Pedal edema and inflamed knees
pedal edema knee arthritis differential diagnosis
pedal edema inflamed knee joints causes differential diagnosis clinical approach
Pedal Edema + Inflamed Knees: Clinical Approach
Key Pathophysiology of Edema
- Increased hydrostatic pressure - impaired venous return (heart failure, thrombosis, liver cirrhosis)
- Reduced colloid osmotic pressure - hypoproteinemia (nephrotic syndrome, malnutrition, liver disease)
- Lymphatic obstruction - inflammatory, neoplastic, post-surgical
- Sodium retention - renal insufficiency, hyperaldosteronism
- Inflammation - acute or chronic, which causes increased vascular permeability
Differential Diagnosis
1. Polymyalgia Rheumatica (PMR)
"A few patients have pitting edema of the hands or feet (Salvarini and colleagues); others have knee or wrist arthritis or carpal tunnel syndrome."
- Typically in middle-aged to elderly patients (>50 years)
- Severe proximal muscle pain and stiffness (shoulders, hips, neck)
- Markedly elevated ESR (usually >70 mm/h) and CRP
- Normal creatine kinase (unlike polymyositis)
- Often associated with giant cell (temporal) arteritis
- Responds dramatically to low-dose corticosteroids
2. Systemic Lupus Erythematosus (SLE)
"Lupus arthritis is typically characterized by a symmetric, inflammatory arthritis that predominantly affects the knees, wrists, and small joints of the hands."
- Knee involvement in up to 90% of SLE patients at some point
- Pedal edema can arise from lupus nephritis (nephrotic range proteinuria) or hypoproteinemia
- Small synovial effusions, not as inflammatory as RA
- Associated with rash, serositis, renal disease, cytopenias
- ANA, anti-dsDNA antibodies positive
3. Rheumatoid Arthritis (RA)
- Symmetric polyarthritis involving knees, wrists, MCPs, PIPs
- Pedal edema can result from secondary systemic complications: hypoalbuminemia, renal amyloidosis, or heart failure from rheumatoid involvement
- Elevated RF, anti-CCP antibodies
- Erosive changes on imaging
4. Gout / Pseudogout
- Gout typically causes asymmetric, acute monoarthritis (classically the first MTP joint, but the knee is a common site)
- Pedal edema can coexist with tophaceous gout around foot/ankle joints
- Crystal-proven: negatively birefringent needle-shaped monosodium urate crystals (gout) vs. positively birefringent calcium pyrophosphate crystals (pseudogout)
- Elevated serum uric acid supports but is not diagnostic
5. Congestive Heart Failure (CHF)
- Bilateral dependent pitting pedal edema with elevated JVP is a hallmark, as noted in Harrison's Principles of Internal Medicine
- Joints can develop secondary inflammatory changes (e.g., due to restricted mobility, DVT, or co-existing arthritis)
- However, true knee arthritis is NOT a feature of CHF itself - arthritis in this setting means a co-existing condition
6. Reactive Arthritis (formerly Reiter Syndrome)
- Triggered by a preceding infection (genitourinary or enteric)
- Asymmetric oligoarthritis of large joints including the knee
- Lower limb edema may arise from associated periostitis or enthesitis
- Classic triad: arthritis + urethritis + uveitis
- HLA-B27 associated
7. Nephrotic Syndrome
- Bilateral pedal edema from severe hypoproteinemia (hypoalbuminemia)
- Arthritis is NOT a primary feature, but can co-exist (e.g., SLE-related nephritis causing both)
- Frothy urine, heavy proteinuria (>3.5 g/day), hypoalbuminemia, hyperlipidemia
8. Septic Arthritis
- Medical emergency - acute red, hot, extremely painful single joint (often the knee)
- Pedal edema in this setting would suggest sepsis-related capillary leak or coexisting condition
- Fever, elevated WBC, synovial fluid WBC >50,000 cells/µL
- Requires urgent joint aspiration and IV antibiotics
Approach to Evaluation
| Investigation | What it rules in/out |
|---|---|
| ESR, CRP | Inflammation (very high in PMR, moderate in RA/SLE) |
| CBC | Anemia of chronic disease, cytopenias in SLE |
| Serum albumin | Hypoproteinemia as cause of edema |
| Urine protein/creatinine ratio | Nephrotic syndrome |
| RF, anti-CCP | Rheumatoid arthritis |
| ANA, anti-dsDNA, complement | SLE |
| Uric acid | Gout (elevated, but not diagnostic alone) |
| Echocardiogram | Heart failure |
| Synovial fluid aspiration | Cell count, crystals, culture - key for gout vs. septic vs. inflammatory |
| Knee X-ray | Erosions (RA), chondrocalcinosis (pseudogout), joint space loss |
Red Flags Requiring Urgent Assessment
- Fever + single hot swollen knee - septic arthritis until proven otherwise
- Acute unilateral leg edema + knee pain - consider DVT with hemarthrosis
- Elevated JVP + bilateral pedal edema + dyspnea - heart failure
- Temporal headache + jaw claudication + PMR features - giant cell arteritis (risk of blindness)
- Adams and Victor's Principles of Neurology, 12th Ed., p. 237 - PMR causing pitting pedal edema and knee arthritis
- Robbins & Kumar Basic Pathology - Causes of edema (Table 3.1) and pathophysiology
- Firestein & Kelley's Textbook of Rheumatology - SLE arthritis
- Harrison's Principles of Internal Medicine, 22E - Heart failure and lower extremity edema
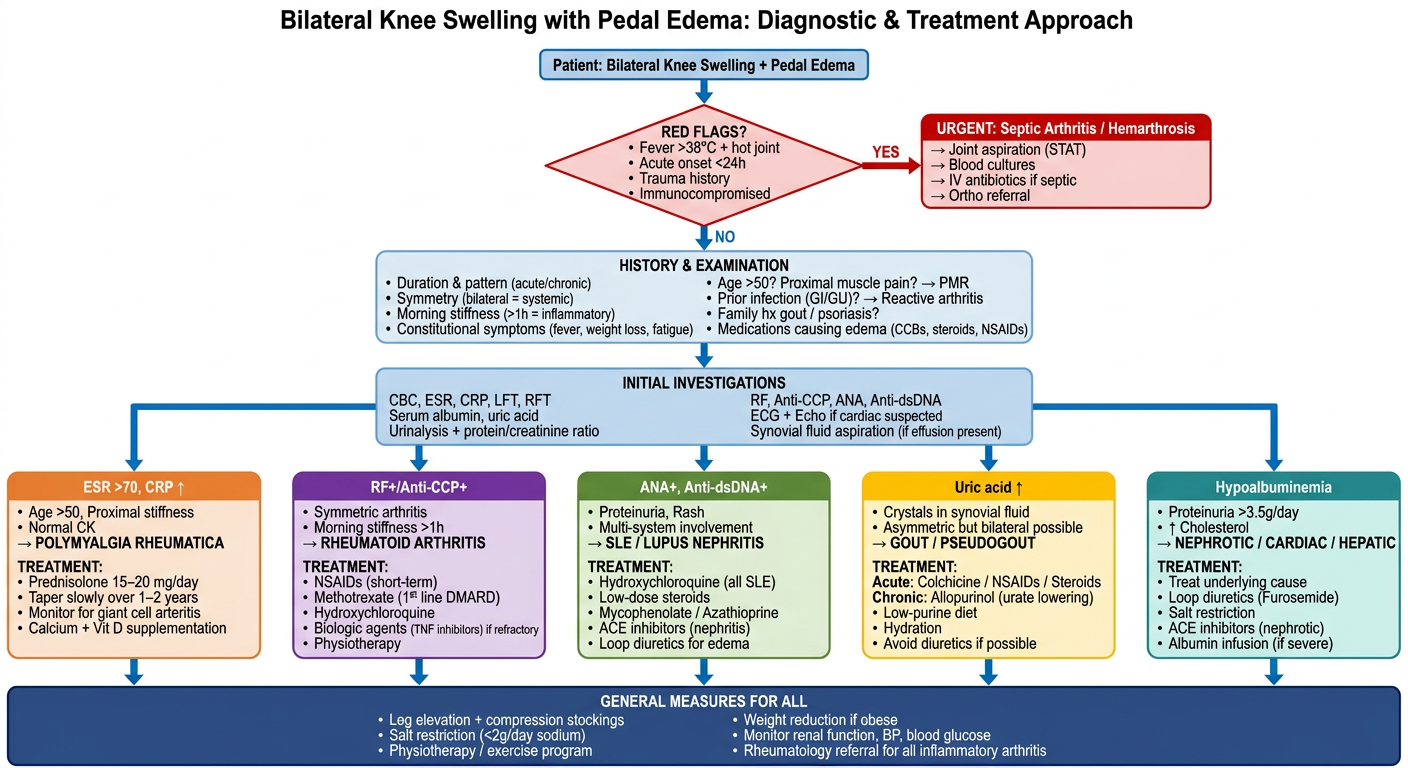
Generate a clinical flowchart for approaching bilateral knee swelling with pedal edema and treatment
A detailed clinical flowchart titled "Bilateral Knee Swelling with Pedal Edema: Diagnostic & Treatment Approach". The flowchart should be clean, professional, medical-grade, with color-coded decision boxes, on a white background. FLOWCHART STRUCTURE (top to bottom): START BOX (blue, top center): "Patient: Bilateral Knee Swelling + Pedal Edema" ↓ FIRST DECISION DIAMOND (red): "RED FLAGS? • Fever >38°C + hot joint • Acute onset <24h • Trauma history • Immunocompromised" YES → RED EMERGENCY BOX (red): "URGENT: Septic Arthritis / Hemarthrosis → Joint aspiration (STAT) → Blood cultures → IV antibiotics if septic → Ortho referral" NO ↓ BOX (light blue): "HISTORY & EXAMINATION • Duration & pattern (acute/chronic) • Symmetry (bilateral = systemic) • Morning stiffness (>1h = inflammatory) • Constitutional symptoms (fever, weight loss, fatigue) • Age >50? Proximal muscle pain? → PMR • Prior infection (GI/GU)? → Reactive arthritis • Family hx gout / psoriasis? • Medications causing edema (CCBs, steroids, NSAIDs)" ↓ BOX (light blue): "INITIAL INVESTIGATIONS CBC, ESR, CRP, LFT, RFT Serum albumin, uric acid Urinalysis + protein/creatinine ratio RF, Anti-CCP, ANA, Anti-dsDNA X-ray both knees ECG + Echo if cardiac suspected Synovial fluid aspiration (if effusion present)" ↓ BRANCHING into 5 parallel columns: COLUMN 1 - ORANGE BOX: "ESR >70, CRP ↑ Age >50, Proximal stiffness Normal CK → POLYMYALGIA RHEUMATICA TREATMENT: • Prednisolone 15–20 mg/day • Taper slowly over 1–2 years • Monitor for giant cell arteritis • Calcium + Vit D supplementation" COLUMN 2 - PURPLE BOX: "RF+/Anti-CCP+ Symmetric arthritis Morning stiffness >1h → RHEUMATOID ARTHRITIS TREATMENT: • NSAIDs (short-term) • Methotrexate (1st line DMARD) • Hydroxychloroquine • Biologic agents (TNF inhibitors) if refractory • Physiotherapy" COLUMN 3 - GREEN BOX: "ANA+, Anti-dsDNA+ Proteinuria, Rash Multi-system involvement → SLE / LUPUS NEPHRITIS TREATMENT: • Hydroxychloroquine (all SLE) • Low-dose steroids • Mycophenolate / Azathioprine • ACE inhibitors (nephritis) • Loop diuretics for edema" COLUMN 4 - YELLOW BOX: "Uric acid ↑ Crystals in synovial fluid Asymmetric but bilateral possible → GOUT / PSEUDOGOUT TREATMENT: Acute: Colchicine / NSAIDs / Steroids Chronic: Allopurinol (urate lowering) • Low-purine diet • Hydration • Avoid diuretics if possible" COLUMN 5 - TEAL BOX: "Hypoalbuminemia Proteinuria >3.5g/day ↑ Cholesterol → NEPHROTIC / CARDIAC / HEPATIC TREATMENT: • Treat underlying cause • Loop diuretics (Furosemide) • Salt restriction • ACE inhibitors (nephrotic) • Albumin infusion (if severe)" ↓ (all columns merge) BOTTOM BOX (dark blue): "GENERAL MEASURES FOR ALL • Leg elevation + compression stockings • Salt restriction (<2g/day sodium) • Physiotherapy / exercise program • Weight reduction if obese • Monitor renal function, BP, blood glucose • Rheumatology referral for all inflammatory arthritis" The flowchart should use clean arrows connecting each box, readable fonts, and distinct colors per branch. Professional medical diagram style.
Flowchart Summary - Key Decision Points
Step 1: Rule Out Emergencies First
- Fever + acute hot joint - septic arthritis (requires same-day joint aspiration + IV antibiotics)
- Trauma history - hemarthrosis/ligament injury
- Immunocompromised - lower threshold for infection
Step 2: History & Exam Clues
| Feature | Points Toward |
|---|---|
| Age >50 + proximal stiffness + ESR >70 | Polymyalgia Rheumatica |
| Morning stiffness >1h + symmetric | RA or SLE |
| Prior GI/GU infection | Reactive arthritis |
| Frothy urine + severe edema | Nephrotic syndrome |
| Dyspnea + elevated JVP | Heart failure |
| Recurrent acute attacks + high uric acid | Gout |
Step 3: Treatment by Diagnosis
| Diagnosis | First-Line Treatment |
|---|---|
| PMR | Prednisolone 15-20 mg/day; taper over 1-2 years |
| Rheumatoid Arthritis | Methotrexate (first-line DMARD) - confirmed by Goldman-Cecil Medicine |
| SLE/Lupus nephritis | Hydroxychloroquine + immunosuppressants (mycophenolate/azathioprine) |
| Gout (acute) | Colchicine / NSAIDs / short-course steroids |
| Gout (chronic) | Allopurinol (urate-lowering therapy) |
| Cardiac/Hepatic/Renal edema | Loop diuretics (furosemide) + treat underlying cause |
General Measures for All Patients
- Leg elevation and compression stockings
- Salt restriction (<2 g sodium/day)
- Physiotherapy and weight reduction
- Rheumatology referral for confirmed inflammatory arthritis