ABG analysis Medicine
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive information to compile a thorough ABG analysis guide. Let me put it all together:
Arterial Blood Gas (ABG) Analysis
Normal ABG Values
| Parameter | Normal Range |
|---|---|
| pH | 7.35 - 7.45 |
| PaCO2 | 35 - 45 mmHg |
| PaO2 | 80 - 100 mmHg |
| HCO3- | 22 - 26 mEq/L |
| SaO2 | 95 - 100% |
| Base Excess | -2 to +2 mEq/L |
Step-by-Step ABG Interpretation
Step 1 - Assess the pH
- pH < 7.35 = Acidosis
- pH > 7.45 = Alkalosis
- pH 7.35-7.45 = Normal (but a primary disorder may still exist with compensation)
Step 2 - Determine the Primary Process (Respiratory vs. Metabolic)
| Condition | pH | PaCO2 | HCO3- |
|---|---|---|---|
| Respiratory Acidosis | ↓ | ↑ (>45) | Normal/↑ (compensatory) |
| Respiratory Alkalosis | ↑ | ↓ (<35) | Normal/↓ (compensatory) |
| Metabolic Acidosis | ↓ | Normal/↓ (compensatory) | ↓ (<22) |
| Metabolic Alkalosis | ↑ | Normal/↑ (compensatory) | ↑ (>26) |
Rule: In a simple disorder, the pH and PaCO2 move in opposite directions for respiratory disorders; in metabolic disorders, the pH and HCO3- move in the same direction.
Step 3 - Assess Compensation
Compensation never fully corrects the pH. If the pH is normalized, suspect a mixed disorder.
| Primary Disorder | Expected Compensation |
|---|---|
| Metabolic Acidosis | ↓ PCO2 = 1.3 × ↓ HCO3- (Winter's formula below) |
| Metabolic Alkalosis | ↑ PCO2 = 0.6 × ↑ HCO3- |
| Respiratory Acidosis (Acute) | HCO3- ↑ by 1 mmol/L per 10 mmHg ↑ in PCO2 |
| Respiratory Acidosis (Chronic) | HCO3- ↑ by 4 mmol/L per 10 mmHg ↑ in PCO2 |
| Respiratory Alkalosis (Acute) | HCO3- ↓ by 2 mmol/L per 10 mmHg ↓ in PCO2 |
| Respiratory Alkalosis (Chronic) | HCO3- ↓ by 5 mmol/L per 10 mmHg ↓ in PCO2 |
Winter's Formula (Metabolic Acidosis Compensation Check)
Expected PCO2 = (1.5 × HCO3-) + 8 ± 2
- If measured PCO2 > expected → concurrent respiratory acidosis
- If measured PCO2 < expected → concurrent respiratory alkalosis
- If measured PCO2 = expected → pure metabolic acidosis with appropriate compensation
Useful trick: In metabolic acidosis, expected PCO2 approximately equals the last two digits of the pH. (e.g., pH 7.23 → expected PCO2 ≈ 23 mmHg)
Step 4 - Calculate the Anion Gap (AG)
AG = Na+ - (Cl- + HCO3-) Normal = 8-12 mEq/L (or up to 16 if albumin-uncorrected)
An elevated AG indicates the presence of an unmeasured anion.
High AG Metabolic Acidosis - Mnemonic: MUDPILES CAT (or GOLD MARK - newer)
| MUDPILES | |
|---|---|
| M | Methanol, Metformin |
| U | Uremia |
| D | DKA (Diabetic Ketoacidosis) |
| P | Paraldehyde, Phenformin |
| I | Isoniazid, Iron |
| L | Lactic acidosis |
| E | Ethylene glycol |
| S | Salicylates |
Normal AG (Hyperchloremic) Metabolic Acidosis - Mnemonic: HARD-UP / DURHAM
Common causes: diarrhea, RTA (renal tubular acidosis), acetazolamide, ureteroenteric fistula.
Step 5 - Delta-Delta Ratio (for High AG Metabolic Acidosis)
Used to detect a concurrent metabolic alkalosis or normal-AG acidosis hidden behind a high-AG acidosis.
Delta ratio = (AG - 12) / (24 - HCO3-)
| Delta Ratio | Interpretation |
|---|---|
| < 0.4 | Pure normal-AG (hyperchloremic) acidosis |
| 0.4 - 0.8 | Mixed high-AG + normal-AG acidosis |
| 1.0 - 2.0 | Pure high-AG metabolic acidosis |
| > 2.0 | High-AG acidosis + concurrent metabolic alkalosis |
Step 6 - Assess Oxygenation
A-a Gradient (Alveolar-Arterial PO2 Difference)
PAO2 = FiO2 × (Patm - PH2O) - (PaCO2/RQ) On room air: PAO2 = 150 - (PaCO2 / 0.8) A-a gradient = PAO2 - PaO2
Normal A-a gradient: < 10 mmHg (increases with age: ~2.5 + 0.21 × age)
| A-a Gradient | Cause of Hypoxemia |
|---|---|
| Normal | Hypoventilation (e.g., CNS depression, obesity) |
| Elevated | V/Q mismatch, shunt, diffusion defect |
Acid-Base Map
This map plots PCO2 (x-axis) against pH (y-axis) to classify simple and mixed disorders:
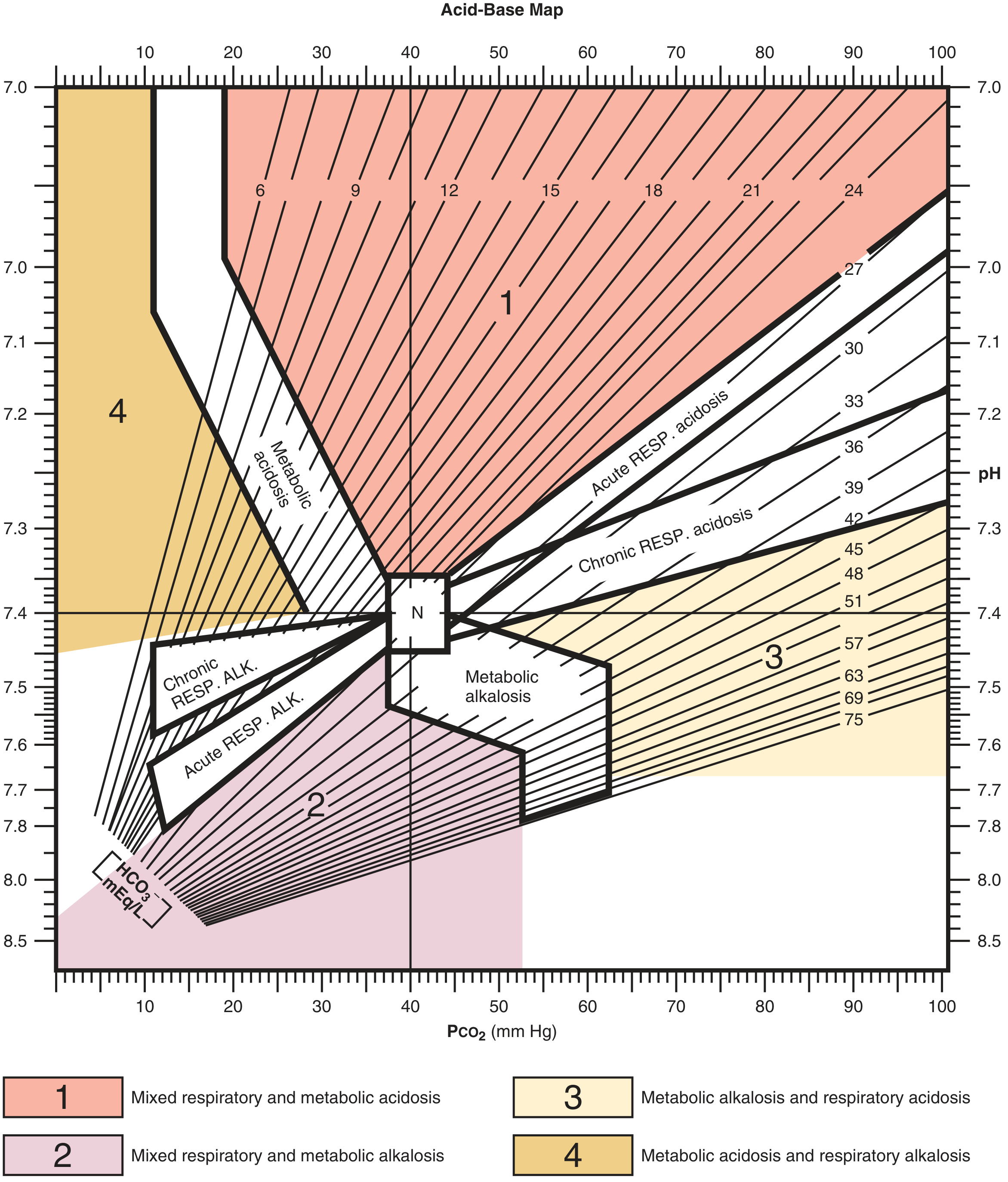
- Zone 1 (red): Mixed respiratory + metabolic acidosis
- Zone 2 (pink): Mixed respiratory + metabolic alkalosis
- Zone 3 (tan): Metabolic alkalosis + respiratory acidosis
- Zone 4 (gold): Metabolic acidosis + respiratory alkalosis
- N: Normal zone
Mixed Disorders (Harrison's, 22nd Ed.)
| Pattern | Key Finding | Classic Example |
|---|---|---|
| Met. Acidosis + Resp. Alkalosis | High AG; PaCO2 below predicted | Lactic acidosis + sepsis |
| Met. Acidosis + Resp. Acidosis | High AG; PaCO2 above predicted | Severe pneumonia/pulmonary edema |
| Met. Alkalosis + Resp. Alkalosis | PaCO2 does not rise as predicted | Liver disease + diuretics |
| Met. Alkalosis + Resp. Acidosis | PaCO2 higher than predicted; pH near normal | COPD + diuretics |
| High-AG Acidosis + Met. Alkalosis | ΔAG >> ΔHCO3- | Uremia + vomiting |
| Mixed High-AG + Normal-AG Acidosis | ΔHCO3- > ΔAG | Diarrhea + lactic acidosis |
Osmolal Gap (for Toxic Ingestions)
OsmCalc = 2×Na + (BUN/2.8) + (Glucose/18) Osmolal Gap = OsmMeasured - OsmCalc Normal = 5-10 mOsm/kg; gap >10 suggests unmeasured osmoles
Causes of elevated osmolal gap: methanol, ethylene glycol, isopropyl alcohol, ethanol, acetone.
Worked Clinical Examples
Example 1 - Diarrhea (from Roberts & Hedges):
Na 133 | K 2.8 | Cl 118 | pH 7.26 | PCO2 13 | HCO3- 5
- pH 7.26 = Acidosis; HCO3- low = Metabolic acidosis
- Winter's: Expected PCO2 = 1.5×5 + 8 = 15.5 → Actual = 13 ≈ within range
- Conclusion: Pure metabolic acidosis, appropriate respiratory compensation
Example 2 - Sepsis (Harrison's):
Na 140 | Cl 106 | HCO3- 14 | PaCO2 24 | pH 7.39
- AG = 140-(106+14) = 20 (elevated)
- pH near normal; HCO3- low; PCO2 low
- Delta ratio: (20-12)/(24-14) = 0.8 → approaching pure high-AG
- Conclusion: High-AG metabolic acidosis (lactic) + respiratory alkalosis (sepsis-driven hyperventilation)
Example 3 - COPD + Diuretics (Harrison's):
Na 140 | Cl 88 | HCO3- 42 | PaCO2 67 | pH 7.42
- pH 7.42 = near normal; both HCO3- and PCO2 elevated
- Conclusion: Metabolic alkalosis (diuretic-induced) + respiratory acidosis (COPD) - pH appears "normal" masking both
Sources
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, Acid-Base Balance section
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Ch. 58 - Mixed Acid-Base Disorders
- Tintinalli's Emergency Medicine - A Comprehensive Study, ABG Analysis
- Murray & Nadel's Textbook of Respiratory Medicine - Arterial Blood Gas
This is a shared conversation. Sign in to Orris to start your own chat.