Vitiligo
Reading File
Finding Sources
Searching PubMed
vitiligo
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive information. Let me compile a detailed, well-structured answer on vitiligo.
Vitiligo
Vitiligo is an acquired autoimmune skin disease characterized by progressive loss of epidermal melanocytes, resulting in well-defined milky-white macules and patches. It affects approximately 0.5-1% of the global population and can carry significant psychosocial burden.
Clinical Appearance
The classic lesion of vitiligo is a well-defined, depigmented (chalk-white) macule or patch with smooth, convex margins, often surrounded by normal or hyperpigmented skin. Hairs within the patches may also depigment - this is called poliosis.
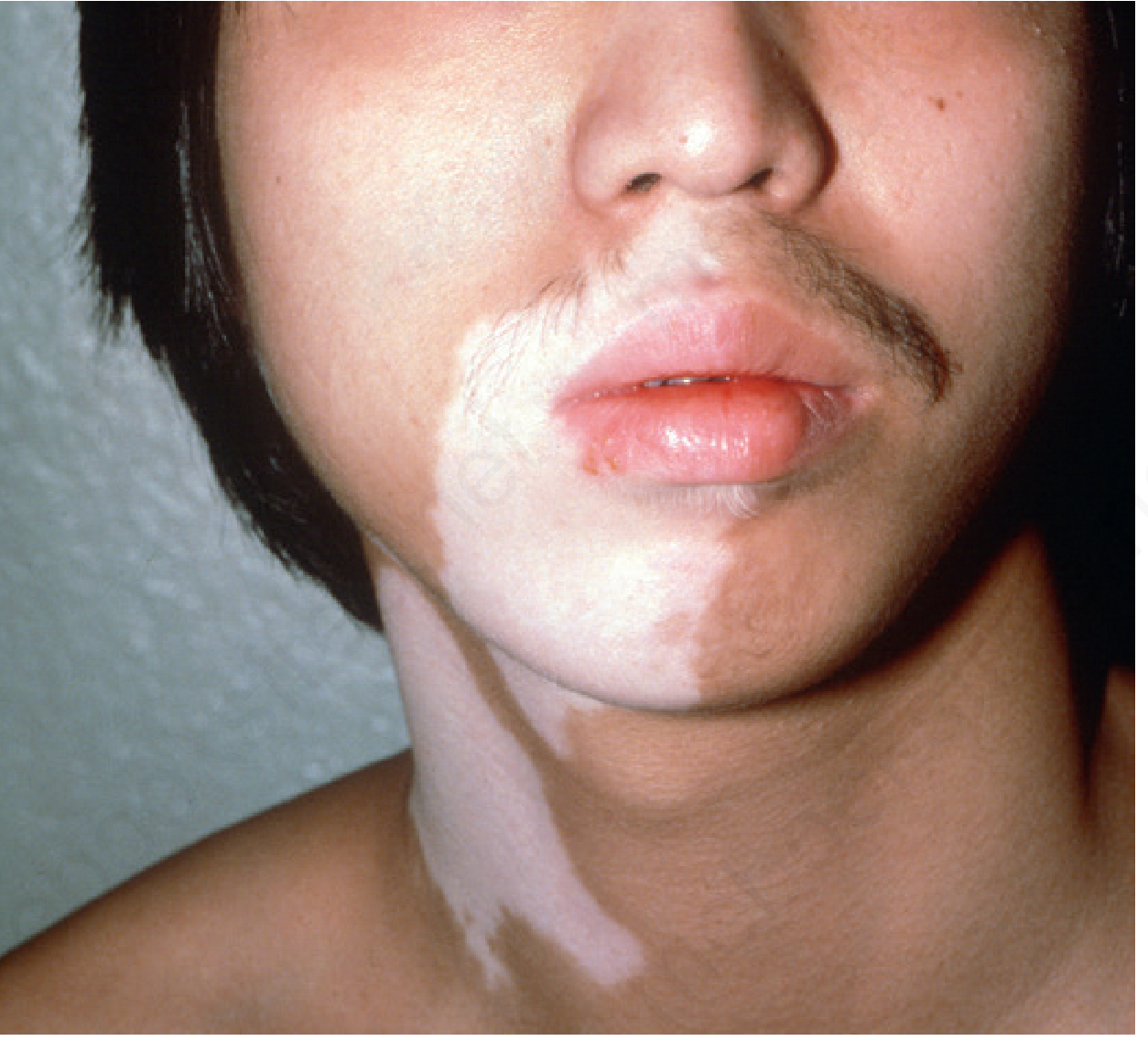
Segmental vitiligo: well-demarcated depigmented patch involving the perioral region and neck - Andrews' Diseases of the Skin, p. 1001
Trichrome vitiligo (an early or active sign) shows 3 zones: depigmented center, hypopigmented intermediate zone, and normally pigmented skin at the border. The patches favor periorificial areas (eyes, mouth, nose, ears, nipples, umbilicus, genitalia), acral areas, and sites of trauma (elbows, knees - the Koebner phenomenon).
Classification / Types
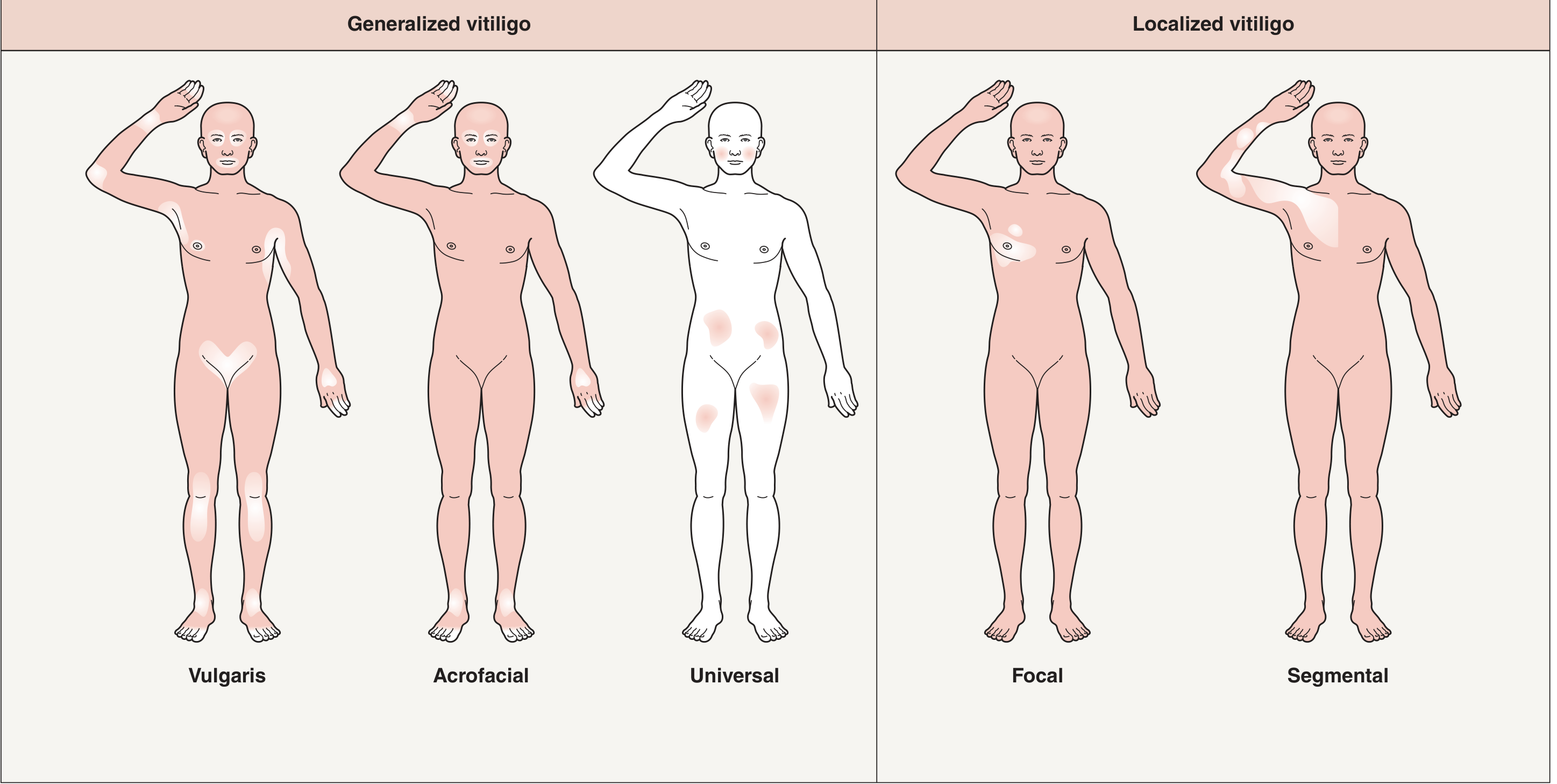
Classification of vitiligo by distribution pattern - Dermatology 2-Volume Set 5e, p. 1310
| Type | Description |
|---|---|
| Vulgaris (Common) | Most common; symmetric bilateral patches on face, hands, trunk |
| Acrofacial | Distal fingers and perioral/periorbital areas |
| Universal | Near-total body depigmentation (>80% BSA) |
| Segmental | Unilateral, dermatomal-like, block-like pattern; does NOT cross midline |
| Focal | Single or few macules in one area (e.g., glans penis, trigeminal area in children) |
| Mucosal | Mucous membranes only |
Generalized (vulgaris) is the most common pattern. Segmental vitiligo is clinically distinct - it tends to be stable, is less responsive to systemic treatment, and has different pathogenesis (less autoimmune, more neurogenic component).
Epidemiology
- Prevalence: ~0.5-1% worldwide; up to 8% in some regions of India
- Average age of onset: ~30 years; ~50% of cases begin before age 20
- Peak onset: 10-30 years
- No definitive sex predilection, though females seek care more often
- Associated with other autoimmune diseases: thyroid disease (most common - ~20-30% have thyroid autoantibodies), type 1 diabetes, Addison's disease, pernicious anemia, alopecia areata, rheumatoid arthritis
- Interestingly, vitiligo patients have a decreased risk of skin cancer (likely due to heightened immune surveillance against melanocytes)
Pathogenesis
The pathogenesis is multifactorial, involving genetic susceptibility + melanocyte stress + autoimmune destruction.
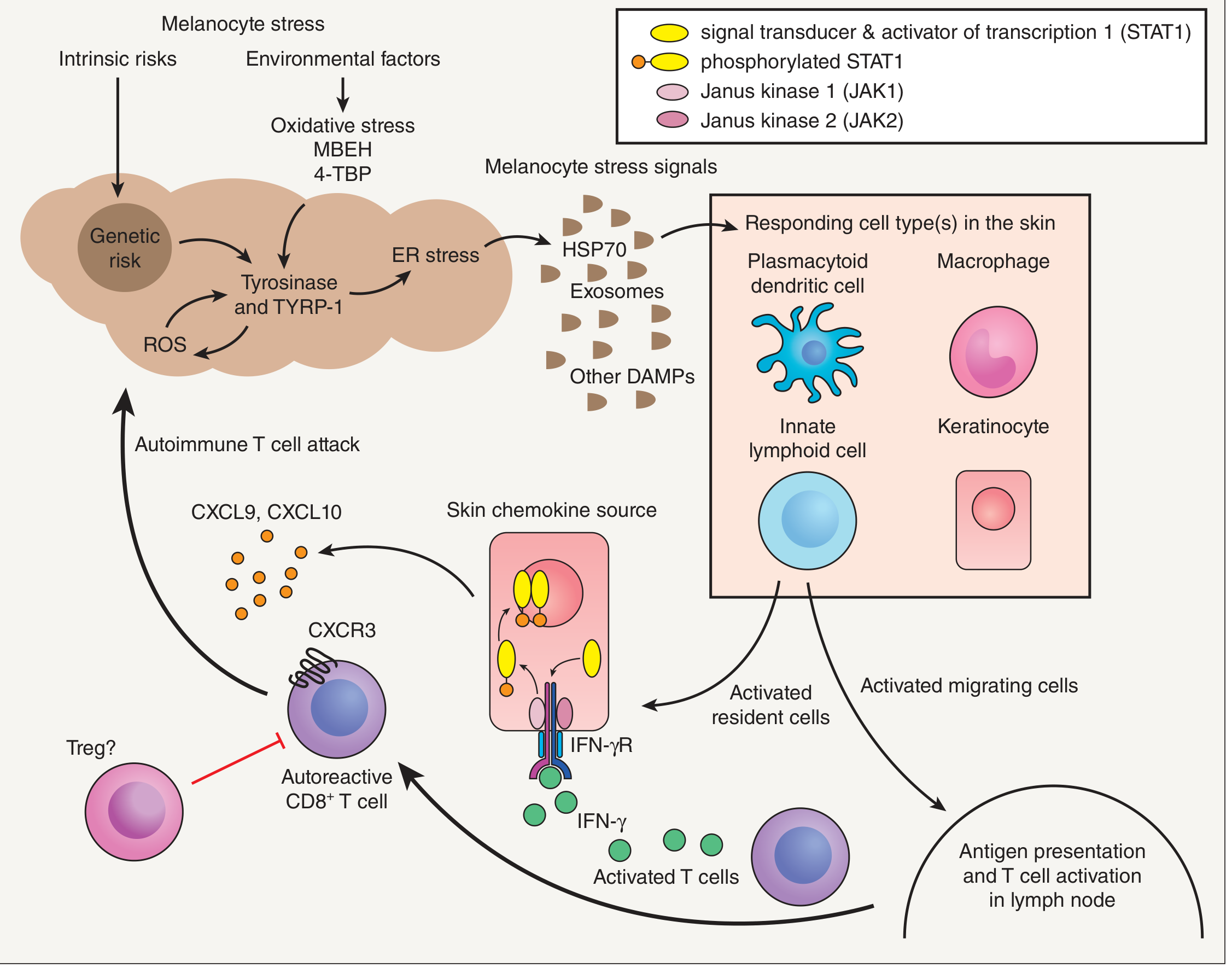
Proposed pathogenesis model of vitiligo - Dermatology 2-Volume Set 5e, p. 1308
Step by step:
-
Genetic risk - Multiple susceptibility loci identified (genes involved in melanogenesis, immune regulation, apoptosis). 7% of first-degree relatives of vitiligo probands have vitiligo; 23% concordance in monozygotic twins (confirming environmental component).
-
Melanocyte stress - Intrinsic melanocyte abnormalities (increased oxidative stress, ROS, ER stress) make melanocytes vulnerable. Environmental triggers include phenolic chemicals (tyrosine analogs), UV exposure, and emotional stress. Oxidative stress also impairs WNT signaling (normally promotes melanocyte precursor differentiation).
-
Innate immune activation - Stressed melanocytes release DAMPs (HSP-70, HMGB1), which activate plasmacytoid dendritic cells and innate lymphoid cells to secrete IFN-α and IFN-γ.
-
Adaptive immune cascade - IFN-γ signals through IFN-γR on keratinocytes, activating JAK1/2 → phospho-STAT1 → transcription of CXCL9 and CXCL10. These chemokines recruit autoreactive CD8+ cytotoxic T cells expressing CXCR3, which kill melanocytes.
-
Memory and relapse - Resident memory T cells (CD69+, CD103+, CD49a+) remain in skin and mediate relapse at previously affected sites.
The IFN-γ → JAK-STAT → CXCL9/10 axis is the central therapeutic target, explaining why JAK inhibitors (e.g., ruxolitinib) are effective.
Clinical Markers of Disease Activity
| Sign | Significance |
|---|---|
| Koebner phenomenon | Depigmentation at sites of skin trauma; indicates active disease, predicts poor treatment response |
| Trichrome vitiligo | 3-color zones at border; indicates rapidly spreading, active disease |
| Confetti depigmentation | Multiple tiny depigmented macules at lesion edges; indicates rapid progression |
| Inflammatory border | Rare; red border indicates active lesion |
| Poliosis | White hairs in lesion; indicates follicular melanocyte loss; predicts poorer repigmentation |
Diagnosis
Diagnosis is primarily clinical. Key tools:
- Wood's lamp (365 nm UV) - enhances contrast in a dark room; turns vitiligo chalky-white/bright; distinguishes complete depigmentation from hypopigmentation (helpful in fair-skinned patients)
- Dermoscopy - reveals reticular pigmentation pattern at borders; can show perifollicular pigmentation (sign of repigmentation)
- Skin biopsy - usually unnecessary; shows complete absence of melanocytes; melanophages may be present; mild lymphocytic infiltrate at edges in active disease
- Laboratory workup - screen for associated autoimmune conditions: TSH, anti-TPO/anti-Tg antibodies, fasting glucose, CBC (pernicious anemia)
Differentials to exclude:
- Pityriasis alba (hypopigmented, not depigmented; indistinct borders; in children)
- Tinea versicolor (hypopigmented; KOH positive)
- Post-inflammatory hypopigmentation (history of preceding dermatitis)
- Leprosy (hypopigmented, hypoesthetic patches; ill-defined borders)
- Chemical leukoderma (contact with phenolic compounds; patterned distribution)
- Piebaldism (congenital; white forelock; stable patches)
- Pityriasis lichenoides chronica
- Halo nevus (depigmented ring around a nevus)
Treatment
Treatment depends on extent, activity, and location of disease. Repigmentation is only possible in areas with viable melanocyte reservoirs - i.e., areas with pigmented hairs (follicular melanocyte stem cells). Glabrous skin (lips, fingertips) and areas with white hairs respond poorly.
1. Topical Therapies (limited disease, <5-10% BSA)
| Agent | Notes |
|---|---|
| Topical corticosteroids (Class I-II) | First-line; ~50% achieve >75% repigmentation; best response on face/neck; use in 6-8 week cycles to prevent atrophy; avoid eye area |
| Topical calcineurin inhibitors (tacrolimus 0.1%, pimecrolimus 1%) | Preferred for face, neck, intertriginous areas, children; 65% repigmentation of facial lesions with tacrolimus in RCT; combine with phototherapy for synergy |
| Topical ruxolitinib 1.5% (JAK1/2 inhibitor) | FDA-approved (2022) for non-segmental vitiligo ≥12 years; significant repigmentation in clinical trials |
2. Phototherapy (moderate/widespread disease)
| Modality | Details |
|---|---|
| Narrowband UVB (NB-UVB) | Treatment of choice for widespread vitiligo; 2-3 sessions/week; safe in pregnancy and children; best results on face and trunk |
| Excimer laser (308 nm) | Targeted phototherapy for localized lesions; delivers higher UV doses to small areas |
| PUVA (psoralen + UVA) | Effective but largely replaced by NB-UVB; higher phototoxicity and carcinogenicity risk |
3. Systemic Therapies (rapidly progressive disease)
| Agent | Use |
|---|---|
| Oral mini-pulse corticosteroids (e.g., dexamethasone 2.5 mg on 2 consecutive days/week) | Arrests progression in active vitiligo; used short-term |
| Oral JAK inhibitors (ruxolitinib, baricitinib - investigational/emerging) | Target the JAK-STAT pathway systemically |
4. Surgical Options (stable vitiligo)
For stable segmental vitiligo or lesions non-responsive to medical treatment:
- Split-thickness skin grafting
- Suction blister epidermal grafting
- Melanocyte-keratinocyte transplantation
- Best results in segmental type; contraindicated in active (koebnerizing) disease
5. Depigmentation (extensive, >50-80% BSA)
When the burden of residual pigmented skin is greater than depigmented skin, patients may opt for complete depigmentation:
- Monobenzone (monobenzyl ether of hydroquinone) 20% - applied twice daily for 3-6 months to remaining pigmented areas; permanent; requires psychiatric counseling beforehand
- Topical 4-methoxyphenol (mequinol) 20%
- Q-switched laser - selectively destroys remaining melanocytes
6. Ancillary / Supportive
- Sunscreen (SPF 30+) - vitiligo patches lack photoprotection; reduce sunburn risk; also prevents tanning of surrounding skin (which worsens contrast)
- Camouflage cosmetics - significant improvement in QoL
- Psychological support - counseling, support groups; vitiligo causes significant depression and social stigma, especially in darker skin phototypes
Repigmentation Pattern
Repigmentation appears first in a perifollicular pattern (small pigmented dots around hair follicles, as melanocyte stem cells migrate outward from follicular bulge), and also from the periphery of lesions at the border of normal skin. After therapeutic repigmentation, relapse rate is ~40%.
Prognosis
- Vitiligo is often a lifelong, relapsing condition with unpredictable flares
- Segmental vitiligo tends to stabilize within 1-2 years and does not spread beyond its initial distribution
- Non-segmental vitiligo is more progressive and unpredictable
- Only areas with pigmented (non-poliotic) hairs can fully repigment
- Glabrous skin (lips, fingertips, nipples) and areas with leukotrichia respond poorly
Sources:
- Fitzpatrick's Dermatology, 9e - Chapter 76: Vitiligo (Ezzedine & Harris), pp. 1358-1375
- Dermatology 2-Volume Set, 5e - Chapter 66: Vitiligo, pp. 1307-1315
- Andrews' Diseases of the Skin, Clinical Dermatology - Chapter 36: Vitiligo, pp. 1000-1003
A 2025 systematic review on off-label topical ruxolitinib (PMID 40192197) confirms emerging use of JAK inhibitors in vitiligo treatment, supporting the textbook guidance above.
This is a shared conversation. Sign in to Orris to start your own chat.