Liver cyst
Reading File
Finding Sources
Searching PubMed
"liver cyst" AND management
Finding Sources
Finding Sources
Searching PubMed
"hepatic cyst" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information. Let me compile the full response.
Liver Cyst
A liver (hepatic) cyst is a fluid-filled cavity within the liver. The term covers a spectrum from common, benign simple cysts to parasitic (hydatid) cysts, polycystic liver disease, and rare cystic neoplasms. Below is a structured review.
Classification / Types
| Type | Cause | Key Features |
|---|---|---|
| Simple (congenital) cyst | Aberrant bile duct development | Most common; benign; solitary or multiple |
| Polycystic liver disease (PLD) | Genetic (PKD1/PKD2 or PRKCSH/SEC63) | Multiple cysts; associated with ADPKD |
| Hydatid cyst | Echinococcus granulosus / E. multilocularis | Parasitic; daughter cysts; eosinophilia |
| Biliary cystadenoma / cystadenocarcinoma | Neoplastic | Complex; thick wall; septal nodules |
| Ciliated hepatic foregut cyst | Congenital | Rare; left lobe; lined by ciliated epithelium |
| Traumatic / hemorrhagic cyst | Blunt trauma, prior abscess | Elevated fluid attenuation on CT |
Simple (Congenital) Hepatic Cyst
Pathogenesis
Simple liver cysts arise from aberrant bile ducts that lack communication with the biliary tree. Serous, non-bilious fluid accumulates in a spherical cavity lined by a single layer of cuboidal or columnar biliary epithelium with a surrounding fibrous stroma.
- Current Surgical Therapy 14e, p. 411
Epidemiology
- Prevalence ~18% of the general population
- Slight female predominance (1.5:1)
- More common in the right lobe
- Usually discovered incidentally in adults
- Current Surgical Therapy 14e, p. 411
Clinical Features
Most are asymptomatic. Large cysts may cause:
- Right upper quadrant pain or fullness
- Early satiety, nausea, vomiting
- Shortness of breath (if large)
- Rare complications: infection, hemorrhage, biliary obstruction, rupture
Liver function tests are typically normal.
Imaging
Ultrasound
The first-line modality. A simple cyst appears as:
- Round, anechoic (echo-free)
- Well-defined margins
- No internal echoes, no perceptible wall
- Posterior acoustic enhancement (bright zone behind the cyst)
- No internal Doppler flow
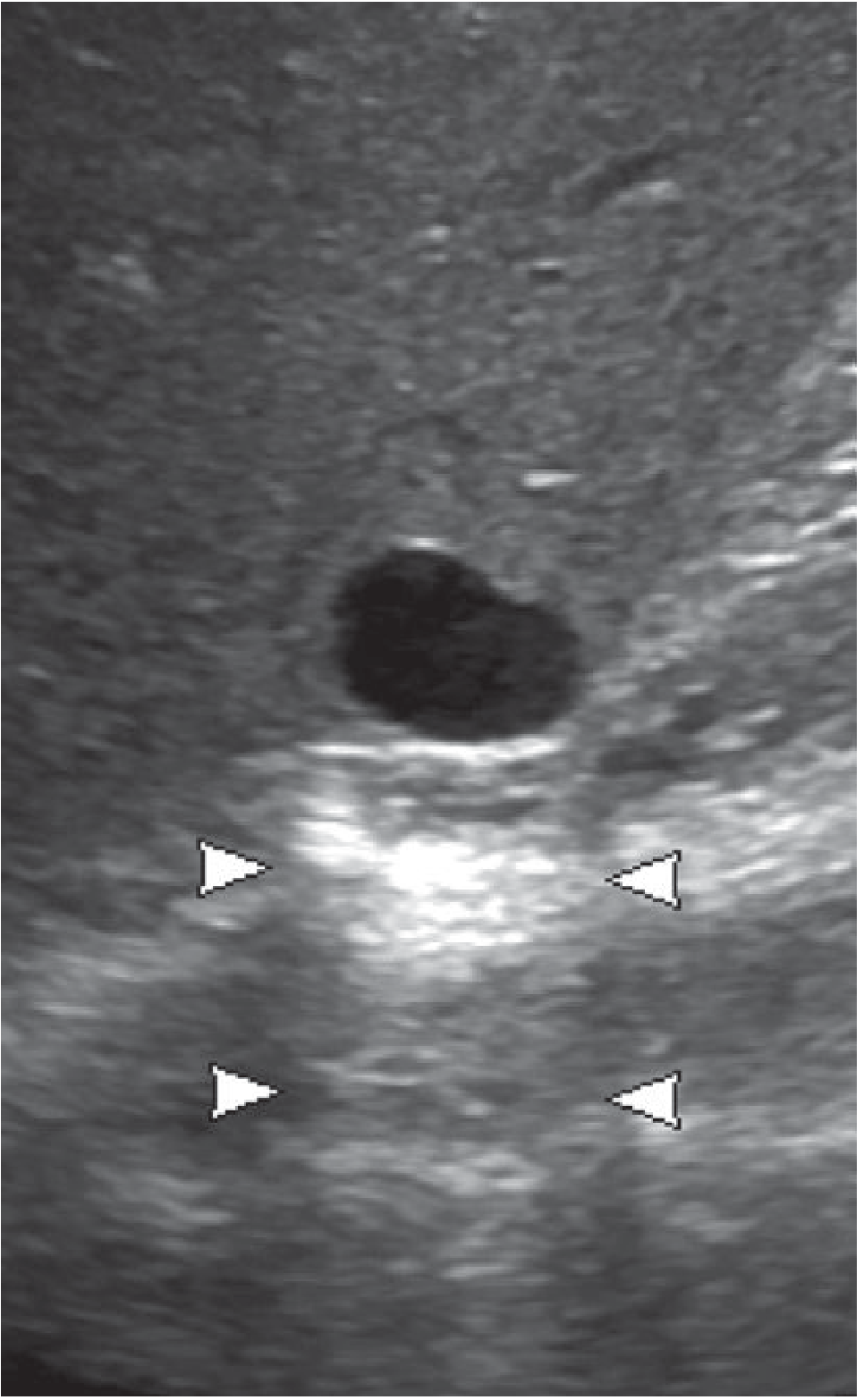
Simple liver cyst on US: anechoic, no wall, posterior acoustic enhancement (arrowheads). - Grainger & Allison's Diagnostic Radiology, p. 632
Prompt further imaging (CT or MRI) if: internal echoes, thick septations, perceptible wall, or solid components are seen.
CT
- Well-circumscribed, homogeneous
- Attenuation 0-10 HU (near water density)
- No enhancement after IV contrast
- Small cysts may have partial volume effects; US can help exclude a solid lesion
MRI
- T1: hypointense (dark)
- T2: very hyperintense (bright) - typically brighter than the spleen, comparable to CSF
- No enhancement with gadolinium
- Heavily T2-weighted sequences (MRCP-like) help separate cysts from hemangiomas
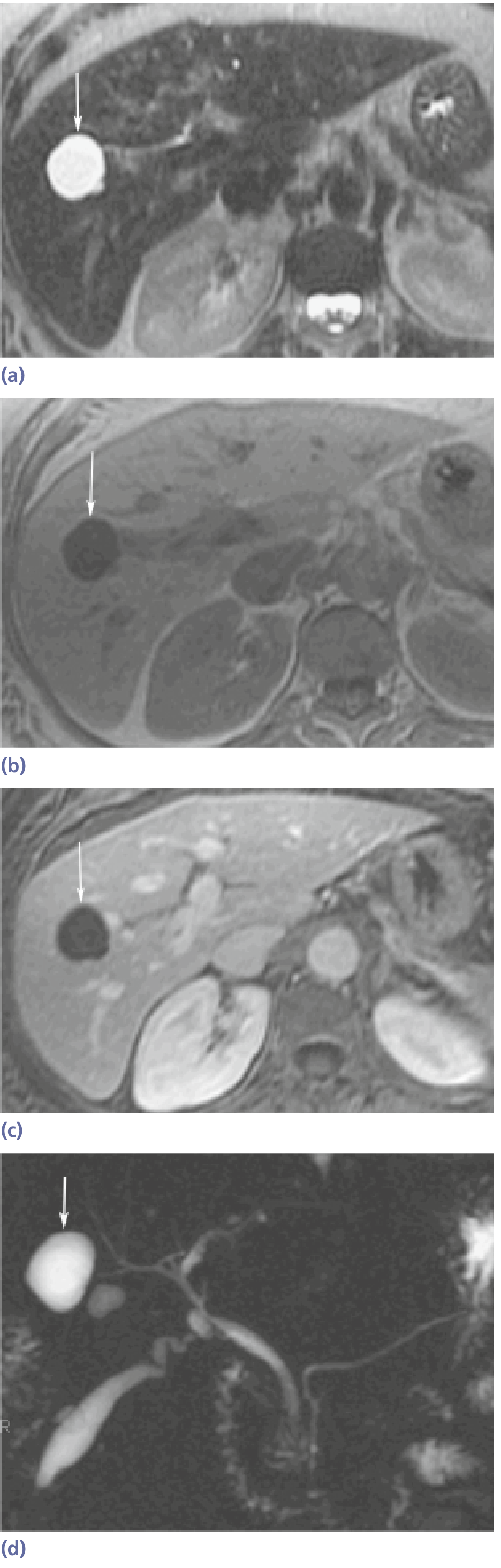
Simple hepatic cyst on MRI - high T2 signal, low T1 signal, no enhancement. - Yamada's Textbook of Gastroenterology, p. 2748
Imaging comparison table (from Current Surgical Therapy 14e):
| Lesion | US | CT | MRI |
|---|---|---|---|
| Simple cyst | Round, anechoic, through-transmission, generally no septations | Well circumscribed, hypoattenuated, limited contrast enhancement | T1 hypointense, T2 very hyperintense, no enhancement |
| Biliary cystadenoma | Anechoic, thick wall, internal septations, may have mural nodules | Mural and nodular enhancement | Heterogeneous, T2 hyperintense, mural/nodular enhancement |
| Hemangioma | Homogeneous, hyperechoic | Asymmetric peripheral pooling → centripetal fill-in | T2 very hyperintense; gadolinium mirrors CT |
Differential Diagnosis of Cystic Liver Lesions
- Simple cyst - most common benign lesion
- Polycystic liver disease - multiple cysts + family history/renal cysts
- Hydatid cyst - daughter cysts, calcified wall, travel/animal exposure
- Biliary cystadenoma - thick wall, septations, mural nodules; pre-malignant
- Biliary cystadenocarcinoma - malignant; irregular enhancement
- Cystic metastasis - ovarian, colorectal, sarcoma primaries
- Hepatic abscess - fever, debris, wall enhancement
- Cystic hemangioma - peripheral nodular enhancement
Management
Simple Cyst
- Asymptomatic, small cysts: No treatment; reassure and observe
- Symptomatic or large cysts (>5-10 cm): Options include:
- Percutaneous aspiration with sclerotherapy (ethanol or tetracycline) - first-line for most symptomatic cysts
- Laparoscopic fenestration (deroofing) - excise the exposed cyst roof; effective with low recurrence
- Open fenestration or resection - reserved for complex cases
- Current Surgical Therapy 14e, p. 411-413
A 2025 clinical practice guideline (Rho et al., Ann Hepatobiliary Pancreat Surg 2025, PMID 40653359) specifically addresses diagnosis, treatment, and prognosis of simple hepatic cysts - the most recent authoritative guidance available.
Hydatid (Echinococcal) Cyst
The most common cause of liver cysts worldwide. In humans, 50-75% of echinococcal cysts involve the liver (right lobe in 80%, single in 75%).
- Maingot's Abdominal Operations
WHO/Gharbi Classification
| Stage | Description |
|---|---|
| CL | Unilocular anechoic cystic lesion without internal echoes or septations |
| CE1 | Uniformly anechoic with fine internal echoes ("hydatid sand") |
| CE2 | Internal septations; multivesicular, honeycomb or rosette formation |
| CE3a | Detached laminated membrane (water-lily sign) |
| CE3b | Daughter cysts inside a solid matrix |
| CE4 | Inactive; no visible daughter cysts; mixed hypo-/hyperechoic pattern ("bag of wool") |
| CE5 | Inactive; partial or complete calcification of the wall |
Bailey and Love's Short Practice of Surgery, 28th ed.
Diagnosis
- Eosinophilia (~35%)
- Serology: ELISA, immunoelectrophoresis
- Imaging: US + CT (first choice); classic findings = calcified thick wall with daughter cysts
- ERCP if biliary communication suspected
Treatment
Treatment should ideally be in a tertiary unit with a multidisciplinary team.
| Approach | Indication |
|---|---|
| Watch and wait | CE4/CE5 (inactive); asymptomatic |
| Albendazole (medical) | Used pre- and post-procedurally in all active cysts |
| PAIR (Puncture-Aspiration-Injection-Re-aspiration) | CE1, CE2; inoperable patients; pregnancy; disseminated disease |
| Pericystectomy / hepatic resection (surgery) | Active cysts; failed PAIR; large/complex cysts; biliary communication |
| Laparoscopic deroofing | CE1/2 accessible cysts in experienced centers |
Scolicidal agents used intraoperatively include hypertonic saline (15-20%) or 5-10% povidone-iodine (risk of sclerosing cholangitis if biliary communication exists).
- Bailey and Love's Short Practice of Surgery, 28th ed., p. 95-96
- Maingot's Abdominal Operations, p. 935-937
Polycystic Liver Disease (PLD)
- Associated with ADPKD (PKD1/PKD2 mutations) or isolated PLD (PRKCSH/SEC63)
- Estrogen receptors on cyst epithelium - cyst growth stimulated by estrogens and IGF-1; hence more severe in women, especially with prior OCP/HRT use
- Treatment for massive PLD: somatostatin analogs (octreotide, lanreotide) reduce cyst growth; fenestration or liver transplantation for extreme cases
- Comprehensive Clinical Nephrology, 7th ed.
Key Clinical Pearls
- A confidently diagnosed simple cyst (all US criteria met) in a patient without ovarian metastases or hydatid exposure requires no further workup.
- Any complexity (septations, wall, echoes, solid nodules) mandates CT or MRI.
- Biliary cystadenoma must be resected (not merely drained) due to malignant potential.
- Hydatid cyst aspiration/biopsy without preparation risks anaphylactic shock from cyst fluid spillage - always give albendazole first and use scolicidal agents.
- On DWI-MRI, cysts show high ADC values (free diffusion) - distinguishing them from solid tumors or abscesses which show restricted diffusion.
This is a shared conversation. Sign in to Orris to start your own chat.