Describe in detail abt undernutrition from pediatrics and community medicine based
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive content from both Park's Preventive & Social Medicine (community medicine) and Robbins' Pathologic Basis of Disease (pathology/pediatrics). I have enough to write a detailed, well-organized answer. Let me compile it now.
Undernutrition - A Detailed Overview (Pediatrics & Community Medicine)
Sources: Park's Textbook of Preventive and Social Medicine; Robbins, Cotran & Kumar - Pathologic Basis of Disease; Robbins & Kumar Basic Pathology
1. Definition and Scope
Undernutrition is a state in which the supply of energy and/or nutrients is insufficient to meet the body's demands for growth, maintenance, and specific functions. In children, undernutrition is synonymous with growth failure - undernourished children are shorter and lighter than expected for their age/height. The term encompasses:
- Stunting (chronic malnutrition)
- Wasting (acute malnutrition)
- Underweight (composite of both)
At the population level, India faces a large burden: per NFHS-4, 35.7% of under-5 children are underweight, 38.4% are stunted, and 21% are wasted.
- Park's Textbook of Preventive and Social Medicine, p.735
2. Classification of Undernutrition
A. By Anthropometric Indicator (WHO Z-score system)
Each of the three nutritional indicators is expressed in standard deviation units (Z-scores) from the WHO Child Growth Standards median:
| Condition | Indicator | Moderate | Severe |
|---|---|---|---|
| Underweight | Weight-for-Age (WFA) | -2 to -3 SD | < -3 SD |
| Stunting | Height-for-Age (HFA) | -2 to -3 SD | < -3 SD |
| Wasting | Weight-for-Height (WFH) | -2 to -3 SD | < -3 SD |
B. By Form (Clinical Types)
- Marasmus - total calorie + protein deficiency
- Kwashiorkor - predominantly protein deficiency with adequate or near-adequate energy
- Marasmic kwashiorkor - combined features
3. Epidemiology and Public Health Burden (Community Medicine)
Undernutrition is a major nutritional problem in public health - not only causing childhood morbidity and mortality, but also permanently impairing physical and possibly mental development in survivors.
- Rural poor and urban slum populations are disproportionately affected
- Protein-energy malnutrition (PEM) and micronutrient deficiencies are the predominant forms
- ~33% of adult men and 36% of adult women in India have BMI < 18.5, indicating chronic energy deficiency; among tribal adults, this rises to 40% (men) and 49% (women)
- Park's Textbook of Preventive and Social Medicine, p.735
4. Etiology and Web of Causation
Primary Causes
- Food gap - inadequate intake of food in both quantity and quality (the modern view has shifted from the older "protein gap" theory)
- Infections - diarrhoea, respiratory infections, measles, and intestinal worms increase calorie/protein requirements while decreasing absorption
The Malnutrition-Infection Vicious Cycle
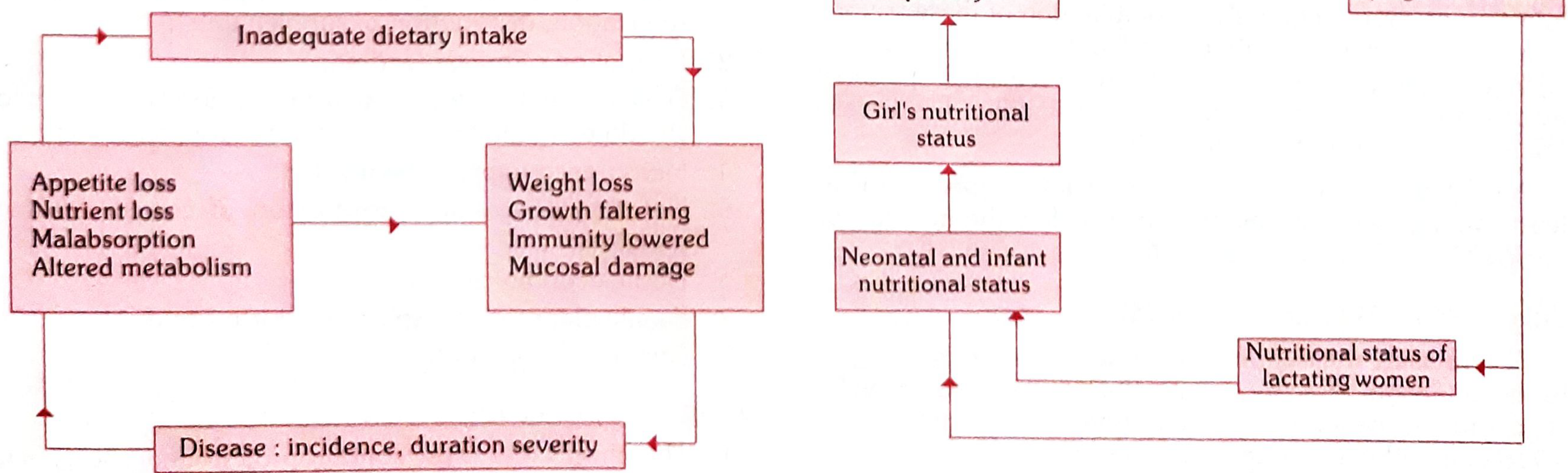
Fig: Malnutrition/Infection Cycle (Park's Textbook p.736)
Other Contributing Factors
- Poor environmental conditions and sanitation
- Large family size; close birth intervals
- Poor maternal health, anaemia, short stature
- Premature termination of breastfeeding
- Over-diluted cow's milk; discarding cereal cooking water
- Delayed or inadequate supplementary feeding
- Adverse cultural/child-rearing practices
Self-Perpetuating Cycle across Generations
Malnutrition is inter-generational: a malnourished girl grows into a malnourished mother who delivers a low birth weight baby, continuing the cycle.
5. Types of Undernutrition in Detail
A. Underweight
- Based on Weight-for-Age (WFA)
- A composite measure of both stunting and wasting
- Recommended indicator for tracking changes in malnutrition over time
- Even mild underweight increases mortality risk; severely underweight children are at even greater risk
- Defined as WFA Z-score < -2 SD from WHO median
B. Stunting
- Based on Height-for-Age (HFA)
- Failure to achieve expected height compared to healthy, well-nourished children of the same age
- Indicator of past/chronic growth failure
- Results from: chronic insufficient nutrient intake, frequent infections, sustained inappropriate feeding practices, and poverty
- Associated with delayed psychosocial and cognitive development, poor school performance
- Defined as HFA Z-score < -2 SD
C. Wasting
- Based on Weight-for-Height (WFH)
- Represents recent/acute failure to receive adequate nutrition
- May be triggered by recent diarrhoea or acute illness
- Shows marked seasonal patterns (changes in food availability, disease prevalence)
- Defined as WHZ-score < -2 SD
D. Severe Acute Malnutrition (SAM)
Diagnostic criteria (any one):
- WHZ < -3 SD
- Mid-upper arm circumference (MUAC) < 115 mm
- Presence of bilateral pitting oedema of the lower limbs
SAM significantly increases the risk of child death. Children who are severely wasted are 9 times more likely to die than well-nourished children. Globally (2022), ~45 million children under 5 were wasted; 13.6 million had SAM.
- Robbins, Cotran & Kumar, p.412
6. Kwashiorkor vs. Marasmus - Clinical Comparison

Fig. 9.20: (A) Marasmus - note loss of muscle and subcutaneous fat, head appears large for emaciated body. (B) Kwashiorkor - generalized oedema with ascites and puffiness of face, hands, and legs. (Robbins & Kumar, p.412)
| Feature | Kwashiorkor | Marasmus |
|---|---|---|
| Primary deficiency | Protein (with relatively adequate energy) | Both protein AND calories |
| Body weight | 60-80% of normal (edema masks true loss) | Severely reduced; severe cachexia |
| Oedema | Present (generalized/dependent - from hypoalbuminaemia) | Absent (or minimal) |
| Subcutaneous fat | Relatively spared | Severely depleted |
| Muscle mass | Relatively spared | Severely wasted |
| Skin changes | "Flaky paint" appearance - alternating zones of hyperpigmentation, desquamation, hypopigmentation | Loose, wrinkled skin |
| Hair changes | Loss of color, alternating light/dark bands, straightening, fine texture, easily pluckable | Sparse, thin |
| Liver | Enlarged, fatty (reduced apolipoprotein synthesis) | Normal |
| Affect | Apathy, listlessness, anorexia | Alert but irritable |
| Serum albumin | Markedly low | May be near normal |
| Typical age | Post-weaning toddler (~1-3 years) | Infancy |
- Park's Textbook of Preventive and Social Medicine, p.736
- Robbins, Cotran & Kumar, p.412-413
7. Pathology / Morphology (SAM)
From Robbins' Pathologic Basis of Disease:
Main anatomic changes in SAM:
- Growth failure
- Peripheral oedema - in kwashiorkor (from hypoalbuminaemia)
- Loss of body fat and muscle atrophy - more marked in marasmus
Organ-specific changes:
-
Liver (in kwashiorkor only): Enlarged and fatty due to reduced synthesis of carrier proteins (apolipoproteins) needed for VLDL assembly; superimposed cirrhosis is rare
-
Small bowel (kwashiorkor > marasmus): Decreased mitotic cells in crypts, mucosal atrophy, loss of villi and microvilli, disaccharidase deficiency (esp. lactase) - children may not initially tolerate full-strength milk-based diets; reversible with treatment
-
Bone marrow: Hypoplastic - decreased red cell precursors leading to mild-moderate anaemia (multifactorial: iron, folate, protein deficiency + anaemia of chronic inflammation from infections)
-
Brain (if SAM occurs in first 1-2 years): Cerebral atrophy, reduced neuron numbers, impaired myelination of white matter - long-term neurocognitive consequences
-
Thymus and lymphoid tissue: Atrophy (more marked in kwashiorkor) - contributes to immune suppression
-
Immunity: Defects in cell-mediated immunity; susceptibility to infections (parasitic, bacterial, viral) further worsens malnutrition
-
Robbins, Cotran & Kumar, p.413
8. Measurement and Early Detection
Anthropometric Indices
- Weight-for-Age (WFA) - most practical; growth chart monitoring
- Height/Length-for-Age (HFA) - detects stunting
- Weight-for-Height (WFH) - detects wasting
Mid-Upper Arm Circumference (MUAC)
Reliable proxy for muscle mass; usable from age 1-5 years (minimal change in this age group):
-
13.5 cm: Satisfactory nutritional status
- 12.5 - 13.5 cm: Mild to moderate malnutrition
- < 12.5 cm: Severe malnutrition
- < 11.5 cm: SAM (WHO criterion)
Growth Charts
The most practical field tool - detects a lag in weight gain before clinical signs appear. Can be used by frontline health workers.
9. Prevention and Control (Community Medicine - FAO/WHO Framework)
(a) Health Promotion
- Education and dietary supplements for pregnant and lactating women
- Promotion of exclusive breastfeeding
- Development of low-cost, nutritious weaning foods; frequent small feeds
- Measures to improve family diet
- Nutrition education - promotion of correct feeding practices
- Home economics and food hygiene training
- Family planning and birth spacing
- Improvement of family environment
(b) Specific Protection
- Protein- and energy-rich foods in the child's diet (milk, eggs, fresh fruits)
- Immunization (prevents infections that trigger malnutrition)
- Food fortification (e.g., vitamin A in dalda/oil, iodine in salt)
(c) Early Diagnosis and Treatment
- Periodic nutritional surveillance
- Early identification of growth faltering (via growth charts)
- Early diagnosis and treatment of diarrhoea and infections
- Oral rehydration programmes
- Supplementary feeding during epidemics
- Deworming of heavily infested children
(d) Rehabilitation
- Nutritional rehabilitation services (NRC - Nutrition Rehabilitation Centres)
- Hospital treatment for SAM with complications
- Follow-up care post-discharge
- Park's Textbook of Preventive and Social Medicine, p.737
10. National Programs (India - Community Medicine Context)
Key government programs addressing undernutrition:
- ICDS (Integrated Child Development Services) - supplementary nutrition, health check-ups, growth monitoring, pre-school education
- NHM (National Health Mission) - nutrition rehabilitation centres (NRCs) for SAM management
- MAA Programme - promotes breastfeeding
- POSHAN Abhiyan (National Nutrition Mission) - comprehensive nutrition strategy targeting stunting, wasting, underweight, and anaemia in children under 6, adolescent girls, and pregnant/lactating women
- Mid-Day Meal Scheme - addresses school-age undernutrition
11. Summary: Key Points to Remember
| Point | Detail |
|---|---|
| SAM definition | WHZ < -3 SD OR MUAC < 115 mm OR bilateral pitting oedema |
| Kwashiorkor hallmark | Oedema + hypoalbuminaemia + fatty liver + "flaky paint" skin |
| Marasmus hallmark | Severe wasting, loose skin, "old man" face, NO oedema |
| Stunting | Chronic (past) malnutrition; HFA < -2 SD |
| Wasting | Acute (current) malnutrition; WHZ < -2 SD |
| Severely wasted mortality risk | 9x higher than well-nourished children |
| MUAC for SAM | < 11.5 cm |
| Malnutrition-infection | Vicious cycle - each perpetuates the other |
| Brain impact | First 1-2 years of life most critical for neurodevelopment |
| Generational | Malnourished girl → malnourished mother → LBW baby |
References:
- Park's Textbook of Preventive and Social Medicine (Nutritional Problems in Public Health, pp.735-737)
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, Nutritional Disease chapter, pp.411-413
- Robbins & Kumar Basic Pathology - SAM morphology section
Define malnutrition and classify protein energy malnutrition describe causes and clinical features of severe forms of malnutrition. Explain preventive measures to reduce protein energy malnutrition in India.
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a thorough, exam-quality answer. Here it is:
Protein-Energy Malnutrition (PEM): Definition, Classification, Causes, Clinical Features, and Prevention in India
Sources: Park's Textbook of Preventive and Social Medicine; Robbins, Cotran & Kumar - Pathologic Basis of Disease; Sleisenger and Fordtran's Gastrointestinal and Liver Disease
1. Definition of Malnutrition
Malnutrition is a broad term that refers to deficiencies, excesses, or imbalances in a person's intake of energy and/or nutrients. It encompasses:
- Undernutrition - insufficient intake of calories, protein, or micronutrients
- Overnutrition - excess intake leading to overweight/obesity
- Micronutrient malnutrition - specific vitamin or mineral deficiencies
Protein-Energy Malnutrition (PEM) is defined as a range of pathological conditions arising from coincident lack, in varying proportions, of protein and calories, occurring most frequently in infants and young children, and commonly associated with infections.
Per UNICEF/WHO/World Bank, malnutrition is "a life-threatening wasting disorder of children caused by poor nutrient intake and/or recurrent illnesses."
- Robbins, Cotran & Kumar, p.412
2. Classification of PEM
A. By Etiology
| Type | Description |
|---|---|
| Primary PEM | Inadequate intake of protein, calories, or both; or ingestion of protein with poor essential amino acid content |
| Secondary PEM | Due to illness or injury - increases metabolic demands, impairs digestion/absorption, induces anorexia |
In practice, both often coexist - illness triggers anorexia and catabolism while the child is already on a deficient diet.
- Sleisenger and Fordtran's, p.86
B. By Waterlow Classification (based on anthropometry)
The Waterlow classification uses two parameters:
Weight-for-Height (Wasting) and Height-for-Age (Stunting):
| Degree | Wasting (Wt/Ht % of median) | Stunting (Ht/Age % of median) |
|---|---|---|
| Normal | 90-100% | 95-105% |
| Mild | 80-89% | 90-94% |
| Moderate | 70-79% | 85-89% |
| Severe | < 70% | < 85% |
(NCHS standards; Z-score equivalent: severe = < -3 Z)
- Sleisenger and Fordtran's, Table 5.16, p.87
C. By Clinical Type (Three Major Syndromes in Children)
| Parameter | Kwashiorkor | Marasmus | Nutritional Dwarfism |
|---|---|---|---|
| Appetite | Poor | Good | Good |
| Oedema | Present | Absent | Absent |
| Mood | Apathetic alone; irritable when held | Alert | Alert |
| Weight-for-age | 60-80% | < 60% | < 60% |
| Weight-for-height | Normal or decreased | Markedly decreased | Normal |
| Serum albumin | Markedly low | Normal or near-normal | Normal |
- Sleisenger and Fordtran's, Table 5.17, p.87
D. By WHO/SAM Criteria
Severe Acute Malnutrition (SAM) is defined by any one of:
- Weight-for-height Z-score < -3 SD
- MUAC (Mid-Upper Arm Circumference) < 115 mm
- Bilateral pitting oedema of lower limbs
3. Causes of PEM
Primary/Direct Causes
- Food gap - inadequate dietary intake in quantity and quality (the concept has evolved from the older "protein gap" to a "food gap")
- Infections - diarrhoea, respiratory infections, measles, and intestinal worms:
- Increase caloric and protein requirements
- Decrease absorption and utilization
- Cause anorexia and increased catabolism
- This creates a vicious cycle where infection worsens malnutrition and malnutrition worsens susceptibility to infection
Contributory/Indirect Causes (Park's Community Medicine framework)
- Socioeconomic: Poverty, food insecurity, crop failures, drought, political upheaval
- Maternal factors: Poor maternal health, malnutrition, anaemia, short stature
- Feeding practices: Premature termination of breastfeeding, use of over-diluted cow's milk, delayed supplementary feeding, discarding cooking water from cereals (which contains nutrients)
- Family factors: Large family size, close birth intervals, poor family environment
- Environmental: Poor sanitation, contaminated water, high infection burden
- Cultural/behavioural: Adverse child-rearing practices, food taboos, ignorance about nutrition
- Self-perpetuating cycle: A malnourished mother delivers a low birth weight infant, who grows up malnourished
"Malnutrition is self-perpetuating. A child's nutritional status at any point of time depends on his or her past nutritional history, which in turn is linked to the mother's health and nutritional status."
- Park's Textbook of Preventive and Social Medicine, p.735
4. Clinical Features of Severe Forms
A. Marasmus (Severe Calorie + Protein Deficiency)
Fig: (A) Marasmus - emaciation with prominent ribs and bones. (B) Kwashiorkor - generalised oedema. (Robbins & Kumar)
Pathophysiology: Dietary calorie deficit leads to catabolism of both the somatic protein compartment (skeletal muscle) and subcutaneous fat, while the visceral protein compartment (liver proteins, albumin) is relatively spared as an adaptive mechanism.
Clinical Features:
- Weight: Falls to < 60% of expected for age, sex, and height
- Appearance: Severe growth retardation; the child looks like a "little old man"
- Muscle wasting: Marked loss of skeletal muscle; extremities are emaciated
- Subcutaneous fat: Severely depleted; skin hangs in loose folds
- Face: Drawn, wizened (old man face); head appears disproportionately large
- Oedema: Absent
- Appetite: Preserved or even increased ("ravenous hunger")
- Mood: Alert, though weak
- Skin: Thin, wrinkled, loose-hanging; no flaky paint changes
- Hair: Sparse, thin
- Serum albumin: Normal or near-normal (visceral protein spared)
- Liver: Not enlarged or fatty
- Anaemia: Present (multifactorial)
- Immunity: Impaired T-cell-mediated immunity; concurrent infections common
B. Kwashiorkor (Predominantly Protein Deficiency)
Pathophysiology: Protein deprivation > calorie deficiency. The visceral protein compartment (serum albumin, transport proteins) is severely depleted, causing hypoalbuminaemia and consequent leaky cell membranes, causing water shift into extracellular space → oedema. The somatic compartment (muscle, fat) is relatively spared.
Clinical Features:
General:
- Weight: 60-80% of expected (true tissue loss masked by oedema)
- Usually occurs after weaning (age 1-3 years); often precipitated by a superimposed infection
Oedema (hallmark):
- Bilateral pitting oedema of lower limbs, face, and hands
- Protuberant abdomen from weakened abdominal muscles, intestinal distension, and hepatomegaly (ascites is rare; its presence should prompt investigation for liver disease)
Skin changes ("flaky paint" dermatosis):
- Alternating zones of hyperpigmentation, desquamation, and hypopigmentation
- Peeling, cracking skin resembling flaking paint
Hair changes:
- Loss of pigmentation (flag sign - alternating pale and darker bands)
- Hair straightening, fine texture
- Loss of firm attachment to scalp (easily plucked painlessly)
Behavioural/Neurological:
- Apathy, listlessness, anorexia when alone
- Becomes very irritable when held or disturbed
Metabolic/Lab:
- Serum albumin: Markedly low (hypoalbuminaemia)
- Hypoproteinaemia, hypokalaemia (leaky cell membranes)
Liver:
- Enlarged, fatty liver (hepatic steatosis) due to reduced synthesis of apolipoprotein carriers needed for VLDL assembly, causing fat accumulation in hepatocytes
Immunity:
- Thymic and lymphoid atrophy
- Defects in cell-mediated immunity
- Increased susceptibility to infections (secondary infections produce further catabolism)
GI tract:
- Mucosal atrophy, villus blunting, loss of brush border enzymes
- Disaccharidase (especially lactase) deficiency - initial intolerance to milk-based diets during refeeding
- Malabsorption of carbohydrates, fats, and vitamins
Cardiovascular:
- Reduced myocardial mass, bradycardia, low blood pressure, decreased cardiac output
Haematological:
- Bone marrow hypoplasia, anaemia (normocytic/microcytic/macrocytic depending on predominant deficiency), leukopenia, lymphocytopenia
C. Marasmic Kwashiorkor (Combined/Overlap)
- Features of both - severe wasting combined with oedema
- Weight < 60% of expected
- Represents the most severe spectrum of SAM
5. Preventive Measures to Reduce PEM in India
"There is no simple solution to the problem of PEM. Many types of actions are necessary."
- Park's Textbook of Preventive and Social Medicine, p.736-737
The FAO/WHO Expert Committee framework organizes prevention across four levels:
(a) Health Promotion
- Maternal nutrition: Education and distribution of nutritional supplements to pregnant and lactating women
- Breastfeeding promotion: Exclusive breastfeeding for 6 months; continued breastfeeding up to 2 years with complementary foods
- Weaning foods: Development of low-cost, locally available, protein-energy-rich weaning foods; frequent small feeds rather than three large meals
- Family diet improvement: Encourage use of pulses, eggs, green leafy vegetables, and fortified foods
- Nutrition education: Promotion of correct feeding practices at community and household level
- Home economics: Training in food preparation, storage, and preservation
- Family planning: Spacing of births to allow adequate nutrition per child; reducing family size
- Family environment improvement: Poverty alleviation, improved living conditions
(b) Specific Protection
- Dietary protein and energy: Ensure the child's diet contains protein-rich and energy-dense foods (milk, eggs, pulses, fresh fruits)
- Immunization: Prevents infections that trigger malnutrition (measles vaccine is particularly important as measles precipitates severe PEM)
- Food fortification: Addition of micronutrients to staple foods:
- Vitamin A in cooking oil/dalda
- Iodine in salt
- Iron in cereals (iron fortification)
(c) Early Diagnosis and Treatment
- Periodic nutritional surveillance: Growth monitoring using growth charts at Anganwadi centres (ICDS)
- Early identification of growth faltering: Growth charts are the most practical field tool - usable by frontline health workers
- MUAC screening: MUAC < 12.5 cm = severe malnutrition; < 11.5 cm = SAM
- Early treatment of infections and diarrhoea: Prevents malnutrition-infection vicious cycle
- ORS programmes: Oral Rehydration Therapy for diarrhoea to prevent further nutritional losses
- Supplementary feeding: During disease epidemics, enhanced feeding programmes for vulnerable children
- Deworming: Treatment of intestinal helminthiasis (hookworm, Ascaris) to improve nutrient absorption
(d) Rehabilitation
- Nutrition Rehabilitation Centres (NRCs): In-patient management of SAM with medical complications; education of mothers on feeding
- Hospital treatment: WHO 10-step management of severe malnutrition (treat hypoglycaemia, hypothermia, dehydration, infections, micronutrient deficiency, etc.)
- Community-based management of SAM (CMAM): Ready-to-use therapeutic food (RUTF) for uncomplicated SAM at home
- Follow-up care: Prevent relapse after discharge; continued monitoring
National Programmes in India Targeting PEM
| Programme | Key Nutritional Intervention |
|---|---|
| ICDS (Integrated Child Development Services) | Supplementary nutrition, growth monitoring, nutrition + health education for under-6 children and pregnant/lactating women |
| POSHAN Abhiyan (National Nutrition Mission) | Targets stunting, wasting, underweight, anaemia; convergence of multiple schemes |
| Mid-Day Meal Scheme | Cooked mid-day meal to school children; addresses school-age undernutrition |
| NHM - Nutrition Rehabilitation Centres (NRCs) | In-patient care for SAM children with complications |
| MAA (Mothers' Absolute Affection) | Promotes breastfeeding at community level |
| Pradhan Mantri Matru Vandana Yojana (PMMVY) | Cash incentive for first child to promote ante-natal care and adequate nutrition |
| National Iodine Deficiency Disorders Control Programme | Universal salt iodization |
| Vitamin A Supplementation Programme | Periodic Vitamin A supplementation to children 6 months - 5 years |
Quick Revision Summary
| Point | Key Fact |
|---|---|
| Definition of malnutrition | Deficiency, excess, or imbalance of energy/nutrients |
| PEM primary cause | Food gap (inadequate quantity + quality) + infections |
| Kwashiorkor hallmark | Oedema + hypoalbuminaemia + fatty liver + "flaky paint" skin + hair changes |
| Marasmus hallmark | Severe wasting, NO oedema, preserved albumin, alert child |
| SAM diagnosis | WHZ < -3 SD OR MUAC < 115 mm OR bilateral oedema |
| First indicator of PEM | Underweight-for-age (detected on growth chart) |
| MUAC: severe malnutrition | < 12.5 cm; SAM: < 11.5 cm |
| Kwashiorkor liver | Fatty hepatomegaly (apolipoprotein synthesis decreased) |
| Most vulnerable immune function | T-cell-mediated immunity |
| Vicious cycle | Malnutrition → infection → worsened malnutrition |
| Generations | Malnourished girl → LBW baby → malnourished child |
| Key vaccine preventing PEM | Measles vaccine |
References:
- Park's Textbook of Preventive and Social Medicine, Nutritional Problems in Public Health, pp. 735-737
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, Nutritional Disease, pp. 411-413
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Protein-Energy Malnutrition, pp. 86-88
This is a shared conversation. Sign in to Orris to start your own chat.