What is the test to check ketone bodies in blood and normal values
Reading File
Finding Sources
Searching the Web
ketone bodies blood test normal values beta-hydroxybutyrate reference range
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete, textbook-grounded answer:
Ketone Bodies in Blood - Tests and Normal Values
The Three Ketone Bodies
There are three ketone bodies produced in the liver from fatty acid oxidation:
- Acetoacetate (primary)
- Beta-hydroxybutyrate (β-OHB) - formed from acetoacetate by β-hydroxybutyrate dehydrogenase
- Acetone - formed by spontaneous decarboxylation of acetoacetate
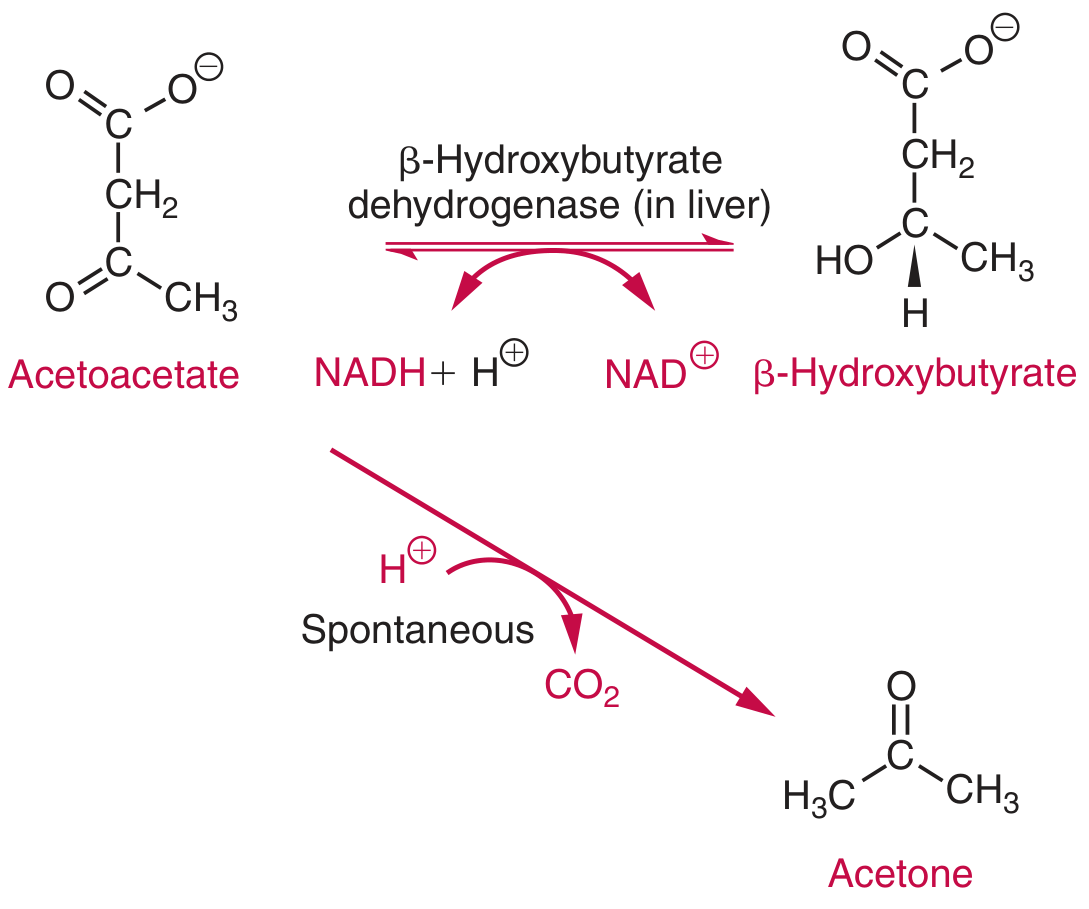
In healthy people, β-hydroxybutyrate and acetoacetate are present at approximately equimolar concentrations and make up virtually all serum ketones. In severe DKA, the β-OHB : acetoacetate ratio can increase up to 6:1 due to high NADH favoring β-OHB production.
Tests for Blood Ketone Bodies
1. Nitroprusside-based Tests (Semi-quantitative)
| Test | Principle | Detects |
|---|---|---|
| AimTab (Rothera's test) | Glycine + sodium nitroprusside forms lavender-purple complex | Acetoacetate (and acetone, less sensitively) |
| Ketostix (reagent strip) | Modified nitroprusside test | Acetoacetate; positive at ≥50 mg/L |
| Gerhardt's ferric chloride test | Ferric chloride reacts with acetoacetate | Acetoacetate only |
Critical limitation: Nitroprusside assays do not react with β-hydroxybutyrate at all. So a negative nitroprusside test does NOT rule out ketoacidosis, especially in severe DKA where β-OHB predominates.
2. Enzymatic Assay for β-Hydroxybutyrate (Quantitative - Preferred)
This is the gold standard test for blood ketones:
- Principle: β-OHB + NAD⁺ → Acetoacetate + NADH (catalyzed by β-hydroxybutyrate dehydrogenase). Diaphorase then reduces nitroblue tetrazolium (NBT) using NADH to form a purple compound measured at 505 nm.
- Specimen: Serum, plasma, or whole blood
- Platforms: Automated chemistry analyzers (Roche, etc.) or handheld point-of-care meters (Precision Xtra, Nova Max Plus)
Normal Values
| Parameter | Normal (Fasting/Fed) | Clinical Interpretation |
|---|---|---|
| Total serum ketones | < 1 mg/dL (< 0.1 mmol/L) | Negative on standard diet |
| β-Hydroxybutyrate (β-OHB) | < 0.4-0.5 mmol/L | Normal fasting range |
| β-OHB on ketogenic diet | ~1 mmol/L (up to 10 mg/dL) | Dietary ketosis, not pathological |
| β-OHB - risk threshold | ≥ 1.5 mmol/L | DKA risk - needs evaluation |
| β-OHB in ketoacidosis | ≥ 3 mmol/L | Diagnostic of ketoacidosis |
| Critical value (DKA) | > 3 mmol/L | Possible critical value |
| Severe DKA | May exceed 25 mmol/L | Life-threatening |
Note: Handheld meters measuring β-OHB are less accurate at concentrations > 3 mmol/L.
Clinical Significance - When Are Ketones Elevated?
- Diabetic ketoacidosis (DKA): glucose > 200 mg/dL + elevated ketones + pH < 7.3
- Alcoholic ketoacidosis (AKA): elevated β-OHB without hyperglycemia
- Starvation/prolonged fasting: after 3-day fast, ketones provide 30-40% of body's energy
- Low-carbohydrate (ketogenic) diets
- Isopropyl alcohol ingestion, salicylate poisoning
- Pregnancy: ~30% of first morning void specimens are ketone-positive
Blood β-OHB measurement is more accurate than urine ketone testing for managing DKA.
Sources: Tietz Textbook of Laboratory Medicine, 7th Ed., p. 1741-1742; Medscape - Ketones Reference Range; EBM Consult - Beta-Hydroxybutyrate Blood Level
What is the significance of ketone bodies in diabetes
Finding Sources
Searching the Web
significance of ketone bodies in diabetes mellitus DKA pathophysiology
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Excellent content gathered. Here is a thorough, textbook-grounded answer:
Significance of Ketone Bodies in Diabetes
1. Why Ketones Form in Diabetes
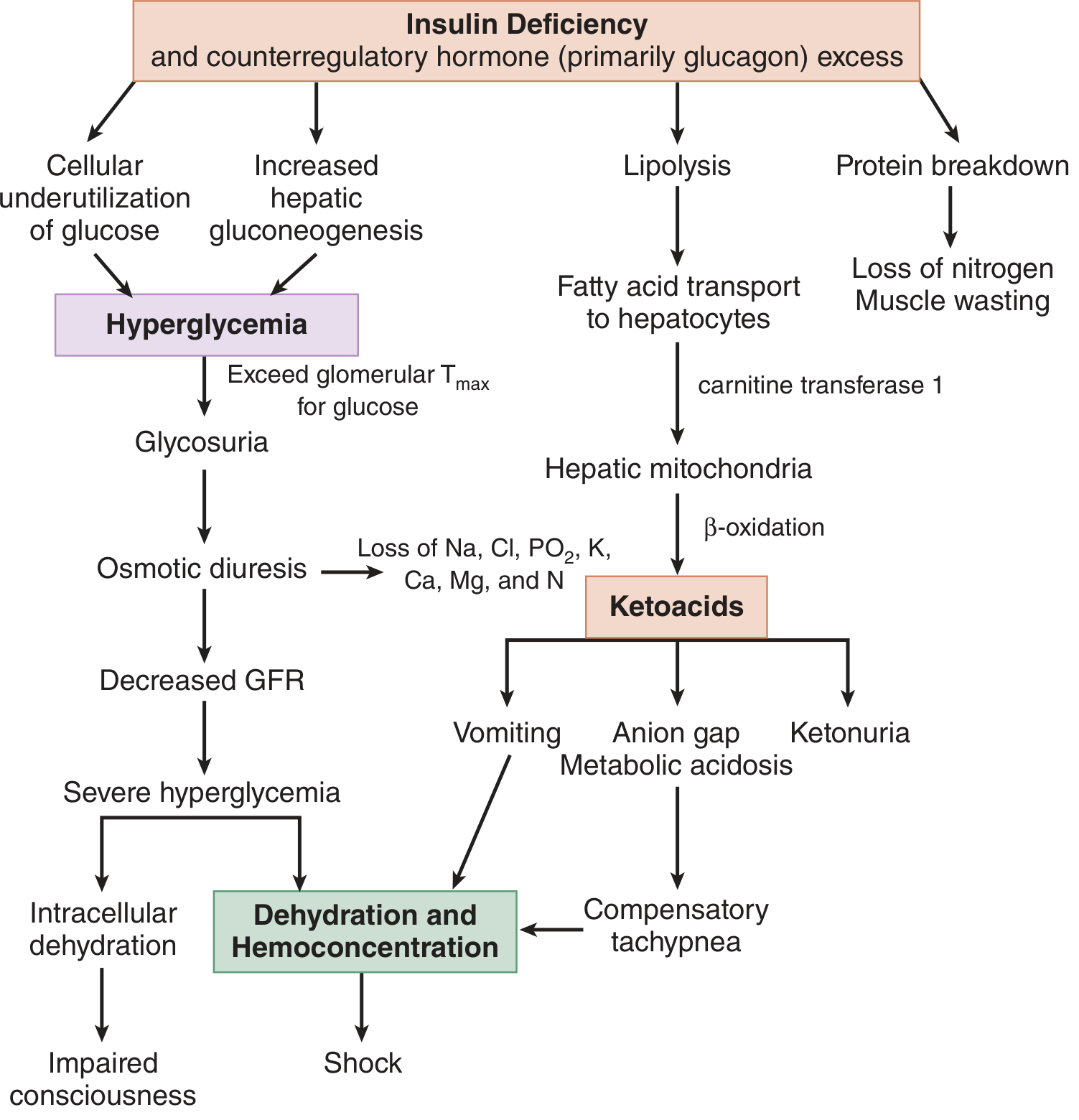
In normal physiology, insulin promotes glucose uptake and inhibits lipolysis. In diabetes - especially Type 1 DM or poorly controlled Type 2 DM - insulin deficiency combined with excess counterregulatory hormones (glucagon, catecholamines, cortisol, growth hormone) triggers a chain of metabolic events:
- Increased lipolysis in adipose tissue → free fatty acids (FFAs) released into blood
- FFAs transported to the liver, enter hepatic mitochondria via carnitine transferase-1
- Beta-oxidation of FFAs → acetyl-CoA → ketone body synthesis (acetoacetate, β-hydroxybutyrate, acetone)
- Simultaneously, low insulin levels reduce peripheral tissue ability to use ketones as fuel → ketonemia builds up
This entire cascade is summarized below:
2. Diabetic Ketoacidosis (DKA) - The Primary Clinical Significance
DKA is the most serious consequence of ketone accumulation in diabetes. It is a life-threatening emergency defined by the triad:
| Parameter | Criterion |
|---|---|
| Blood glucose | > 250 mg/dL (13.9 mmol/L) |
| pH | < 7.3 |
| Serum bicarbonate | < 15 mEq/L |
| Anion gap | > 10-12 mEq/L |
| Ketones | Moderate ketonuria or ketonemia |
Severity Classification
| Grade | pH | Bicarbonate | Consciousness |
|---|---|---|---|
| Mild | 7.25-7.30 | 15-18 mEq/L | Alert |
| Moderate | 7.00-7.24 | 10-15 mEq/L | Alert to drowsy |
| Severe | < 7.00 | < 10 mEq/L | Stuporous to comatose |
Common Precipitating Causes
- Missed or reduced insulin doses (most common)
- Infection (most common external trigger)
- Myocardial infarction, stroke, pancreatitis
- Pregnancy, surgery, major trauma
- Medications: steroids, SGLT2 inhibitors, antipsychotics
- Cocaine abuse
3. Pathophysiological Consequences of Ketosis
The ketone bodies (β-hydroxybutyrate and acetoacetate) are strong organic acids that cause:
- Anion gap metabolic acidosis - β-OHB and acetoacetate dissociate, consuming bicarbonate
- Kussmaul respirations - deep, rapid breathing to compensate for acidosis (blowing off CO₂)
- Fruity breath odor - from acetone exhalation
- Nausea, vomiting, abdominal pain - mediated by prostaglandins I₂ and E₂ released from adipose breakdown
- Osmotic diuresis - from hyperglycemia → loss of Na, K, Cl, PO₄, Ca, Mg in urine → dehydration → shock
- Paradoxical vasodilation despite severe volume depletion (prostaglandin effect)
- Impaired consciousness - correlates with serum osmolality > 320 mOsm/L; multifactorial (acidosis + hyperosmolarity + poor hemodynamics)
- Electrolyte imbalance - especially potassium depletion (total body K⁺ depleted despite possible high serum K⁺ at presentation)
4. Euglycemic DKA - A Diagnostic Trap
A special situation where DKA occurs with blood glucose < 250 mg/dL - easily missed if ketones are not checked:
- Pregnant Type 1 diabetics with vomiting
- Recent insulin administration
- Starvation or low caloric intake
- SGLT2 inhibitor use (canagliflozin, dapagliflozin, empagliflozin): SGLT2 inhibitors increase urinary glucose excretion, lower insulin levels, raise glucagon → ketogenesis despite near-normal blood sugar. β-OHB > 3 mmol/L helps diagnose this.
Key point: SGLT2 inhibitors should be stopped 3-4 days before elective surgery to prevent perioperative euglycemic DKA.
5. Monitoring Significance - Why Ketone Testing Matters in Diabetes
| Clinical Situation | Recommendation |
|---|---|
| Type 1 DM during acute illness/stress | Test ketones |
| Blood glucose consistently > 300 mg/dL | Test ketones |
| Pregnancy with pre-existing diabetes | Test ketones |
| Symptoms of DKA (nausea, vomiting) | Test ketones |
| On SGLT2 inhibitor with any illness | Test ketones |
Blood β-hydroxybutyrate measurement is more accurate than urine ketone strips for monitoring DKA treatment progress (urine ketones can lag behind blood levels).
6. Treatment Priorities in DKA (DRIP mnemonic)
| Priority | Action |
|---|---|
| D - Dehydration correction | 0.9% saline - 1 L bolus, then 500-1000 mL/h |
| R - Regular insulin | 0.1 units/kg bolus → 0.1 units/kg/h infusion; target glucose drop 50-75 mg/dL/h |
| I - Ion (Potassium) repletion | Do NOT start insulin until K⁺ > 3.5 mmol/L; insulin drives K⁺ intracellularly |
| P - Phosphate, Bicarbonate | Not routinely given; consider bicarbonate only if pH < 6.9 |
| Dextrose 5% added | When glucose falls to ~200-250 mg/dL to prevent hypoglycemia while continuing insulin to clear ketones |
Key Takeaway
Ketone bodies in diabetes are markers and mediators of metabolic decompensation. They signal that the body has switched from glucose to fat burning due to insulin lack - and the resulting acid load can be rapidly fatal if untreated. Regular ketone monitoring, especially during illness, is a cornerstone of diabetes self-management.
Sources: Tintinalli's Emergency Medicine (Comprehensive Study Guide), p. 1476-1477; Washington Manual of Medical Therapeutics, p. 890; Medscape - DKA Pathophysiology
This is a shared conversation. Sign in to Orris to start your own chat.