POPLITEAL ARTERY ANEURYSM
"popliteal artery aneurysm"[MeSH Terms] AND management
Popliteal Artery Aneurysm (PAA)
Definition and Epidemiology
- Overwhelmingly affects men in their seventh decade of life
- ~50% are bilateral - the contralateral limb must always be examined
- 30-40% are associated with abdominal aortic aneurysm (AAA) - bilateral PAAs increase this risk further
- Up to 75% of PAA patients have aortic ectasia or aneurysm (Sabiston)
- Most are fusiform, true degenerative aneurysms associated with smoking, age, and hypertension
Clinical rule: Every patient diagnosed with a PAA requires ultrasound interrogation of the contralateral popliteal artery and the abdominal aorta. Conversely, all AAA patients should be screened for PAA.
Anatomy
- P1: adductor hiatus to the superior border of the patella
- P2: superior border of the patella to the center of knee articulation
- P3: knee articulation to the origin of the anterior tibial artery
Natural History
- Rupture is rare in true PAAs; any rupture should raise suspicion of a false/mycotic aneurysm
- ~1/3 of PAAs will thrombose within 5 years of diagnosis
- The mechanism: mural thrombus within the aneurysm sac embolizes to distal run-off vessels over time; as successive run-off vessels occlude, flow in the sac diminishes and eventually the aneurysm thromboses acutely
- By the time acute thrombosis occurs, the outflow vessels are chronically diseased, making reconstruction difficult and the limb loss rate as high as 50%
- Risk factors for progression: larger index size at presentation, presence of intramural thrombus, concurrent AAA
Clinical Presentation
| Presentation | Features |
|---|---|
| Incidental/asymptomatic | Prominent popliteal impulse on examination, found during AAA screening |
| Pulsatile mass | Swelling behind the knee, expansile and pulsatile, audible bruit |
| Compressive symptoms | Leg swelling (venous compression), DVT, restricted range of motion, nerve compression |
| Distal embolism | Toe/foot ischemia ("blue toe"), claudication, rest pain |
| Acute limb ischemia | Thrombosed aneurysm - white, painful, pulseless, paralyzed, cold limb |
Differential Diagnosis
- Popliteal artery aneurysm - pulsatile, bruit on auscultation
- Baker's (popliteal) cyst - synovial outpouching from the posteromedial knee between the medial gastrocnemius head and semimembranosus tendon, non-pulsatile
- Arterial adventitial cyst - uncommon cystic structure from the artery wall
- Benign or malignant tumor
Investigation
- Vein mapping (to assess ipsilateral and contralateral great saphenous vein)
- Baseline ankle-brachial index (ABI)
- Lower extremity CTA/MRA/conventional arteriogram
Indications for Repair
| Scenario | Recommendation |
|---|---|
| Asymptomatic PAA ≥2 cm, healthy patient | Elective repair |
| Asymptomatic PAA, high-risk patient | Defer until ≥3 cm (if no intraluminal thrombus) |
| Any aneurysm with intraluminal thrombus | Repair regardless of size |
| Any aneurysm with signs of ipsilateral thromboembolism | Repair regardless of size |
| All symptomatic PAAs | Repair |
| All pseudoaneurysms | Repair |
Treatment
Open Surgical Repair (Gold Standard)
- Single-segment great saphenous vein (GSV) ≥3 mm diameter - ideal
- Short saphenous or cephalic vein
- Expanded PTFE or allograft (no-conduit cases)
- Patient supine, knee flexed and externally rotated
- Preferred for aneurysms extending beyond the popliteal fossa
- Proximal and distal incisions, tunnel created, bypass performed with saphenous vein or prosthetic graft
- The PAA must be ligated both proximally and distally as close as possible to the sac (failure to isolate may cause sac expansion and late rupture from patent geniculate collaterals)
- Patient prone
- Advantageous for large aneurysms confined to the popliteal space, allows aneurysmectomy and direct ligation of geniculate branches
- Limits exposure of superficial femoral and crural arteries - only use when aneurysm is confined to the popliteal fossa
- Short saphenous vein can be harvested in the prone position
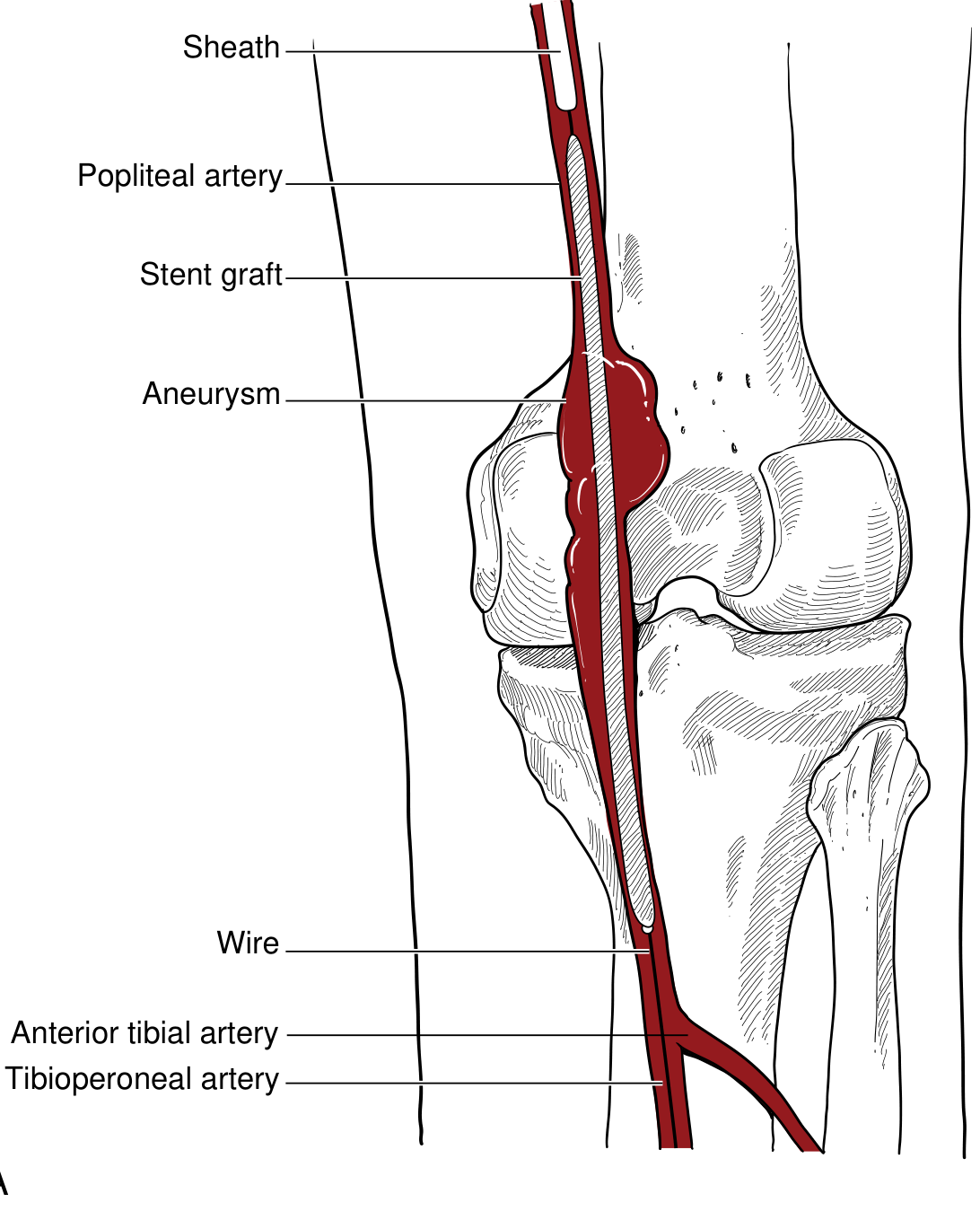
Endovascular Repair
- Proximal and distal landing zones ≥15 mm in healthy vessel
- Minimal aneurysmal kinking or tortuosity
- Good tibiopedal runoff (≥2 patent vessels)
- Stent grafts oversized 10-15%; if multiple stents required, 2 cm overlap recommended
- Angiography with the knee flexed is performed to confirm stent sizing and avoid termination at the point of maximum flexure
- Aneurysms not crossing the knee (proximal popliteal / distal SFA)
- Patients of advanced age with significant medical comorbidities
- Patients who are NOT expected to survive ≥5 years (guidelines favor open for those with ≥5-year life expectancy)

Acute Presentation (Thrombosed PAA with Limb Ischemia)
- Initiate anticoagulation immediately
- CTA or conventional angiography - assess aneurysm thrombosis, extent of distal embolization, tibiopedal runoff
- If motor/sensory function intact (mild ischemia): catheter-directed thrombolysis to restore runoff, followed by definitive repair
- If profound/limb-threatening ischemia: immediate OR - thromboembolectomy of popliteal and tibial vessels (± pharmacomechanical thrombolysis), aneurysm exclusion, and bypass
- If compartment syndrome suspected or confirmed: 4-compartment fasciotomy
- Non-viable limb: primary amputation rather than futile revascularization
Postoperative Surveillance and Medical Therapy
- Duplex ultrasound at 3, 6, and 12 months during the first year, then annually
- Monitor for: graft patency, excluded sac size, flow
- Aspirin 81 mg indefinitely as minimum antiplatelet therapy
- Dual antiplatelet or anticoagulation: individualized risk-benefit assessment
- Standard cardiovascular risk-reduction: statins, antiplatelet agents, angiotensin blockade as indicated
Key Points Summary
| Feature | Detail |
|---|---|
| Most common peripheral aneurysm | 70-80% of all peripheral aneurysms |
| Demographics | Males, 7th decade |
| Bilateral | ~50% |
| Associated AAA | 30-40% (up to 75% have some aortic ectasia) |
| Dominant complication | Thromboembolism, NOT rupture |
| Diagnostic standard | Duplex ultrasound |
| Surgical gold standard | Exclusion bypass with saphenous vein (medial approach) |
| Indication threshold | ≥2 cm asymptomatic OR any thrombus OR any symptoms |
| Acute ischemia mortality | Limb loss up to 50% with thrombosed PAA |
reactive inguinal lymph node usg images
reactive inguinal lymph node ultrasound sonography features images
reactive lymph node ultrasound B-mode oval echogenic hilum hypoechoic cortex normal benign
Reactive Inguinal Lymph Node - Ultrasound
Key USG Features of a Reactive Lymph Node
| Feature | Reactive (Benign) | Malignant (for comparison) |
|---|---|---|
| Shape | Oval/elliptical, preserved | Rounded (shape index >0.5) |
| Long:Short axis ratio | >2 (S/L ratio <0.5) | <2 (rounder) |
| Echogenic hilum | Present and preserved | Absent or lost |
| Cortex | Hypoechoic, concentrically thickened (uniform) | Eccentric/focal cortical thickening |
| Margins | Sharp, well-defined, smooth | Irregular, blurred, invasive |
| Vascularity (Doppler) | Hilar flow - central, radial, branching | Peripheral flow, multiple feeders, chaotic |
| Perinodal tissue | Normal | Perinodal edema, soft tissue infiltration |
| Internal echoes | Homogeneous | Necrosis, calcification, heterogeneous |
B-Mode Ultrasound - Reactive Node Anatomy
- Oval/reniform shape - the long axis is at least twice the short axis
- Hypoechoic cortex - the peripheral lymphoid tissue appears dark (hypoechoic) relative to adjacent muscle
- Echogenic (hyperechoic) central hilum - bright central stripe representing fatty/fibrovascular hilum; present in up to 92% of benign nodes
- Concentrically thickened cortex - reactive cortex thickens uniformly (symmetrically) around the hilum due to immune/inflammatory response
- Well-defined, smooth border
- No necrosis, calcification, or extracapsular infiltration
Doppler Ultrasound Features
- Hilar vascularity - blood vessels enter and branch radially from the hilum (the "hilar flow" pattern)
- Flow is central, orderly, and low-impedance
- May show increased hilar vascularity compared to a resting node (due to active immune response)
- No peripheral cortical flow - this is the key reassuring feature
- ~96% of reactive nodes demonstrate hilar flow only
USG Images
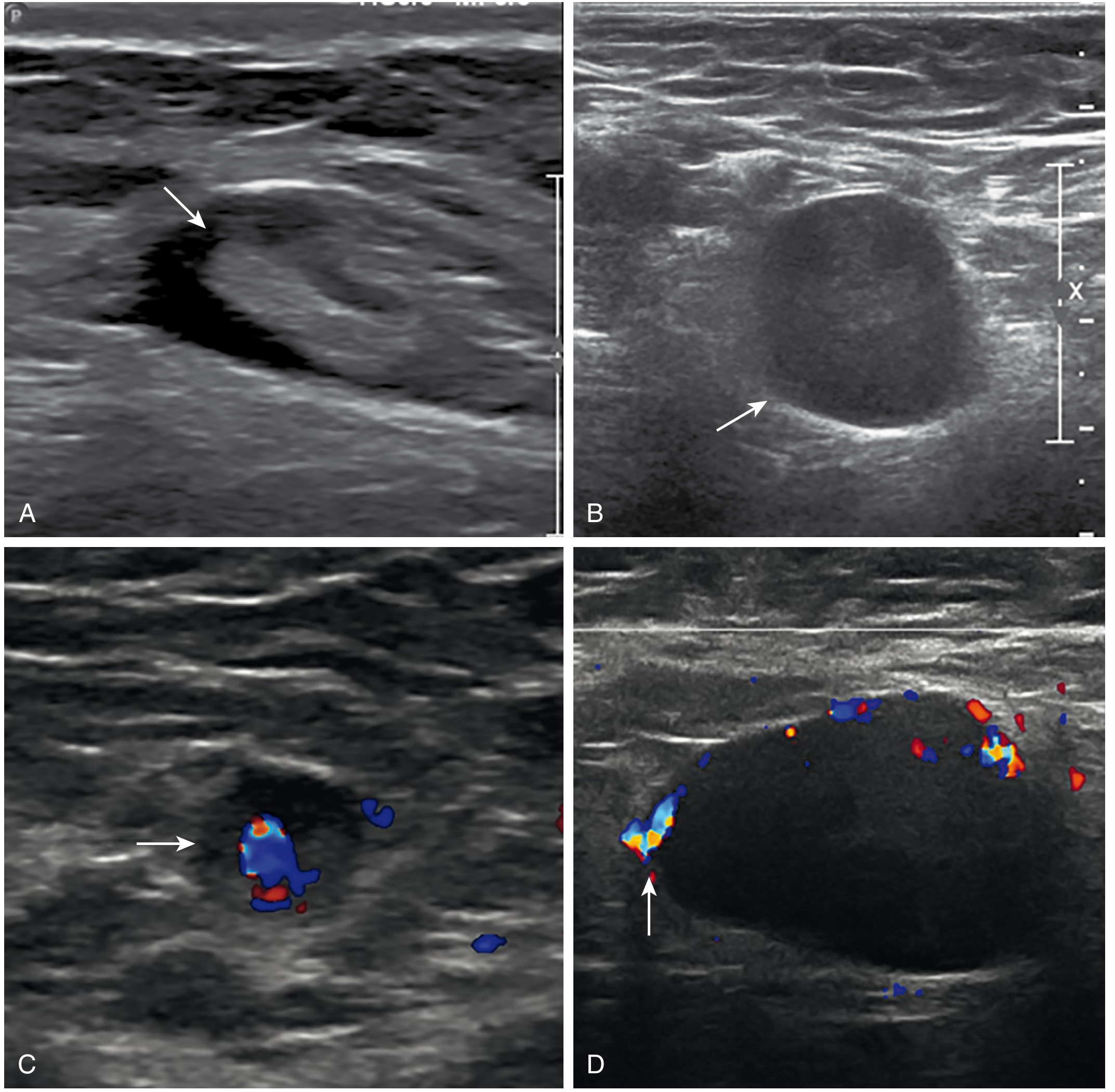
- LN1 (Benign) - Normal flat oval node, barely visible, preserved hilum
- LN2 (Probably benign/Reactive) - Oval, visible nodal-core sign, concentrically thickened hypoechoic cortex due to immune response
- LN3 (Suspicious) - Round to oval, cortex thickened, hilum may be absent
- LN4 (Probably malignant) - Rounded, inhomogeneous, markedly thickened cortex
- LN5 (Malignant) - Large, rounded, heterogeneous, no hilum


Size Criteria
- Inguinal lymph nodes up to 1.5 cm in short axis are generally considered within normal limits
- Reactive nodes may enlarge but typically do not exceed 2-3 cm and retain oval shape
- Nodes with short axis ≥1 cm (oval-shaped) or ≥0.8 cm (circular-shaped) with a malignant morphology are considered suspicious
- Size alone is unreliable - morphology and Doppler pattern are more specific
Important Differential Points
| Feature | Reactive | Suppurative/Abscess | Metastatic | Lymphoma |
|---|---|---|---|---|
| Shape | Oval | Oval to round | Round | Round |
| Hilum | Present | May be lost | Lost | Lost |
| Internal | Homogeneous | Cystic/necrotic center | Heterogeneous | Very hypoechoic, "pseudocystic" |
| Doppler | Central hilar | Hilar ± peripheral | Peripheral/chaotic | Variable |
| Margins | Sharp | Blurred (perinodal edema) | Irregular/invasive | Sharp |
| Matting | No | Yes (in TB) | No | No |
Clinical Tip
- Lower limb infections (cellulitis, wound infections, tinea pedis)
- STIs (herpes simplex, syphilis, chancroid, LGV)
- Recent vaccinations (ipsilateral lower extremity or hip)
- Inflammatory skin conditions (eczema, psoriasis)
- Post-surgical drainage from perineum, gluteal region, lower abdomen
inguinal hernia usg
inguinal hernia ultrasound sonography images direct indirect features
https://pmc.ncbi.nlm.nih.gov/articles/PMC9262670
inguinal hernia ultrasound scan direct indirect bowel contents hernia sac sonogram
inguinal hernia ultrasound bowel in hernia sac peristalsis incarcerated strangulated
Inguinal Hernia - Ultrasound (USG)
Why Use Ultrasound?
- No radiation
- Real-time dynamic assessment (Valsalva, standing position)
- Portable and immediately available
- Can visualize hernia contents (fat vs. bowel vs. fluid)
- Can assess reducibility and detect complications (incarceration, strangulation)
- Sensitivity 86%, specificity 77% (meta-analysis, Schwartz Surgery)
Relevant Anatomy on USG
- Indirect hernia - protrudes lateral to the IEA through the deep inguinal ring, travels within the inguinal canal alongside the spermatic cord
- Direct hernia - protrudes medial to the IEA through Hesselbach's triangle (weakness in transversalis fascia)
Probe Technique
- Use a high-frequency linear probe (7.5-12 MHz) for thin patients; curved probe for obese patients
- Scan in long-axis (longitudinal) and short-axis (transverse) planes along the inguinal canal
- Always perform with the patient:
- Supine at rest (baseline)
- Valsalva maneuver or coughing (to increase intra-abdominal pressure and elicit herniation)
- Standing if no hernia seen supine (increases sensitivity significantly)
- Movement (sliding) of abdominal contents through the canal during Valsalva is essential for diagnosis
Ultrasound Appearance of Hernia Contents
| Content | USG Appearance |
|---|---|
| Omental/peritoneal fat | Hyperechoic (bright), no peristalsis |
| Bowel (small/large) | Tubular structure with echogenic walls, peristalsis visible in real-time |
| Fluid | Anechoic (dark) collection within the sac |
| Mixed | Combination of the above |
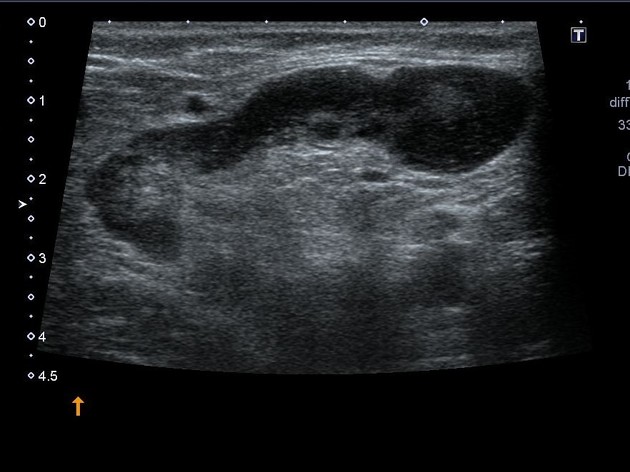
USG Images
1. Anatomy Overview - Bowel-Containing Inguinal Hernia

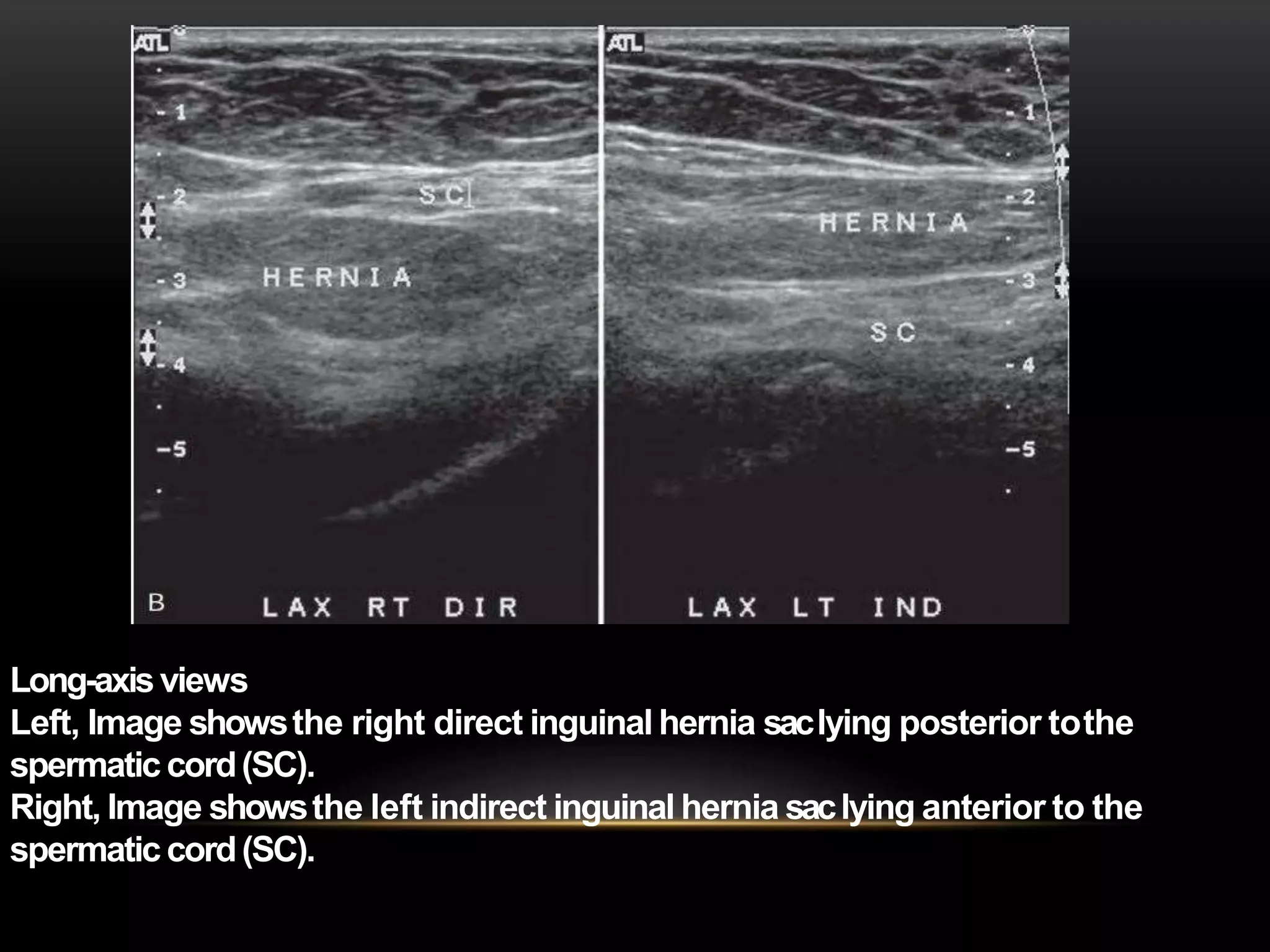
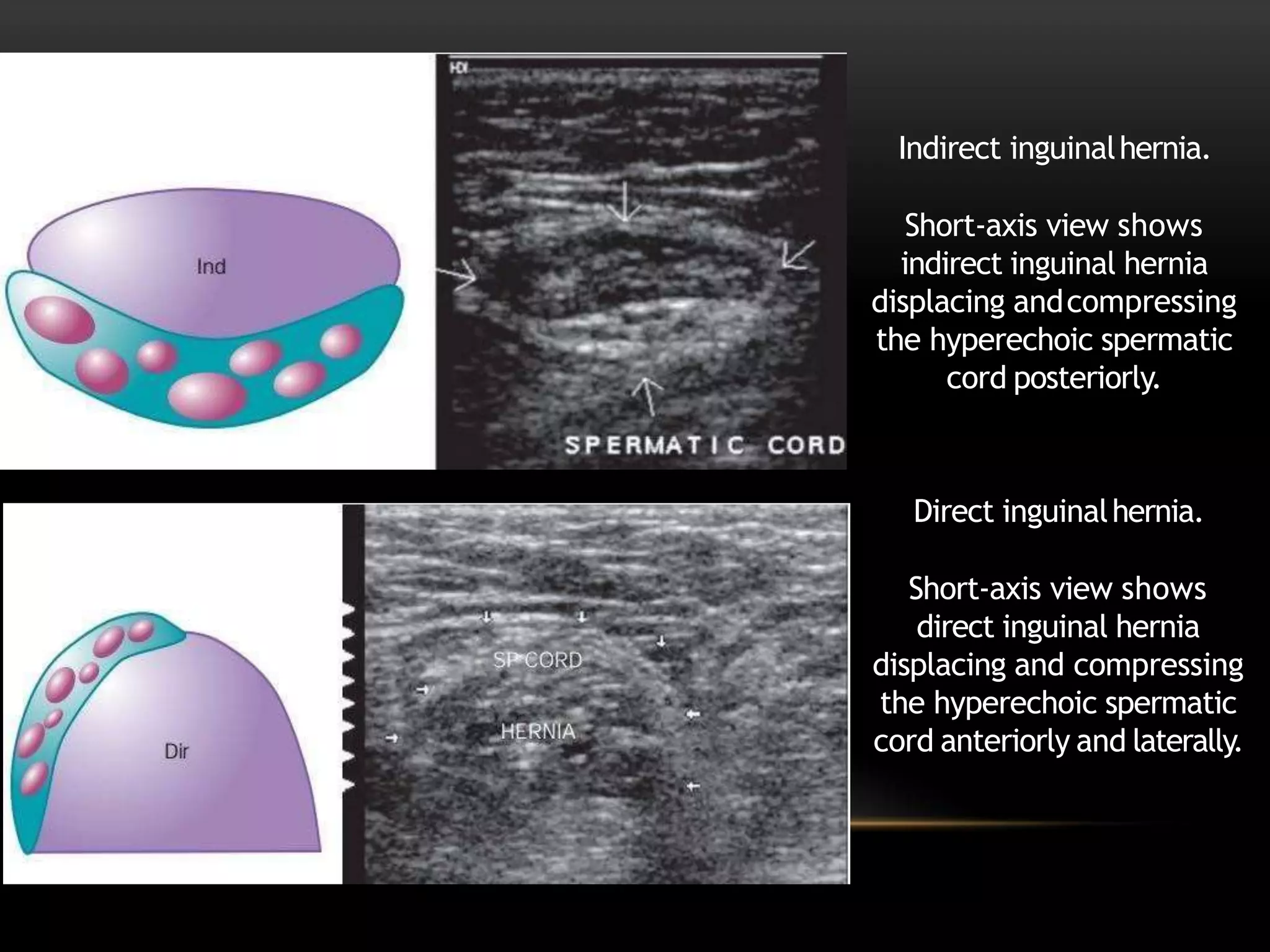
2. Direct vs. Indirect Hernia - Relationship to the Spermatic Cord
- Indirect hernia sac lies anterior to the spermatic cord - it travels with the cord through the deep ring
- Direct hernia sac lies posterior to the spermatic cord - it pushes the cord anteriorly and laterally
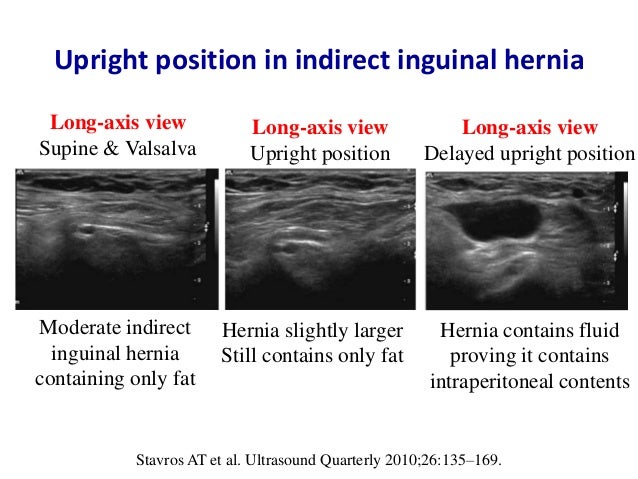
3. Dynamic Assessment - Indirect Hernia Containing Fat
4. Right Inguinal Hernia - B-Mode Scan

Distinguishing Direct from Indirect - Summary Table
| Feature | Indirect (Lateral) | Direct (Medial) |
|---|---|---|
| Relation to IEA | Lateral to IEA | Medial to IEA |
| Entry point | Deep inguinal ring | Hesselbach's triangle (through transversalis fascia) |
| Spermatic cord relation | Hernia sac anterior/anteromedial to cord | Hernia sac posterior to cord; cord pushed anteriorly |
| Canal traversal | Travels full length of inguinal canal | Does not traverse the full canal |
| Descends into scrotum | Yes (common) | Rarely |
| Valsalva direction | Protrudes anterolaterally | Protrudes anteriorly |
| Common in | Children, young adults, congenital | Older adults, degenerative |
| Dynamic movement | Moves with cord during Valsalva | Bulges separately from cord |
Assessing Complications on USG
Incarcerated Hernia
- Hernia contents cannot be reduced back into the abdomen
- Bowel loops appear non-peristaltic (absent real-time peristalsis)
- The hernia sac may contain fluid
- Apply gentle probe pressure - if sac is firm and non-reducible, incarceration is likely
- Look for bowel wall thickening, ascites, or dilated proximal bowel loops
Strangulated Hernia (Ischemic Bowel)
- Absent or reduced color Doppler flow in the bowel wall
- Thickened bowel wall (>3 mm)
- Free fluid in the sac
- Associated echogenic mesenteric fat (edema/ischemia)
- Clinical urgency - do not delay surgery for imaging
USG vs. CT in Emergencies
- POCUS is rapidly available; CT (sensitivity 90%, specificity 97%) is more definitive for incarcerated/strangulated cases
- If bowel is confidently identified in the sac with absent peristalsis and no Doppler flow, surgical consultation should not wait for CT
Postoperative USG
- Seroma - anechoic fluid collection at the repair site (common, usually resolves within 1 month)
- Hematoma - mixed echogenicity fluid collection
- Recurrence - hernia sac visible again at the repair site on Valsalva; mesh may appear as a hyperechoic structure
Differential Diagnosis of Inguinal Region Mass (USG)
| Condition | USG Features |
|---|---|
| Inguinal hernia | Mobile, reducible contents; peristalsis if bowel; increases with Valsalva |
| Reactive lymph node | Oval, echogenic hilum, hypoechoic cortex; no movement with Valsalva |
| Lipoma of cord | Hyperechoic mass; moves with spermatic cord; no reducibility |
| Femoral hernia | Inferomedial to inguinal ligament; medial to femoral vessels |
| Hydrocele | Anechoic fluid surrounding testis; transilluminates |
| Undescended testis | Oval structure with testicular echogenicity; absent ipsilateral intrascrotal testis |
| Saphena varix | Anechoic compressible structure at saphenofemoral junction; Doppler flow; disappears on compression |
| Psoas abscess | Deep hypoechoic/anechoic collection tracking along psoas; may not change with Valsalva |
Key Clinical Tips
- Always scan with Valsalva - many hernias only appear with increased intra-abdominal pressure
- Stand the patient up if supine Valsalva is negative but clinical suspicion is high
- Identify the IEA with color Doppler first - this is the key landmark for direct vs. indirect classification
- Assess both sides - contralateral hernia is common (50% lifetime risk on the other side)
- Female patients: the canal of Nuck (patent processus vaginalis) makes indirect hernias possible; Doppler is especially important as there is no spermatic cord reference structure
- Real-time peristalsis = bowel in sac - this finding alone in the inguinal region is diagnostic of bowel-containing hernia
grainger and allison textbook referance
Grainger Allison Diagnostic Radiology 7th edition 2021 Elsevier chapter list contents ISBN 9780323760751
https://inspectioncopy.elsevier.com/book/details/97807020752…
Grainger & Allison's Diagnostic Radiology - Library Reference
Bibliographic Details
| Field | Information |
|---|---|
| Full Title | Grainger & Allison's Diagnostic Radiology: A Textbook of Medical Imaging |
| Edition | 7th Edition |
| Year | 2021 |
| Publisher | Elsevier |
| ISBN (2-volume set) | 9780702075247 |
| ISBN (library copy) | 9780323760751 |
| Total Pages | ~2,217 (pp. 20-2217 in library) |
| Format | 2-volume set |
| Total Blocks (library) | 16 blocks |
Editors
| Editor | Affiliation |
|---|---|
| Andy Adam CBE, MB BS(Hons), PhD, FRCP, FRCR, FRCS | Professor of Interventional Radiology, Guy's, King's and St Thomas' School of Medicine, London, UK |
| Adrian K. Dixon MD, FRCP, FRCR, FRCS | Professor of Radiology, Addenbrooke's Hospital, University of Cambridge, Cambridge, UK |
| Jonathan H. Gillard BSc, MA, MD, FRCR, FRCP, MBA | Professor of Neuroradiology, University of Cambridge |
| Cornelia Schaefer-Prokop MD, PhD | Professor of Radiology, Meander Medical Centre, Amersfoort, The Netherlands |
Content Coverage by Block (Library)
| Block | Pages | Topics Covered |
|---|---|---|
| Block 1 | pp. 20-161 | Thoracic Imaging - Chest radiography, CT of thorax (MDCT, HRCT, dual-energy CT), Ultrasound, MRI, Radionuclide imaging (V/Q, PET); Normal lung/airway anatomy; Hila; Mediastinum |
| Block 2 | pp. 162-292 | Pleura; Thoracic wall; Diaphragm; Cardiovascular system - cardiac anatomy on imaging; Heart disease |
| Block 3 | pp. 293-432 | Cardiovascular continued - Aorta (aneurysms, dissection); Pulmonary circulation; Peripheral vascular disease; Chest wall invasion, lymph nodes |
| Block 4 | pp. 433-567 | Gastrointestinal - Pharynx, oesophagus, stomach, small bowel, large bowel imaging |
| Block 5 | pp. 568-729 | GI continued - Liver, biliary tract, pancreas, spleen, peritoneum; Abdominal trauma |
| Block 6 | pp. 730-867 | Genitourinary - Kidneys (including acquired cystic disease), ureters, bladder; Adrenal glands |
| Block 7 | pp. 868-1003 | GU continued - Male genitourinary (erectile dysfunction, penis, testes, prostate); Female pelvis |
| Block 8 | pp. 1004-1145 | Musculoskeletal - Bone tumours (radiological assessment, age/site/growth); General MSK |
| Block 9 | pp. 1146-1301 | Musculoskeletal continued - Arthropathies, trauma, spine |
| Block 10 | pp. 1302-1452 | Musculoskeletal continued / Oncological Imaging |
| Block 11 | pp. 1453-1612 | Neuroradiology - Brain (Moyamoya, vasculitis, cerebrovascular disease), skull base, temporal bone; Temporomandibular joint |
| Block 12 | pp. 1613-1743 | Neuroradiology continued - Spinal imaging |
| Block 13 | pp. 1744-1857 | Breast Imaging - Mammography, ultrasound, MRI of the breast |
| Block 14 | pp. 1858-2011 | Paediatric Radiology - Renal calculi in children; Paediatric abdomen, chest, CNS |
| Block 15 | pp. 2012-2146 | Paediatric Radiology continued - Brain tumours (desmoplastic infantile astrocytoma/ganglioglioma etc.) |
| Block 16 | pp. 2147-2217 | Interventional Radiology - Renal artery intervention, vascular interventions, image-guided procedures |
Key Features of the 7th Edition
- 2,400 pages across 2 volumes; >4,000 high-quality illustrations
- Covers the entire spectrum of imaging modalities: X-ray, CT, MRI, Ultrasound, Nuclear medicine, PET-CT, SPECT, Fluoroscopy, Angiography, Interventional radiology
- Organized on an organ and systems basis with integrated, correlative coverage of all imaging modalities
- Expanded cardiac imaging section covering cardiac MRI, 3D ultrasound, PET, and SPECT
- Functional and molecular imaging integrated throughout each section
- Includes latest image-guided biopsy and ablation techniques
- Intended audience: Radiologists in training and in practice; ideal for board/FRCR examination preparation
How to Cite (APA)
Adam, A., Dixon, A. K., Gillard, J. H., & Schaefer-Prokop, C. (Eds.). (2021). Grainger & Allison's diagnostic radiology: A textbook of medical imaging (7th ed.). Elsevier.
How to Search This Textbook in the Library
-- Search by topic (paragraph full-text)
SELECT section_heading, '/textbooks/' || block_file_path AS file_path, line_start, line_end,
snippet(paragraphs_fts, 0, '>>>', '<<<', '...', 30) AS snippet
FROM paragraphs_fts
WHERE paragraphs_fts MATCH 'your topic here'
AND book_isbn = '9780323760751'
ORDER BY rank LIMIT 10;
-- Browse table of contents
SELECT heading, block_number, line_number
FROM v_toc
WHERE book_isbn = '9780323760751'
ORDER BY block_number, line_number;
9780323760751 - use this in any query to restrict results to Grainger & Allison only.LIPOSARCOMA USG IMAGE
liposarcoma ultrasound sonography USG images features subtypes
well differentiated liposarcoma ultrasound hyperechoic vs lipoma myxoid liposarcoma cystic appearance
retroperitoneal liposarcoma ultrasound abdominal scan large heterogeneous mass
Liposarcoma - Ultrasound (USG)
Overview
WHO Subtypes and USG Characteristics
| Subtype | Frequency | USG Appearance | Grade |
|---|---|---|---|
| Atypical Lipomatous Tumour / Well-Differentiated (ALT/WDL) | 40-45% | Predominantly hyperechoic (fat-like), may mimic lipoma; look for thick/nodular septa and non-fat nodular components | Low (intermediate) |
| Myxoid | ~10% | Hypoechoic to anechoic, cyst-like, pseudocystic; myxoid matrix mimics fluid | Low-intermediate |
| Dedifferentiated | ~20% | Biphasic: hyperechoic fatty component + discrete hypoechoic solid non-lipomatous nodule | High |
| Pleomorphic | Rare | Markedly heterogeneous, hypoechoic, large; areas of necrosis/haemorrhage; no visible fat | High |
General USG Features of Liposarcoma
- Usually hyperechoic for well-differentiated types (fat content); can be highly reflective on B-mode
- Retroperitoneal liposarcomas: highly echogenic mass with anterior displacement of viscera (pancreas, aorta, IVC, kidneys, colon)
- Heterogeneous echo pattern with echo-poor centre = necrosis/haemorrhage (tumour outgrows blood supply) - strongly suggests sarcoma
- >25% non-fat component within a fatty mass = consider liposarcoma over lipoma
- Doppler: liposarcoma is more vascular than lipoma - internal vascularity on colour Doppler distinguishes the two
- USG is limited in full characterisation - MRI is the definitive modality; CT for staging
USG Red Flag Features (Distinguish from Lipoma)
| Feature | Lipoma | Liposarcoma |
|---|---|---|
| Size | Usually <5 cm | Often >10 cm |
| Echogenicity | Uniformly hyperechoic | Heterogeneous, mixed |
| Septa | Thin, fine | Thick (>2mm), nodular |
| Non-fat component | Absent | Present (>25%) |
| Depth | Superficial/subcutaneous | Deep, intramuscular/retroperitoneal |
| Colour Doppler | Absent or minimal | Internal vascularity present |
| Shape | Elliptical, smooth | Lobulated, irregular margins |
| Size change | Stable | Growing |
USG Images
1. Mayo Clinic Summary - Key USG Features of Liposarcoma

2. Retroperitoneal Liposarcoma - USG Scan

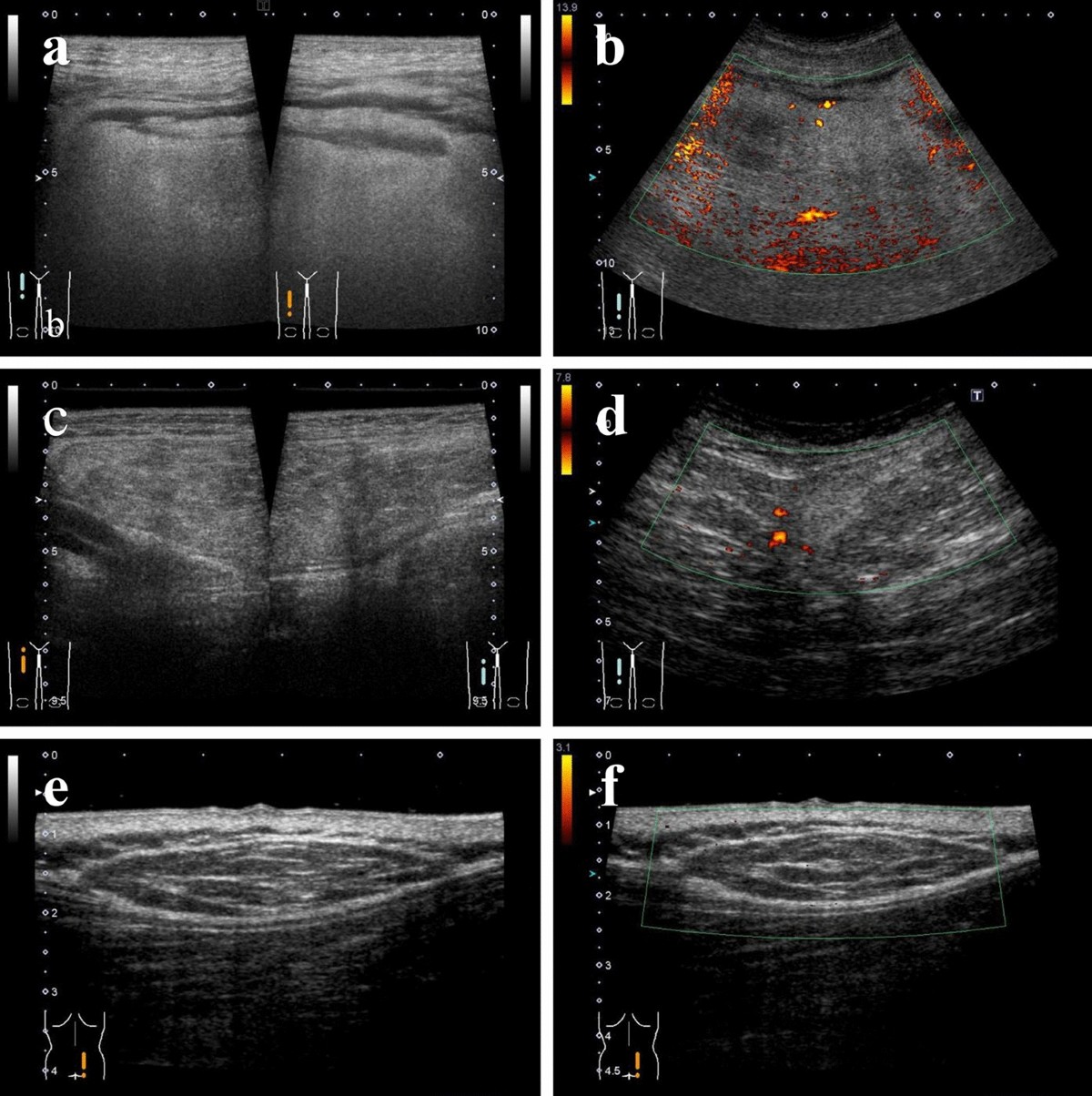
3. Liposarcoma Subtypes - USG Comparison Panel (B-mode + Doppler)
- (a, c, e) B-mode images showing varying echogenicity
- (b) Power Doppler showing rich internal vascularity in a high-grade lesion
- (d) Colour Doppler showing focal internal flow
- (e, f) Well-differentiated subtype - relatively homogeneous, hyperechoic, elongated mass
4. Well-Differentiated Liposarcoma - USG vs. Lipoma

5. Retroperitoneal Liposarcoma - CT for Correlation

6. MRI Subtype Comparison (for Radiological Correlation)
- (a) Myxoid liposarcoma - T1 dark (fluid-like myxoid stroma, arrowheads)
- (b) Dedifferentiated liposarcoma - biphasic mass with fatty and non-lipomatous nodule
- (c) Atypical lipoma/well-differentiated
- (d) Well-differentiated liposarcoma

Subtype-Specific USG Notes
Well-Differentiated / ALT
- Most common subtype; predominantly hyperechoic (fatty)
- Thickened or nodular septa and non-fat globular areas are the key red flags over benign lipoma
- Deep location (intramuscular, retroperitoneal) alone raises suspicion
- Size >10 cm, fat content <75% favour malignancy
- Doppler shows more vascularity than a lipoma
Myxoid Liposarcoma
- Contains abundant myxoid stroma (mucopolysaccharide-rich)
- On USG: hypoechoic to anechoic, may appear pseudocystic - can mimic a ganglion or simple cyst
- Posterior acoustic enhancement may be seen
- Subtle hyperechoic thin septa within the "cyst-like" area is a clue
- Unique metastatic pattern: retroperitoneum, spine (CT abdomen/pelvis and paraspinal MRI needed for staging)
Dedifferentiated Liposarcoma
- Biphasic appearance: a fatty (hyperechoic) component + a distinct solid hypoechoic non-lipomatous mass
- The solid component represents the dedifferentiated (high-grade) area
- Commonly in retroperitoneum; risk of dedifferentiation highest there (~10% of WDL)
- Doppler: internal vascularity in the solid component
Pleomorphic Liposarcoma
- Rare, high-grade
- Markedly heterogeneous, predominantly hypoechoic/solid mass with irregular margins
- Areas of central necrosis (echo-poor centre)
- Little to no identifiable fat on USG
- Rich internal vascularity on Doppler
- Indistinguishable from other high-grade soft tissue sarcomas on USG alone
Practical USG Approach
- Any deep soft tissue mass >5 cm - treat as sarcoma until proven otherwise; refer to specialist centre
- Retroperitoneal fatty mass - in contrast to extremities, lipomas are rare in retroperitoneum; assume liposarcoma until proven otherwise
- Document echogenicity, septa thickness, non-fat components, margins, depth, size
- Always apply colour/power Doppler - vascularity pattern is key in differentiating liposarcoma from lipoma
- USG-guided biopsy - core needle biopsy (not FNA) is required; target the solid/non-fat component for histological diagnosis (avoid purely fatty areas - may give false negative)
- After USG: proceed to MRI with contrast for definitive tissue characterisation and surgical planning
SYNOVIAL SARCOMA
synovial sarcoma imaging ultrasound MRI features biphasic monophasic
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.5.content.24.image.source.base64.data: At least one of the image dimensions exceed max allowed size for many-image requests: 2000 pixels
We encountered an error while processing your request. Please try again or reach out to us for help.
SYNOVIAL SARCOMA USG
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.5.content.24.image.source.base64.data: At least one of the image dimensions exceed max allowed size for many-image requests: 2000 pixels
We encountered an error while processing your request. Please try again or reach out to us for help.