Tell me about histamine and their receptors present in the stomach and what happens on its blockage or inhibition.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive, well-sourced information from multiple authoritative textbooks and two excellent diagrams. Let me compile the full answer.
Histamine and Its Receptors in the Stomach
1. Histamine - Overview
Histamine is a biogenic amine synthesized from the amino acid L-histidine by the enzyme histidine decarboxylase. In the gastrointestinal tract, it is produced primarily by enterochromaffin-like (ECL) cells of the gastric mucosa, as well as by enteric nerves and mast cells in submucosal connective tissue.
There are four types of histamine receptors (H1, H2, H3, H4), all belonging to the G protein-coupled receptor (GPCR) family. In the stomach, the most important is the H2 receptor, though all subtypes are present to varying degrees:
| Receptor | Location in GI Tract | G-Protein Coupling | Primary Function |
|---|---|---|---|
| H1 | Smooth muscle, vascular endothelium | Gq → PLC → IP3/DAG → Ca²⁺ | Allergic responses, smooth muscle contraction |
| H2 | Parietal cells (main), smooth muscle, cardiac myocytes | Gs → adenylate cyclase → cAMP | Gastric acid secretion |
| H3 | CNS, ECL cells of GI tract | Gi → inhibits adenylate cyclase | Neurotransmitter release modulation, autoreceptor |
| H4 | Immune cells | Gi-linked | Immune system function |
- Robbins, Cotran & Kumar Pathologic Basis of Disease
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
2. Role of the H2 Receptor in Gastric Acid Secretion
The H2 receptor on parietal cells is the central regulator of acid secretion. Here is how it works:
The ECL Cell - Parietal Cell Axis
The parietal cell receives three major stimulatory inputs:
- Histamine (via H2 receptor) - from ECL cells (paracrine)
- Gastrin (via G/CCK-B receptor) - from G cells of the antrum (endocrine)
- Acetylcholine (via M3 muscarinic receptor) - from vagal nerve endings (neurocrine)
The critical link: Gastrin and acetylcholine do not just act directly on parietal cells - they also stimulate ECL cells to release histamine, which then acts parautocrinally on nearby parietal cells. This makes histamine the final common mediator of acid secretion.
"The acid stimulatory effect of gastrin is largely mediated by histamine released from mucosal ECL cells." - Schwartz's Principles of Surgery
Intracellular Signalling Cascade
When histamine binds to the H2 receptor on the parietal cell:
- H2 receptor activates Gs protein
- Gs stimulates adenylate cyclase → converts ATP to cAMP
- cAMP activates protein kinase A (PKA)
- PKA activates the H⁺/K⁺-ATPase proton pump
- The proton pump secretes H⁺ ions into the gastric lumen in exchange for K⁺, forming HCl
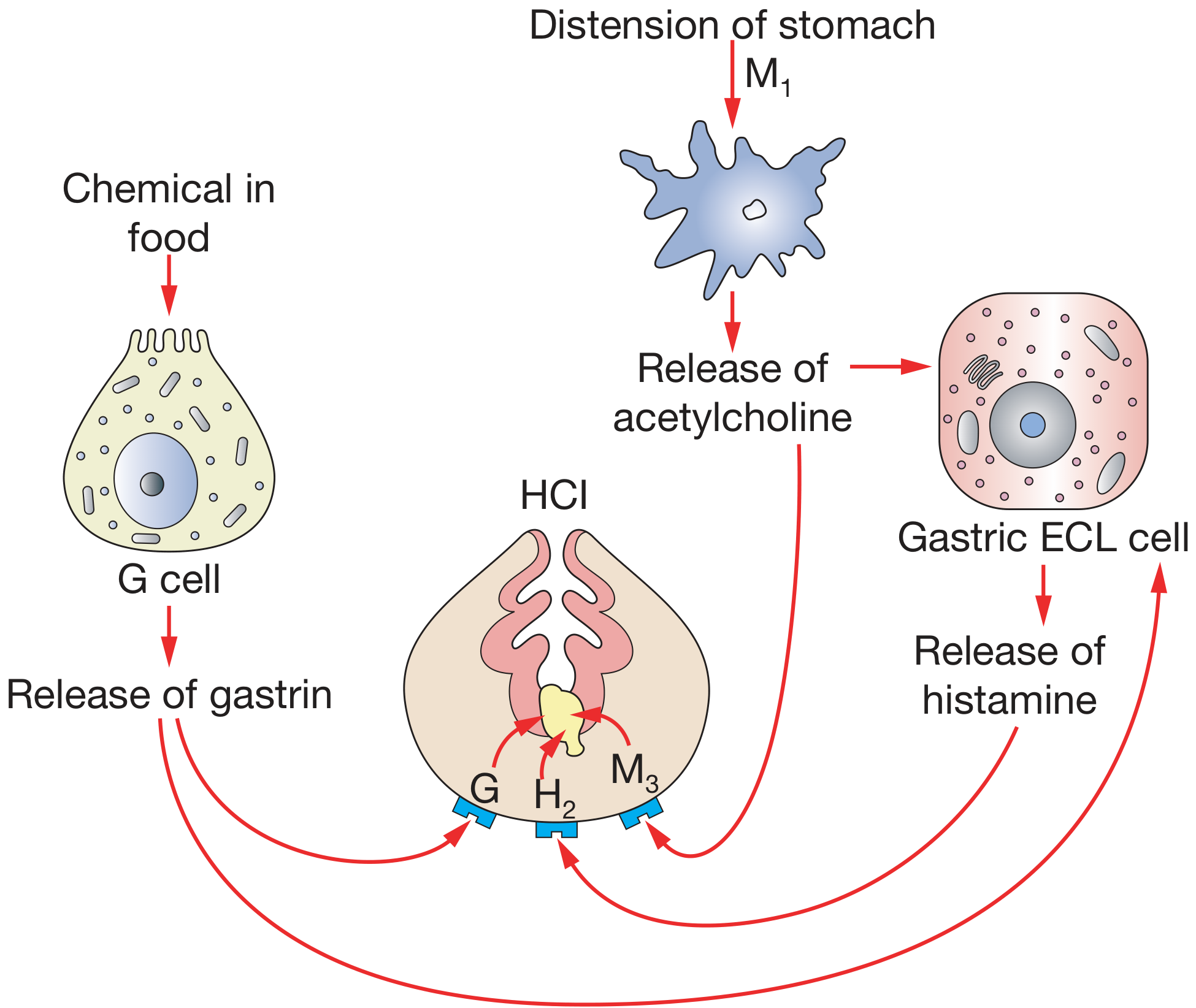
Figure: The parietal cell and mechanism of gastric acid secretion. ECL = enterochromaffin-like cell; G = gastrin receptor; H = H2 histamine receptor; M = muscarinic receptor. (Bailey and Love's Short Practice of Surgery)
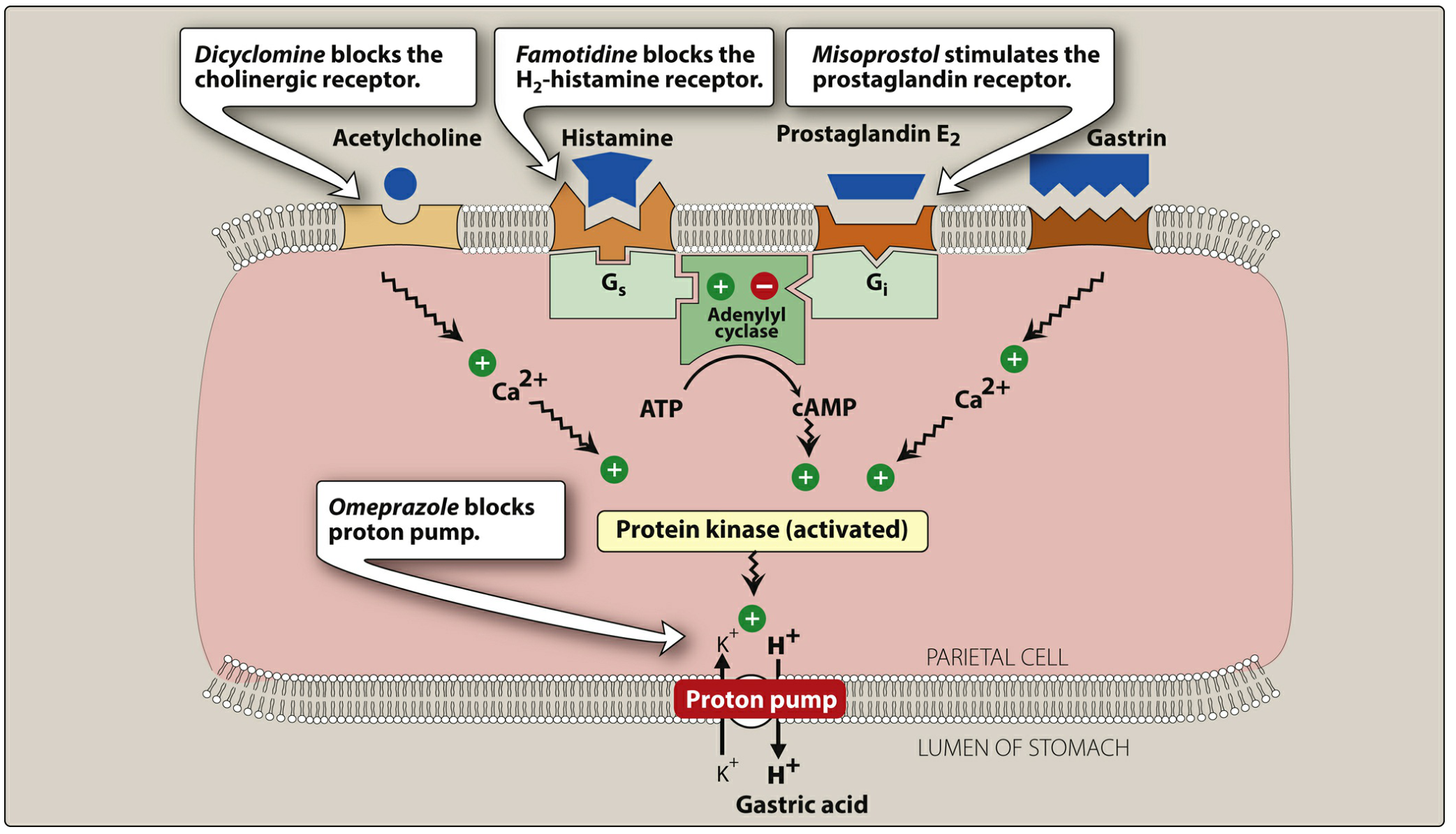
Figure: Signaling pathways in the parietal cell. Note that famotidine (H2 blocker) blocks H2 receptor; omeprazole blocks the proton pump directly; misoprostol stimulates the inhibitory prostaglandin receptor (Gi). (Lippincott Illustrated Reviews: Pharmacology)
3. Negative Feedback on Acid Secretion
- Gastric acid itself inhibits G cell gastrin release (negative feedback loop)
- Somatostatin from D cells inhibits ECL cells and parietal cells
- Prostaglandin E2 (via Gi protein) inhibits adenylate cyclase and reduces cAMP, thereby decreasing acid secretion - this is why NSAIDs (which block prostaglandin synthesis) increase ulcer risk
4. The Three Phases of Gastric Secretion
| Phase | Trigger | Mechanism |
|---|---|---|
| Cephalic | Sight, smell, taste of food | Vagal stimulation → ACh → M3 on parietal cells + ECL cells |
| Gastric | Food in stomach | Gastrin from G cells → ECL histamine release → H2 on parietal cells |
| Intestinal | Chyme in duodenum | Initially stimulates, then secretin and other peptides inhibit further secretion |
5. What Happens on H2 Receptor Blockade (H2 Receptor Antagonists)
Mechanism of Action
H2 receptor antagonists (H2RAs) competitively and reversibly block histamine at H2 receptors on parietal cells. They have no effect on H1 receptors. By blocking cAMP generation, they prevent activation of the proton pump.
"H1 antagonists had no effect on histamine-induced acid secretion in the stomach. Molecular manipulation of the histamine molecule resulted in drugs that blocked acid secretion." - Katzung's Basic and Clinical Pharmacology
Effect: H2RAs inhibit basal, food-stimulated, and nocturnal gastric acid secretion by approximately 70%.
- Unlike PPIs (which abolish >90% of acid), H2RAs only markedly reduce acid - they cannot fully block acid because gastrin and ACh can still directly stimulate parietal cells.
- PPIs act on the final common pathway (the pump itself) and are therefore more potent.
Available H2 Receptor Antagonists
| Drug | Brand Name | Notes |
|---|---|---|
| Cimetidine | Tagamet | First H2RA; inhibits CYP450 enzymes; anti-androgenic effects |
| Famotidine | Pepcid | No CYP450 interactions; most potent of the class |
| Nizatidine | Axid | Similar to famotidine |
| Withdrawn (NDMA carcinogen contamination) |
Clinical Uses of H2 Blockade
- Peptic ulcer disease (gastric and duodenal ulcers) - All H2RAs equally effective; however, recurrence is high if H. pylori is not eradicated
- GERD / heartburn - Reduce acid secretion; onset ~45 min (slower than antacids)
- Acute stress ulcer prophylaxis - Used as IV infusion in ICU settings (tolerance may develop)
- Zollinger-Ellison syndrome - High doses can be used, though PPIs are preferred
Adverse Effects
- Cimetidine-specific:
- Gynecomastia and galactorrhea - acts as a nonsteroidal anti-androgen
- Confusion, altered mentation - particularly in elderly and with IV use
- Drug interactions - strongly inhibits CYP450 isoenzymes, raising levels of warfarin, phenytoin, clopidogrel, theophylline
- Class effects:
- Reduced absorption of drugs needing acidic environment (e.g., itraconazole, ketoconazole)
- Tolerance may develop with prolonged use (tachyphylaxis)
- Generally well tolerated
6. Comparison: H2 Blockers vs. PPIs
| Feature | H2 Receptor Antagonists | Proton Pump Inhibitors (PPIs) |
|---|---|---|
| Site of action | H2 receptor on parietal cell | H⁺/K⁺-ATPase (proton pump) |
| Acid suppression | ~70% | >90% |
| Effect on nocturnal acid | Good | Excellent |
| Onset | 1-3 hours | Requires 3-5 days for full effect |
| Tolerance | Can develop | Rare |
| Examples | Cimetidine, famotidine | Omeprazole, pantoprazole, rabeprazole |
- Lippincott Illustrated Reviews: Pharmacology
- Bailey and Love's Short Practice of Surgery, 28th Ed.
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, 7th Ed.
Summary: The H2 receptor on gastric parietal cells is the key target through which histamine (released by ECL cells) drives HCl production via the Gs-cAMP-PKA-proton pump axis. H2 blockade with drugs like famotidine reduces acid secretion by ~70%, making them useful for peptic ulcer disease, GERD, and stress ulcer prophylaxis - though PPIs, which act downstream at the proton pump itself, provide more complete acid suppression and are now preferred for most indications.
This is a shared conversation. Sign in to Orris to start your own chat.