Inflammatory bowel diseases, its types, gross features, clinical manifestations, and, uh, its, uh, treatment. Uh, how do you manage with the detailed explanation?
Reading File
Finding Sources
Finding Sources
Searching PubMed
"inflammatory bowel disease" AND management
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive data. Let me compile the full answer.
Inflammatory Bowel Disease (IBD): A Comprehensive Overview
1. Definition and Overview
IBD is a group of chronic, relapsing-remitting disorders characterized by idiopathic inflammation of the gastrointestinal tract. The two main forms are Crohn's Disease (CD) and Ulcerative Colitis (UC). A third, less common entity - Indeterminate Colitis - is diagnosed when features of both overlap and cannot be distinguished even after full evaluation.
The etiology involves a complex interplay of genetic susceptibility, dysregulated mucosal immunity, and environmental/microbial triggers. IBD has a bimodal age of onset: a primary peak at 15-40 years and a smaller second peak in the 6th-7th decades.
2. Types of IBD
A. Crohn's Disease (CD)
- Can affect any part of the GI tract from mouth to anus
- Most commonly involves the terminal ileum and ileocecal region (~70%)
- Primary ileal: 30%
- Ileocolonic: 40%
- Isolated colonic: 25%
- Characterized by transmural inflammation with "skip lesions" (areas of normal bowel between affected segments)
- Female-to-male ratio: 1.2:1
B. Ulcerative Colitis (UC)
- Confined strictly to the colon and rectum
- Starts at the rectum and extends proximally in a continuous, uninterrupted pattern
- Inflammation is mucosal only (not transmural)
- Distribution at diagnosis:
- Proctosigmoiditis: 44-49%
- Left-sided colitis: 36-41%
- Pancolitis: 14-37%
- Sex ratio: 1:1
Comparison Table (Goldman-Cecil Medicine)
| Feature | Crohn's Disease | Ulcerative Colitis |
|---|---|---|
| Sites of involvement | Esophagus to anus | Colon only |
| Skip areas | Yes | No |
| Transmural inflammation | Yes | No |
| Type of ulceration | Usually discrete | Continuous |
| Fistula | Yes | No |
| Stricture | Yes | No |
| Perianal disease | Yes | No |
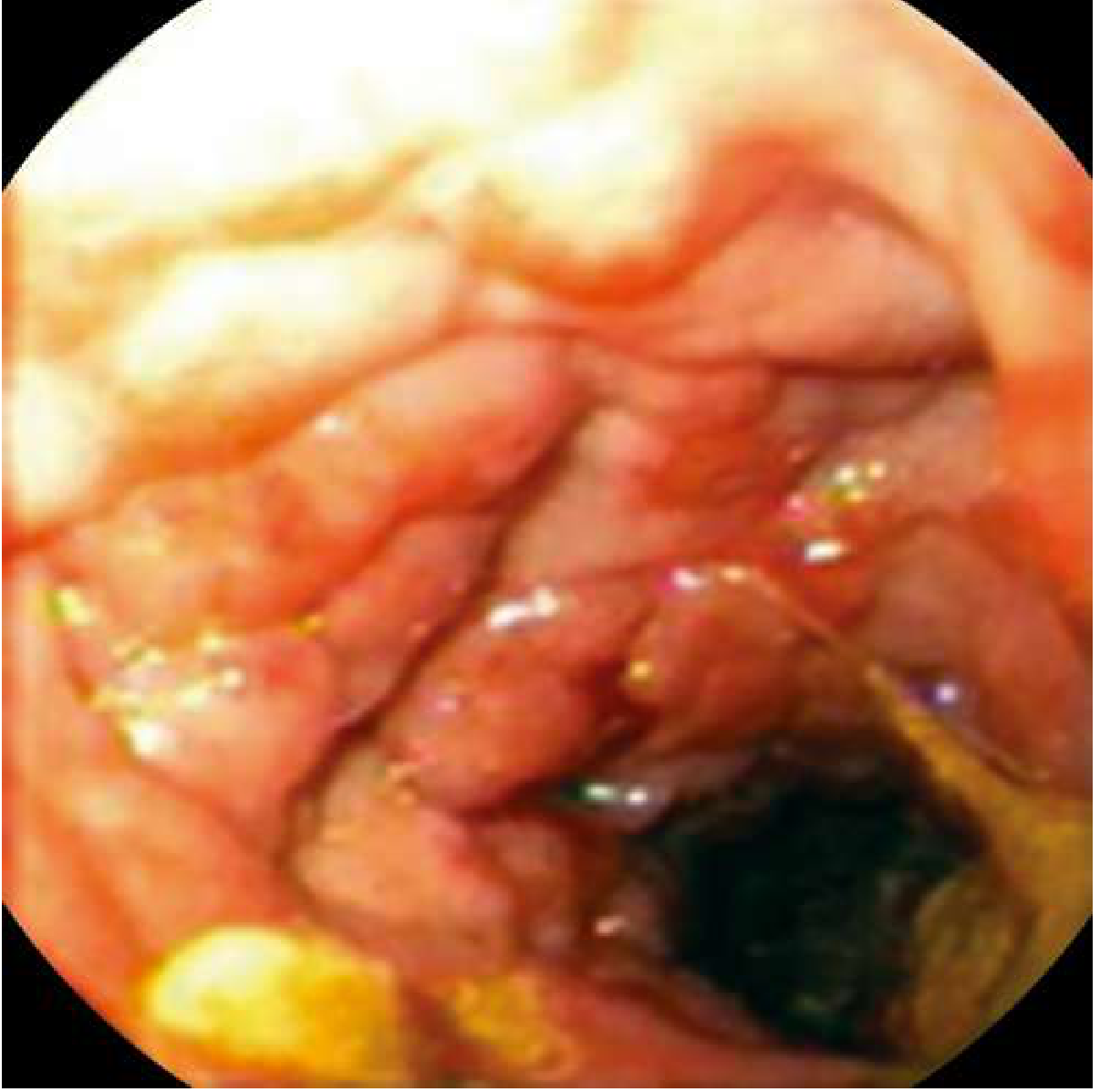
3. Gross & Endoscopic Features
Crohn's Disease - Gross Features
- Aphthous ulcers are the earliest mucosal change - small, superficial mucosal erosions
- As disease progresses, ulcers deepen and become round, linear, or serpiginous
- Cobblestone appearance: intersecting longitudinal and transverse deep ulcers with intervening islands of edematous normal mucosa ("stones")
- Skip lesions: diseased segments alternating with normal bowel
- Mural thickening with "creeping fat" (mesenteric fat wrapping around bowel wall)
- Strictures (fibrotic narrowing from transmural healing)
- Fistulae (enteroenteric, enterocutaneous, rectovaginal, enterovesicular)
- Noncaseating granulomas on histology (pathognomonic when present, but found in only ~30% of biopsies)
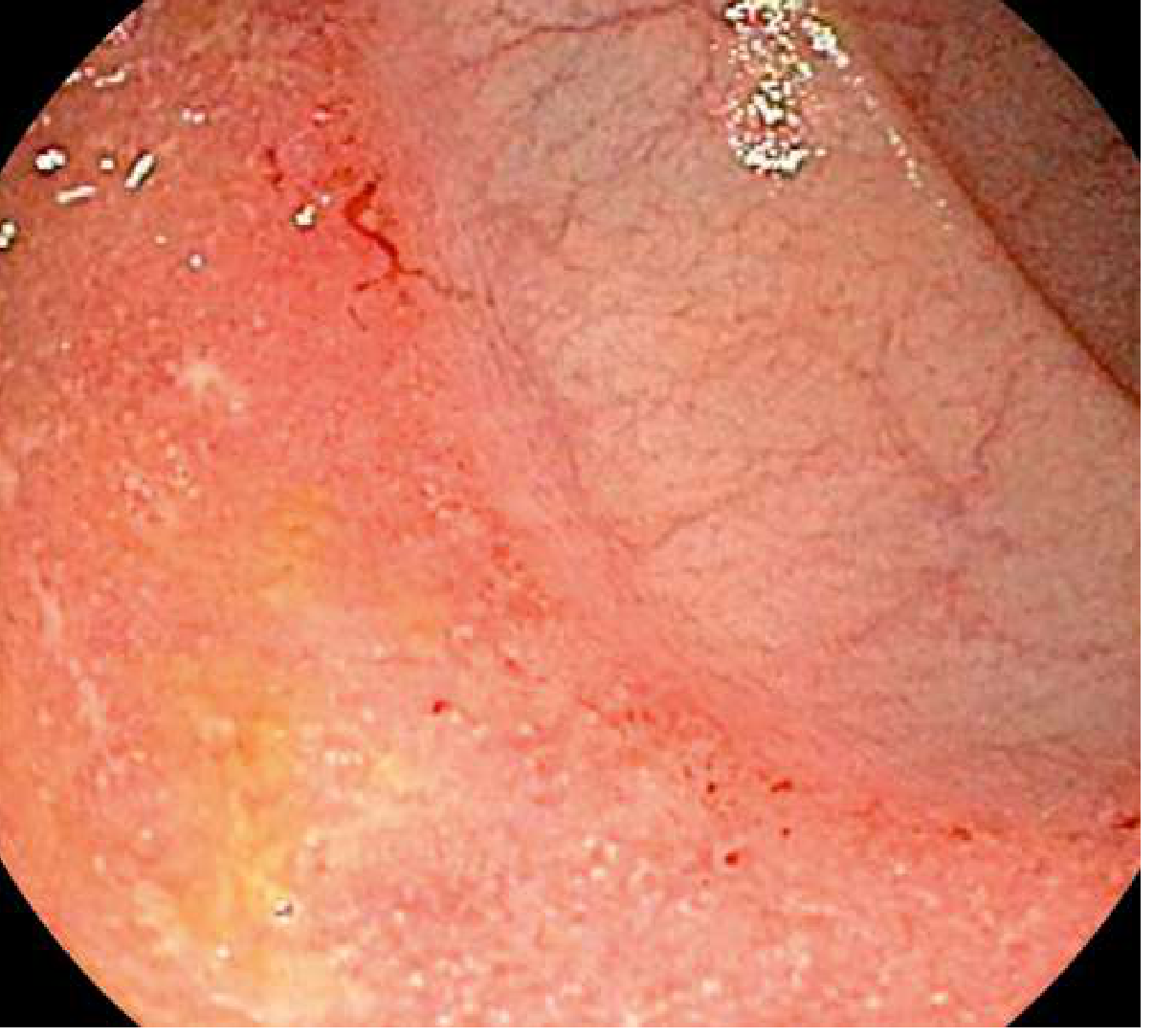
Ulcerative Colitis - Gross Features
- Early disease: diffuse mucosal erythema, loss of normal vascular pattern, granular/edematous mucosa
- Moderate disease: mucosal friability, contact bleeding (bleeds on touch), superficial ulceration
- Severe disease: confluent ulceration, spontaneous bleeding, mucosal sloughing
- Pseudopolyps: islands of regenerating epithelium surrounded by ulceration in long-standing disease - marker of more severe disease
- Inflammation is continuous from the rectum, going proximally
- "Backwash ileitis" may occur as a spillover from the cecum (not true ileal involvement)
- In chronic disease, the colon may shorten and narrow ("lead-pipe colon") with loss of haustrations
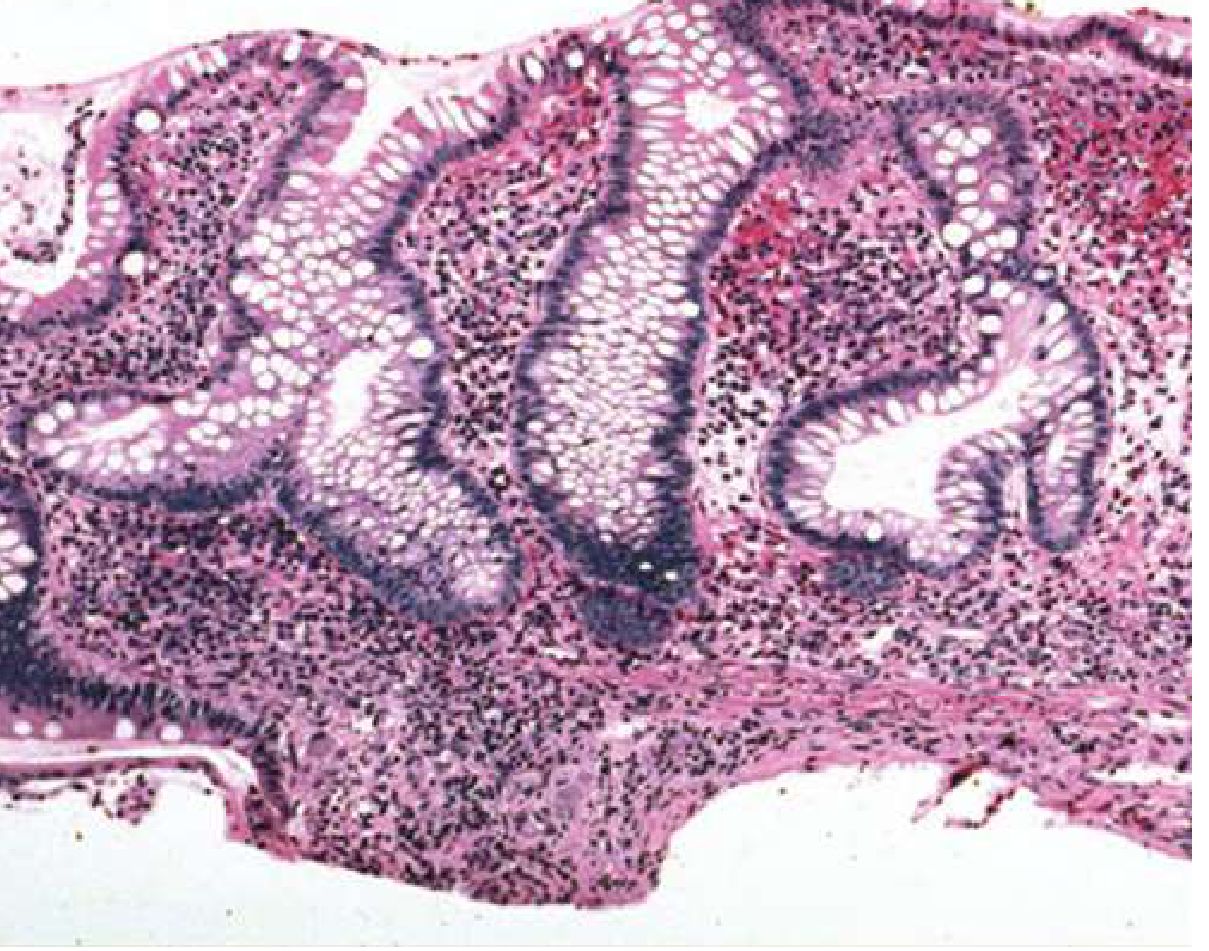
Histopathology of Ulcerative Colitis
4. Clinical Manifestations
Crohn's Disease
Intestinal symptoms (vary by location):
- Right lower quadrant pain (most common - reflects terminal ileal disease)
- Diarrhea (may be non-bloody if small bowel disease; bloody if colonic)
- Hematochezia in colonic disease
- Obstructive symptoms: colicky pain, distension, nausea/vomiting (strictures)
- Malabsorption/steatorrhea: fat-soluble vitamin deficiencies (A, D, E, K), vitamin B12 deficiency from terminal ileal disease
- Dysphagia/odynophagia: upper GI Crohn (rare, <2%)
- Perianal disease (20-30%): fistulas, abscesses, fissures, skin tags, rectal stricture
Fistulae occur in 20-40% and include:
- Enteroenteric (internal)
- Rectovaginal - fluid/gas per vagina
- Enterovesicular - pneumaturia, recurrent UTIs
- Enterocutaneous - external drainage
- Perianal
Ulcerative Colitis
- Bloody diarrhea (cardinal symptom) - blood mixed with stool
- Tenesmus (painful urge to defecate with feeling of incomplete evacuation)
- Mucus in stool (excessive)
- Urgency to defecate
- Abdominal cramping/pain
- Proctitis/proctosigmoiditis may paradoxically present with constipation (hard stool proximal, inflamed distal segment)
- Weight loss, fever, fatigue in extensive or severe disease
- Nausea/vomiting from pain
- Peripheral edema from hypoalbuminemia in severe disease
Extraintestinal Manifestations (Both)
| System | Manifestation | Notes |
|---|---|---|
| Joints | Peripheral arthropathy, ankylosing spondylitis, sacroiliitis | Most common EIM (10-20%); mirrors gut activity |
| Skin | Erythema nodosum (10-15%), pyoderma gangrenosum (1-2%) | EN correlates with gut flares; PG may be independent |
| Eyes | Uveitis, episcleritis | 5-15% |
| Hepatobiliary | Primary sclerosing cholangitis (PSC) | 2-7.5% of IBD; 70-80% of PSC patients have UC |
| Renal | Calcium oxalate stones (CD with fat malabsorption), uric acid stones | Up to 10% |
| Oral | Aphthous stomatitis | CD only |
| Bone | Osteoporosis (~15%) | Steroid-related major risk factor |
| Vascular | DVT/PE | Increased thromboembolic risk, especially in active disease |
| Neurologic | Peripheral neuropathy (B12 def), optic neuritis | Rare |
5. Diagnosis
- Colonoscopy with biopsy - gold standard; must reach terminal ileum
- CT/MRI enterography - preferred for small bowel assessment; detects strictures, fistulae, abscesses
- Capsule endoscopy - used when above tests non-diagnostic (contraindicated in strictures)
- Histopathology: noncaseating granulomas (CD), crypt distortion + continuous mucosal inflammation (UC)
- Lab markers: CRP, ESR (activity markers), fecal calprotectin (elevated in active disease), CBC (anemia, leukocytosis), albumin
- Serologic markers:
- ASCA (IgA + IgG) positive: 40-70% of CD, highly specific when combined (89-100%)
- pANCA positive: 55% of UC, 20% of CD
6. Treatment and Management
Treatment is organized by disease severity (mild/moderate/severe) and aims to induce remission, then maintain remission and prevent complications.
Step 1 - Aminosalicylates (5-ASA)
Drugs: Mesalamine (oral, rectal), Sulfasalazine, Olsalazine, Balsalazide
- Mechanism: Topical anti-inflammatory action on the colonic mucosa; inhibition of NF-kB, prostaglandin synthesis, and free radical scavenging
- Use: Mild-to-moderate UC (first-line); also used for maintenance of remission in UC
- Dosing: Mesalamine 2.4-4.8 g/day orally; rectal forms (suppositories, enemas) for distal disease
- Sulfasalazine requires colonic bacteria to cleave the 5-ASA from its sulfapyridine carrier
- Limited role in CD: 5-ASA has minimal proven benefit in Crohn's disease
- Side effects of sulfasalazine: dose-dependent nausea, headache, oligospermia (reversible); hypersensitivity reactions (sulfa allergy)
Step 2 - Corticosteroids
Drugs: Prednisone, Methylprednisolone (systemic); Budesonide (locally-acting)
- Mechanism: Broad immunosuppression - inhibit NF-kB, reduce cytokine production, suppress neutrophil/macrophage function
- Use: Induction of remission in moderate-to-severe UC or CD; NOT used for maintenance (long-term toxicity)
- Prednisone/Prednisolone: 40-60 mg/day orally, tapered once response achieved
- IV Methylprednisolone: 40-60 mg/day for hospitalized severe disease
- Budesonide: first-pass hepatic metabolism limits systemic toxicity; used for ileal/right-colon CD; 9 mg/day orally
- Side effects: osteoporosis, avascular necrosis of hip, Cushing's syndrome, hyperglycemia, hypertension, infection risk, adrenal suppression
Step 3 - Immunomodulators (Thiopurines & Methotrexate)
Drugs: Azathioprine (AZA), 6-Mercaptopurine (6-MP), Methotrexate
- Mechanism of thiopurines: Converted to 6-thioguanine nucleotides that incorporate into DNA and inhibit purine synthesis, suppressing lymphocyte proliferation
- Mechanism of methotrexate: Inhibits dihydrofolate reductase; anti-inflammatory effects at low doses
- Use: Steroid-sparing agents; maintenance of remission; often combined with anti-TNF biologics to reduce immunogenicity
- AZA: 2-2.5 mg/kg/day; 6-MP: 1-1.5 mg/kg/day; onset of action 3-6 months
- Thiopurine methyltransferase (TPMT) testing required before initiation (gene variant = myelosuppression risk)
- Side effects: myelosuppression (most serious), hepatotoxicity, pancreatitis (6-MP/AZA), increased lymphoma risk (EBV-related), nausea
- Methotrexate: 15-25 mg IM/SC weekly for CD; requires folate supplementation; teratogenic
Step 4 - Biologic Therapies
Anti-TNF-alpha Agents (First-line Biologics)
Drugs: Infliximab, Adalimumab, Certolizumab pegol (CD), Golimumab (UC)
- Mechanism: Bind and neutralize TNF-alpha, a central pro-inflammatory cytokine; some induce apoptosis of activated T cells
- Infliximab (chimeric IgG1): IV infusion 5 mg/kg at weeks 0, 2, 6, then every 8 weeks maintenance; effective in CD (including fistulizing) and UC
- Adalimumab (fully human): SC injection 160 mg, then 80 mg at week 2, then 40 mg every 2 weeks
- Golimumab: SC injection; approved for moderate-to-severe UC
- Side effects: reactivation of latent TB (screen before starting), hepatitis B reactivation, serious infections (bacterial, fungal), demyelinating disease, lymphoma, worsening CHF
- Combination therapy (anti-TNF + thiopurine) shown superior to monotherapy (SONIC trial data) in CD
Anti-Integrin Agents
Drug: Vedolizumab
- Mechanism: Humanized monoclonal antibody that binds the alpha-4-beta-7 integrin on lymphocytes, preventing their binding to MAdCAM-1 on intestinal vascular endothelium - gut-selective (does not affect CNS trafficking, so lower PML risk than natalizumab)
- Dosing: 300 mg IV at weeks 0, 2, 6, then every 8 weeks maintenance
- Use: Moderate-to-severe CD and UC; approved for both
- Side effects: headache, hypersensitivity, arthralgia, nasopharyngitis, fatigue
- Note: Anti-TNF drugs may enhance adverse effects of vedolizumab
Drug: Natalizumab
- Chimeric anti-alpha-4 integrin; approved for moderate-severe CD; associated with progressive multifocal leukoencephalopathy (PML) risk due to JC virus reactivation - requires JC virus antibody testing before use
Anti-IL-12/23 Agent
Drug: Ustekinumab
- Mechanism: Fully humanized IgG1 monoclonal antibody targeting the p40 subunit shared by IL-12 and IL-23, blocking signaling through IL-12Rβ1 and IL-23R on T cells and NK cells
- Dosing: Initial single IV dose (weight-based: 260-520 mg), then 90 mg SC every 8 weeks for maintenance
- Use: Moderate-to-severe CD (approved); also approved for UC
- Side effects: Upper respiratory infections, headache, arthralgia, nasopharyngitis; long half-life (up to 120 days) - must discontinue 15 weeks before live vaccines
JAK Inhibitors (Small Molecules)
Drug: Tofacitinib, Upadacitinib (UC); Upadacitinib (CD)
- Mechanism: Block Janus kinase (JAK) signaling, which is used by multiple cytokine receptors (IL-2, IL-6, IFN-gamma, etc.), broadly suppressing inflammatory cytokine pathways
- Use: Moderate-to-severe UC; oral agents offering an alternative to biologics
- Side effects: Serious infections (herpes zoster, VZV reactivation), lipid elevations, potential cardiovascular/thrombotic events, MACE risk (class warning in older patients)
Step 5 - Surgical Management
Ulcerative Colitis:
- Total proctocolectomy with ileal pouch-anal anastomosis (IPAA / J-pouch) is curative - UC is the only IBD that can be surgically cured
- Indications: Medically refractory disease, toxic megacolon, perforation, high-grade dysplasia/CRC, severe hemorrhage
- Complication: "Pouchitis" (inflammation of the J-pouch) in 50% of patients over time; treated with metronidazole or ciprofloxacin
Crohn's Disease:
- Surgery is not curative; reserved for complications
- Indications: Bowel obstruction from stricture, fistulae not responsive to medical therapy, abscesses, perforation, failure of medical management
- Strictureplasty: bowel-conserving procedure for fibrotic strictures
- High rate of post-surgical recurrence (endoscopic recurrence in >70% at 1 year without prophylaxis); anti-TNF maintenance recommended post-operatively
Additional Management Principles
- Nutritional support: Elemental/polymeric enteral nutrition can induce remission in CD (especially pediatric); TPN for severe disease with gut failure
- Antibiotics: Metronidazole and/or ciprofloxacin for perianal CD, intra-abdominal abscesses; no role in luminal UC/CD activity
- Cancer surveillance: Colonoscopy every 1-2 years after 8-10 years of pancolitis (UC); risk increases ~10% per decade
- Thromboprophylaxis: IBD patients have significantly elevated DVT/PE risk, especially during hospitalizations for active disease
- Bone health: DEXA scan; calcium + vitamin D supplementation; bisphosphonates for steroid-induced osteoporosis
- Vaccinations: Live vaccines contraindicated in patients on immunosuppression; pneumococcal, influenza, HPV, hepatitis B vaccines recommended
7. Summary - Treatment Ladder
MILD DISEASE
↓
5-ASA agents (UC) / Budesonide (ileal CD)
MODERATE DISEASE
↓
Corticosteroids (induction only) + Immunomodulators (maintenance)
MODERATE-SEVERE / STEROID-DEPENDENT
↓
Anti-TNF biologics ± Immunomodulator (combination)
or
Vedolizumab (gut-selective)
or
Ustekinumab (anti-IL-12/23)
or
JAK inhibitors (tofacitinib/upadacitinib - UC)
REFRACTORY / COMPLICATIONS
↓
Surgery (curative in UC; palliative in CD)
Key Textbook Sources:
- Goldman-Cecil Medicine, 26th ed. - Ch. 127, Clinical Characteristics, Symptoms, Extraintestinal Manifestations, Diagnosis & Treatment
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, 14th ed. - Ch. on Monoclonal Antibodies: Vedolizumab, Ustekinumab, Anti-TNF mechanisms
- Sleisenger and Fordtran's GI and Liver Disease - IBD and CRC surveillance
Recent Evidence Update: A 2024 AGA network meta-analysis (PMID 39425738) comparing advanced therapies for moderate-to-severe UC found that combination biologics and JAK inhibitors outperform older agents - consult this for current head-to-head ranking of therapies.
This is a shared conversation. Sign in to Orris to start your own chat.