Placenta accreta spectrum
Reading File
Finding Sources
Finding Sources
Searching PubMed
"placenta accreta spectrum"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive content from Creasy & Resnik's MFM and Robbins pathology. Let me compile the full answer.
Placenta Accreta Spectrum (PAS)
Definition
Placenta accreta spectrum describes the abnormal invasion of trophoblast into or through the myometrium and into adjacent extrauterine tissues. It encompasses three grades based on depth of invasion:
| Type | Invasion | Frequency |
|---|---|---|
| Accreta | Into myometrium but not full thickness | ~82% |
| Increta | Full thickness of myometrium, not beyond serosa | ~12% |
| Percreta | Beyond uterine serosa (may involve bladder, bowel, pelvic vessels) | ~6% |
The pathologic basis is complete absence of the decidua basalis (at least focally), such that placental villous tissue contacts myometrium directly - there is no Nitabuch fibrinoid layer serving as the normal boundary. The placenta therefore fails to separate at birth, causing severe postpartum hemorrhage.
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1020
- Robbins Pathologic Basis of Disease
Histology
Normal vs. accreta - the key microscopic distinction:
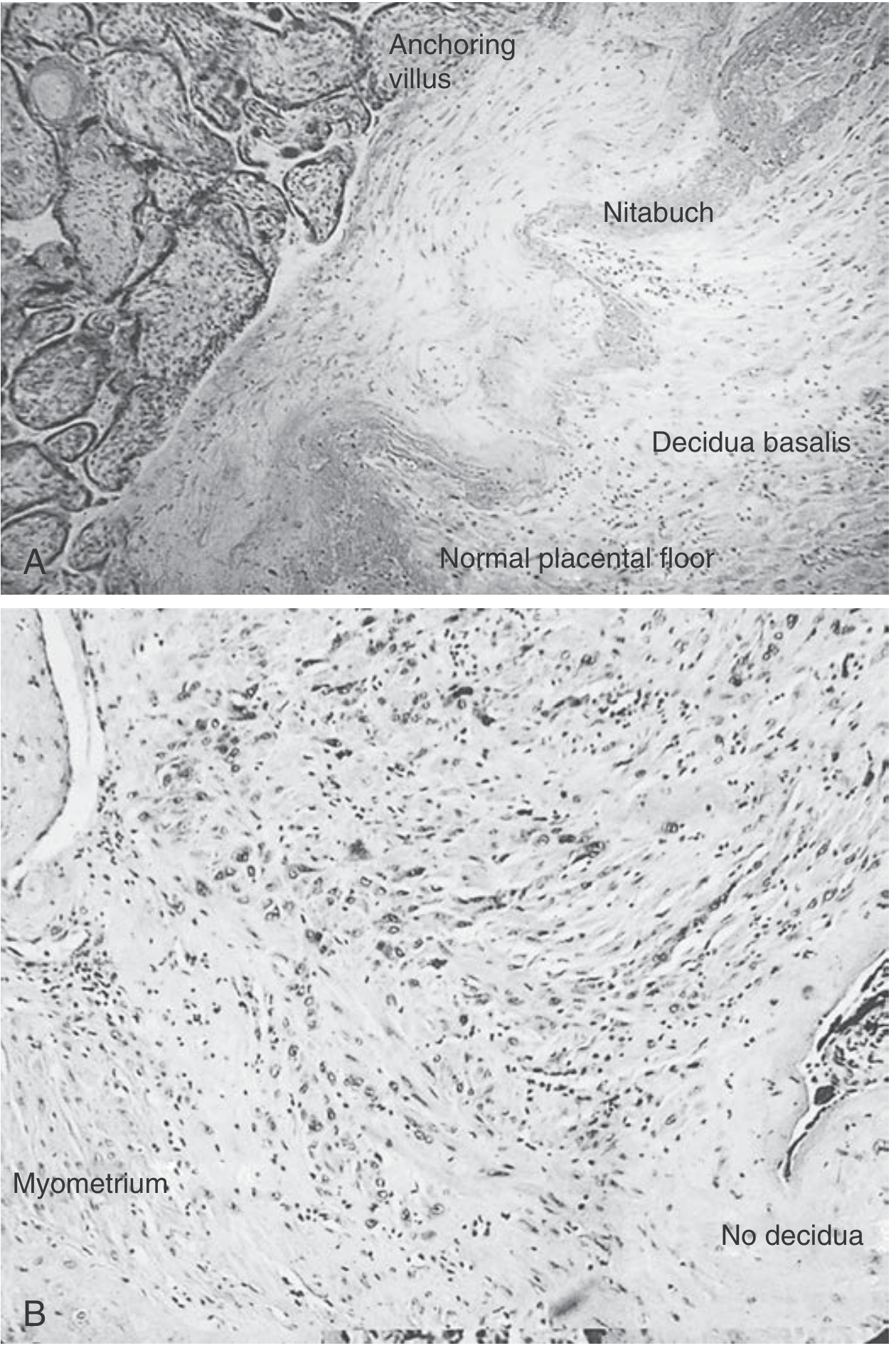
Figure 43.2 - (A) Normal: anchoring villi are held back by the Nitabuch membrane overlying decidua basalis. (B) Placenta accreta: trophoblasts invade myometrial tissue; note "No decidua" label.
Incidence
- Estimated at 1 in 300-500 pregnancies, and rising - driven by increasing cesarean delivery rates.
- Most common indication for emergency peripartum hysterectomy.
Risk Factors
The two cardinal risk factors are placenta previa and prior cesarean delivery. Their combination multiplies risk dramatically:
Risk of Accreta by Number of Prior Cesareans (% risk):
| Prior Cesareans | With Placenta Previa | Without Placenta Previa |
|---|---|---|
| 1st cesarean | 3.3% | 0.03% |
| 2nd | 11% | 0.2% |
| 3rd | 40% | 0.1% |
| 4th | 61% | 0.8% |
| 5th | 67% | 0.8% |
| ≥6th | 67% | 4.7% |
Source: SMFM Publications Committee, Am J Obstet Gynecol 2010
Other risk factors include:
- Endometrial ablation, myomectomy, uterine curettage
- Pelvic radiation
- In vitro fertilization
- Short interpregnancy interval
- Advanced maternal age, smoking, high parity
Diagnosis
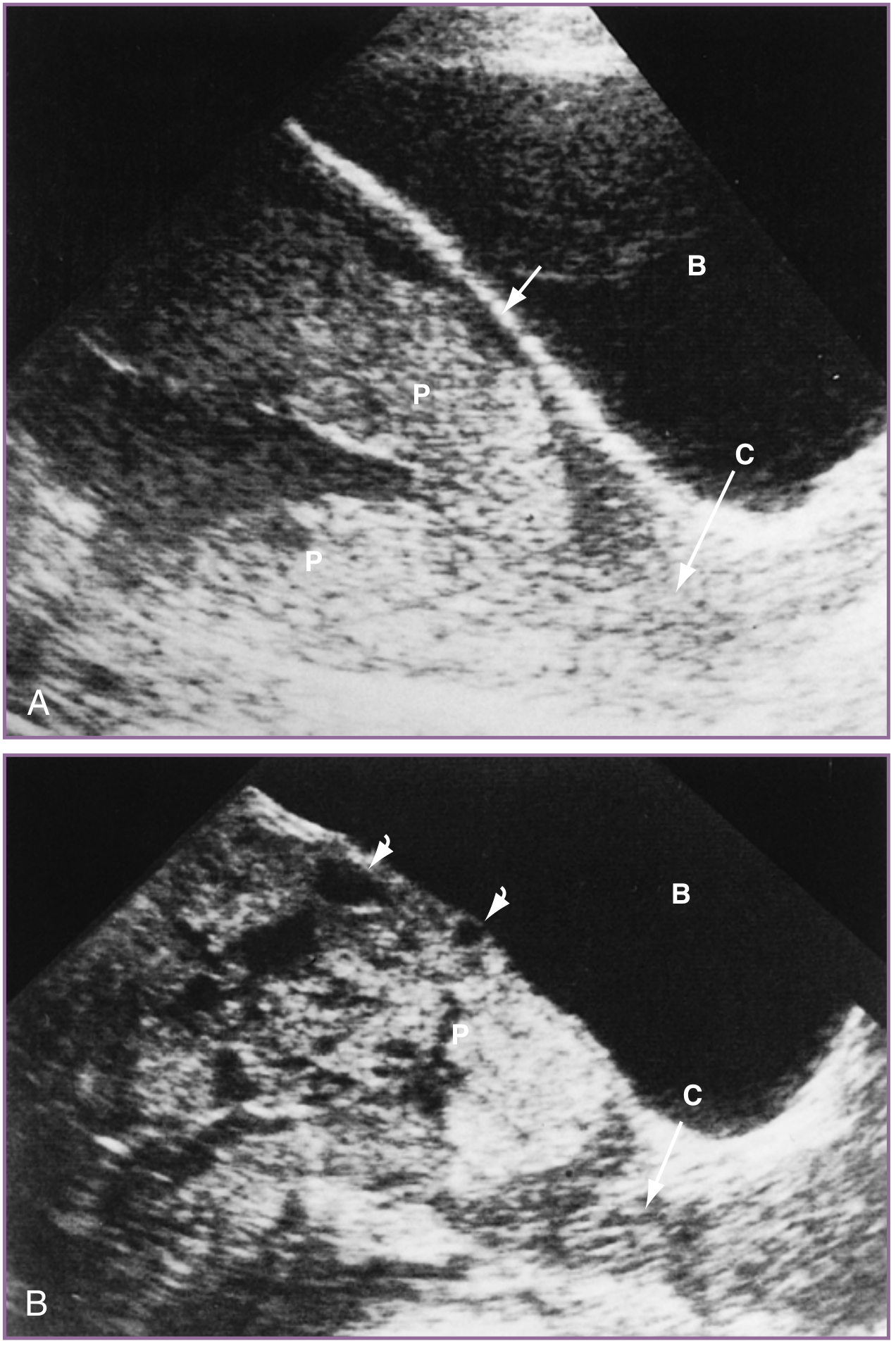
Ultrasound (First-line)
Sensitivity ~80-90% in published studies (though likely an overestimate due to referral bias; blinded expert studies show sensitivity as low as 55%).
Key ultrasound markers:
| Marker | Definition |
|---|---|
| Placental lacunae | Irregular hypoechoic intraplacental spaces with turbulent vascular flow ("Swiss cheese" appearance) |
| Loss of retroplacental hypoechoic zone | Obliteration of the normal myometrial clear space between placenta and bladder |
| Abnormal uterine contour / placental bulge | Placental tissue distorting the uterine contour |
| Bridging vessels | Vessels extending from placenta across myometrium and beyond serosa |
| Exophytic mass | Placental tissue extruding beyond uterine serosa |
| Retroplacental myometrial thinning | Thickness <1 mm |
Color Doppler and power Doppler show turbulent, high-velocity flow in lacunar spaces and increased vascularity at the placenta-uterine interface.
Diagnosis can be made as early as the first trimester, especially in the setting of a cesarean scar ectopic pregnancy.
Ultrasound comparison - normal vs. accreta:
MRI
- Used to confirm diagnosis or delineate extent of invasion.
- Reported high accuracy but prone to referral bias; uncertain benefit over skilled ultrasound.
- Most useful for: posterior placenta, deep myometrial involvement, parametrial/bladder assessment.
- Gadolinium: may improve diagnostic accuracy but associated with risk of rheumatologic/inflammatory conditions and perinatal adverse events in one large Canadian study - use with caution.
Management
Antenatal Planning
- All women with risk factors should be referred to a unit with expertise in PAS diagnosis.
- Diagnosis before delivery is imperative - intraoperative hemorrhage can be massive, and undiagnosed cases carry far higher morbidity.
- Care by a multidisciplinary team at a regional referral center ("center of excellence") markedly reduces maternal morbidity and blood loss.
Timing of Delivery
- Planned elective delivery at 34-35 weeks (range 34-37 weeks in guidelines) after maternal corticosteroid administration.
- Delivery without amniocentesis for fetal lung maturity confirmation given the favorable neonatal outcomes with this approach.
Surgical Management (Preferred)
Cesarean hysterectomy is the standard treatment:
- Delivery via fundal uterine incision (avoiding the placenta)
- Cord is clamped immediately after delivery
- Placenta is left in situ
- Proceed directly to total abdominal hysterectomy
- A pelvic surgeon capable of wide resection of the lower uterine segment and parametrial areas should be available
- Ample transfusion capability required
Balloon occlusion of internal iliac arteries or aorta (via preoperative femoral artery catheterization under fluoroscopy) has been used to reduce blood loss during dissection, but evidence for benefit is inconsistent and embolic complications have been reported - its role remains under study.
Conservative (Uterine-Preserving) Management
May be considered in select cases:
- Suspicion of small focal accreta
- Fundal location (post-myomectomy or classic cesarean)
- Posteriorly implanted placenta
- Strong desire for fertility preservation
Approach: fundal hysterotomy, delivery of baby, placenta left in situ, usually followed by uterine artery embolization postoperatively.
Risks are substantial:
- ~11% require primary hysterectomy for intraoperative hemorrhage
- ~11% require delayed hysterectomy
- Recurrent accreta in subsequent pregnancies
- Methotrexate is not recommended - no proven efficacy and associated with serious complications including one reported death.
- Must be undertaken with extreme caution and full informed consent.
Complications
- Massive obstetric hemorrhage - leading cause of maternal morbidity/mortality
- Emergency peripartum hysterectomy (most common indication)
- Bladder, ureter, bowel injury (especially percreta)
- Preterm birth (iatrogenic)
- Fetal growth restriction
Classification Summary
Placenta Accreta Spectrum (PAS)
├── Accreta → adherent to myometrium, no invasion (82%)
├── Increta → invasion into myometrium (12%)
└── Percreta → invasion through serosa ± adjacent organs (6%)
Also historically called "morbidly adherent placenta" - this older term is still used interchangeably.
Sources: Creasy & Resnik's Maternal-Fetal Medicine, 8th ed., Ch. 27 & 43 | Robbins & Cotran Pathologic Basis of Disease | SMFM Publications Committee (Am J Obstet Gynecol, 2010) | SMFM Placenta Accreta Spectrum Ultrasound Marker Task Force Consensus (Am J Obstet Gynecol, 2021)
This is a shared conversation. Sign in to Orris to start your own chat.