
- Suboptimal sedation management
Post-Extubation Strategy
- High-risk patients (age >65, CHF, COPD, prolonged MV): apply NIV immediately after extubation before ARF develops - reduces reintubation and mortality
- Established post-extubation ARF: NIV may be futile and can delay reintubation; high-flow O₂ is preferred for most patients
- Protocol-driven extubation readiness reduces ventilator days by ~25% and ICU stay by ~10%
Key clinical takeaway: The biggest source of delayed weaning is physicians failing to consider that a patient may be ready. Use daily standardized screening + RSBI + a 30-120 min SBT as a two-step approach. Don't wait for complex testing - a screening test that triggers the SBT is the most important step.
Recent guideline: The 2024 AARC Clinical Practice Guideline on SBTs (PMID 38443142) provides updated recommendations for liberation from adult mechanical ventilation.
This is a shared conversation. Sign in to Orris to start your own chat.