Give me detail notes on Acyanotic heart disease from standard textbook so that I can get full out of full marks in university exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple standard textbooks (Robbins Pathology, Robbins & Kumar Basic Pathology, Harriet Lane Handbook, The Developing Human). Let me compile the full detailed notes.
Acyanotic Congenital Heart Disease - Complete Exam Notes
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology; Harriet Lane Handbook (Johns Hopkins); The Developing Human - Clinically Oriented Embryology
Overview & Classification
Congenital Heart Disease (CHD) refers to structural anomalies of the heart or great vessels that develop during embryogenesis. CHD affects approximately 1% of live births.
Acyanotic CHD = defects that do NOT initially cause cyanosis. These are broadly divided into:
| Category | Defects |
|---|---|
| Left-to-right shunts | VSD, ASD, PDA, AVSD |
| Obstructive lesions | Pulmonary stenosis, Aortic stenosis, Coarctation of the aorta |
Key concept: Left-to-right shunts are the MOST COMMON congenital heart defects. They are acyanotic initially because oxygenated blood flows from the high-pressure left side into the right side - no deoxygenated blood enters the systemic circulation. However, if pulmonary hypertension develops and reverses the shunt (right-to-left), Eisenmenger syndrome results and cyanosis appears.
Fig. 12.3 - Classic Left-to-Right Shunts (from Robbins)
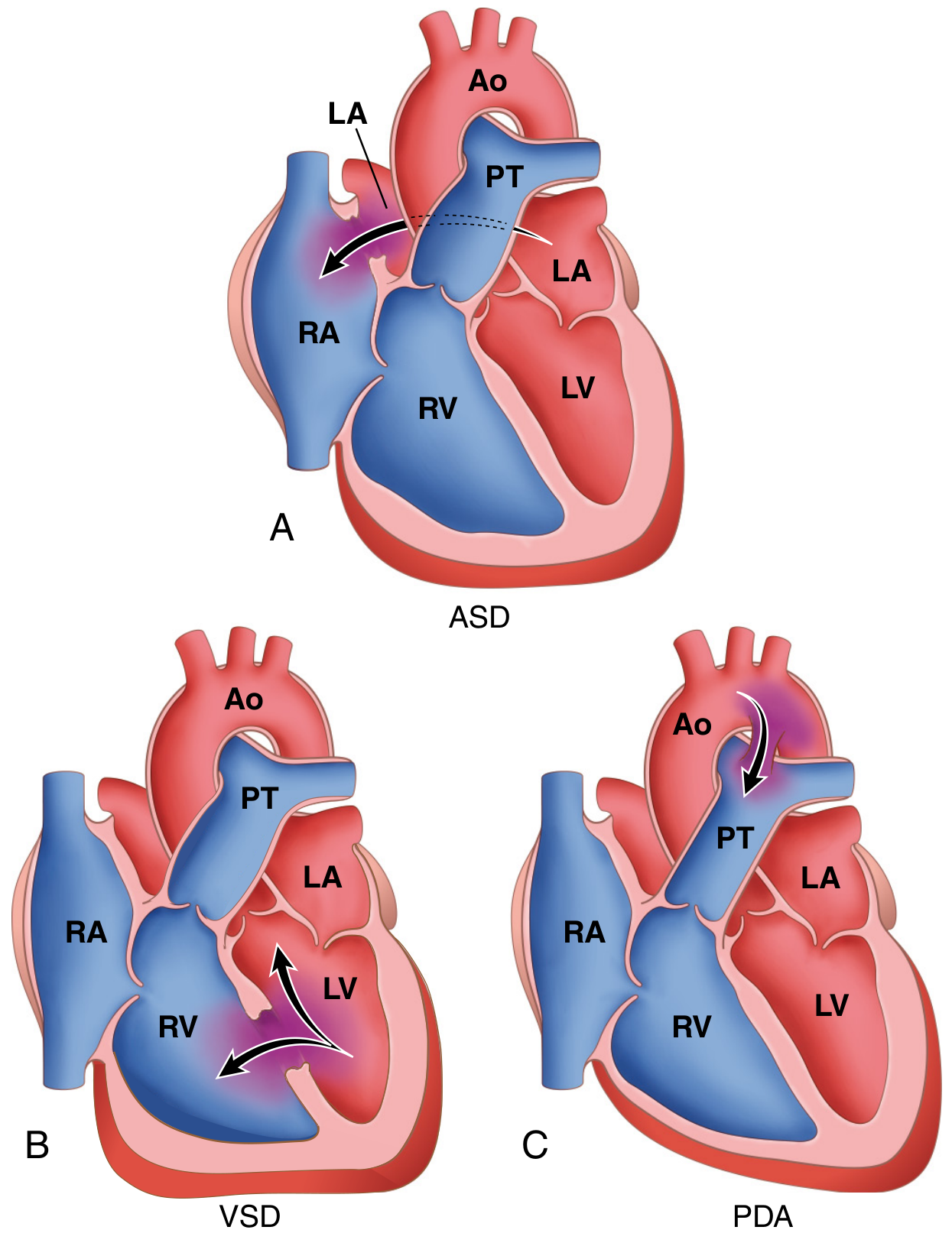
Common left-to-right shunts: (A) ASD - arrow shows L to R flow at atrial level; (B) VSD - bidirectional arrows showing shunting between ventricles; (C) PDA - arrow showing aorta-to-pulmonary trunk shunting. Ao = Aorta, PT = Pulmonary Trunk, LA = Left Atrium, LV = Left Ventricle, RA = Right Atrium, RV = Right Ventricle.
1. Ventricular Septal Defect (VSD)
Definition & Epidemiology
- Incomplete closure of the ventricular septum allowing free communication between left and right ventricles
- Most common CHD diagnosed at birth (approx. 42% of all CHDs)
- Only 20-30% of VSDs are isolated; the majority are associated with other cardiac malformations (e.g., Tetralogy of Fallot)
Embryology
- The ventricular septum forms from:
- A muscular ridge growing upward from the apex
- A membranous partition growing downward from the endocardial cushions
- The basal (membranous) region is the last to close → site of ~90% of VSDs
Morphology / Classification by Location
| Type | Frequency | Notes |
|---|---|---|
| Membranous VSD | ~90% | Just proximal to aortic valve; most common |
| Infundibular VSD | - | Below the pulmonary valve |
| Muscular VSD | 10% | May be multiple; most likely to close spontaneously |
- Most VSDs are 2-3 cm in diameter
- Right ventricle is hypertrophied and often dilated in significant shunts
- Pulmonary artery is dilated due to increased right ventricular output
Pathophysiology
- Left-to-right shunt → increased pulmonary blood flow AND pressure
- Large VSDs → early right ventricular hypertrophy → pulmonary hypertension
- Chronic, unclosed large VSD → irreversible pulmonary vascular disease → shunt reversal → Eisenmenger syndrome (cyanosis)
- Small/medium VSDs → jet lesion in right ventricle → endothelial damage → risk of infective endocarditis
Clinical Features
- Small VSD: Often asymptomatic; ~50% of muscular VSDs close spontaneously in infancy/childhood
- Large VSD: CHF from birth; recurrent respiratory infections; failure to thrive; pulmonary hypertension
Auscultation
- 2-5/6 holosystolic (or early systolic) murmur - loudest at left lower sternal border (LLSB)
- ± systolic thrill
- ± apical diastolic rumble with large shunt (from increased flow across mitral valve)
- With large VSD + pulmonary hypertension: S2 may become narrow or single
ECG Findings
| VSD Size | ECG |
|---|---|
| Small | Normal |
| Medium | LVH ± LAE |
| Large | BVH (biventricular hypertrophy) ± LAE; or pure RVH |
CXR
- Cardiomegaly with increased pulmonary vascular markings (PVMs) - proportional to degree of shunt
- Normal in small VSDs
Management
- Small VSDs: observe; may close spontaneously
- Large/symptomatic VSDs: surgical or catheter-based closure (early, before irreversible pulmonary disease)
- Infective endocarditis prophylaxis
2. Atrial Septal Defect (ASD)
Definition & Epidemiology
- Abnormal, fixed opening in the atrial septum allowing communication between left and right atria
- Most common CHD diagnosed in adults (VSDs more common overall, but close spontaneously; ASDs are less likely to close)
- NOT the same as Patent Foramen Ovale (PFO)
Embryology of Atrial Septum
- Septum primum - crescent-shaped ingrowth posteriorly; leaves anterior gap called ostium primum
- Before ostium primum closes, a second posterior opening forms: ostium secundum
- Septum secundum grows to the right of septum primum; covers ostium secundum but leaves foramen ovale
- The foramen ovale/ostium secundum permits right-to-left flow in fetal life (when pulmonary pressures > systemic)
- At birth: lung expansion drops pulmonary pressure → left atrial pressure exceeds right → foramen ovale valve closes → usually permanently sealed by adulthood
Classification of ASDs
| Type | Frequency | Location |
|---|---|---|
| Secundum ASD | ~90% | Center of the atrial septum (fossa ovalis region); deficient septum secundum |
| Primum ASD | ~5% | Lower atrial septum; associated with AV cushion defects; often seen with Down syndrome |
| Sinus venosus ASD | ~5% | Upper atrial septum near SVC entry; associated with anomalous pulmonary venous return |
Pathophysiology
- Left-to-right shunt → increased volume to right heart and pulmonary circulation
- Pulmonary flow may be 2-8 times normal
- Well tolerated for decades - right ventricle is very compliant
- Eventually: right ventricular failure, pulmonary hypertension, paradoxical embolism
- Unlike VSD, ASDs rarely cause irreversible pulmonary hypertension - but it can occur after age 30-40 years
Clinical Features
- Usually asymptomatic until adulthood (3rd-4th decade)
- Palpitations, dyspnea, fatigue
- Complications: atrial fibrillation, heart failure, paradoxical embolization (stroke)
- Small ASDs (<1 cm): well tolerated throughout life
Auscultation
- Wide, FIXED split S2 (hallmark sign - due to prolonged right ventricular ejection)
- Grade 2-3/6 systolic ejection murmur at left upper sternal border (LUSB) (from increased flow across pulmonary valve)
- May have mid-diastolic rumble at LLSB (from increased tricuspid flow)
ECG Findings
| ASD Size | ECG |
|---|---|
| Small | Normal |
| Large | RAD (right axis deviation) + mild RVH OR RBBB with RSR' pattern in V1 (classic) |
CXR
- Cardiomegaly with increased PVMs if hemodynamically significant
- Right atrial and right ventricular enlargement
- Prominent pulmonary artery
Management
- Surgical or intravascular (catheter-based) closure - to prevent heart failure, paradoxical embolization, irreversible pulmonary vascular disease
- Secundum ASDs: amenable to percutaneous device closure
- Primum ASDs: require surgical repair
- Mortality is low; postoperative survival comparable to unaffected population
3. Patent Ductus Arteriosus (PDA)
Definition & Embryology
- The ductus arteriosus arises from the left pulmonary artery and joins the aorta just distal to the origin of the left subclavian artery
- In fetal life: allows blood to flow from pulmonary artery → aorta (bypassing non-functional lungs)
- At birth (in healthy term infants): closes within 1-2 days in response to:
- Increased arterial oxygenation
- Decreased pulmonary vascular resistance
- Declining prostaglandin E2 levels
- Complete obliteration within first few months → ligamentum arteriosum
- Closure can be delayed by hypoxia (e.g., respiratory distress syndrome, high altitude)
Epidemiology
- Accounts for ~7% of congenital heart lesions
- 90% are isolated defects
- More common in premature infants (40-60% in Very Low Birth Weight [VLBW] infants)
- More common in females
Pathophysiology
- After birth: aortic pressure > pulmonary pressure → left-to-right shunt (aorta to pulmonary trunk)
- High-pressure shunt → increased pulmonary blood flow and pressure
- Can eventually cause Eisenmenger syndrome if untreated
Clinical Features
- Small PDA: Asymptomatic; discovered incidentally
- Large PDA: CHF, failure to thrive, recurrent chest infections
- High-pressure shunts → risk of infective endocarditis
Auscultation
- Continuous "machinery" murmur (throughout systole AND diastole) - loudest at left upper sternal border (LUSB) / left infraclavicular area
- Wide pulse pressure (due to diastolic run-off into pulmonary circulation)
- Grade 1-4/6 intensity
ECG Findings
| PDA Size | ECG |
|---|---|
| Small-moderate | Normal or LVH |
| Large | BVH (biventricular hypertrophy) |
CXR
- Cardiomegaly with increased PVMs depending on size of shunt
Management
- Indomethacin (prostaglandin synthesis inhibitor) - closes PDA in premature infants (pharmacological closure)
- Ibuprofen - alternative to indomethacin
- Surgical ligation or catheter-based device closure for larger PDAs or when pharmacotherapy fails
- Isolated PDAs should be closed as early in life as feasible
4. Atrioventricular Septal Defect (AVSD) / Atrioventricular Canal Defect
Definition
- Combined defect of the lower atrial septum (primum ASD) + upper ventricular septum + abnormal AV valves (common AV valve instead of separate mitral and tricuspid)
Associations
- Strongly associated with Down syndrome (Trisomy 21) - most common cardiac defect in Down syndrome
Clinical Features
- Hyperactive precordium with systolic thrill at LLSB
- Loud S1
- Grade 3-4/6 holosystolic regurgitant murmur at LLSB
- Systolic murmur of mitral regurgitation at apex
- Mid-diastolic rumble at LLSB or apex
ECG
- Superior QRS axis (characteristic)
- RVH and LVH may both be present
CXR
- Cardiomegaly with increased PVMs
5. Pulmonary Stenosis (PS)
Definition
- Obstruction at the level of the pulmonary valve; relatively frequent malformation
- Can be isolated or part of more complex defect (TOF, TGA)
Types
- Valvular PS (most common) - thickened/dysplastic pulmonary valve
- Subvalvular (infundibular) PS - as in TOF
- Supravalvular PS - above the valve
Pathophysiology
- Right ventricular outflow tract obstruction → right ventricular hypertrophy
- Post-stenotic dilation of pulmonary artery (due to high-pressure jet injury)
- With complete atresia: no RV-to-lung communication; blood reaches lungs via PDA only
Clinical Features
- Mild: asymptomatic, compatible with long life
- Moderate-severe: exertional dyspnea, right heart failure
Auscultation
- Ejection click at LUSB (with valvular PS) - click intensity varies with respiration (decreases with inspiration, increases with expiration - pathognomonic of valvular PS)
- S2: widely split with diminished P2
- Systolic ejection murmur (SEM) grade 2-5/6 ± thrill at LUSB, radiating to back and sides
ECG
| PS Severity | ECG |
|---|---|
| Mild | Normal |
| Moderate | RAD + RVH |
| Severe | RAE + RVH with strain |
CXR
- Normal heart size with normal to decreased PVMs (unlike shunt lesions)
- Post-stenotic pulmonary artery dilation may be visible
Management
- Mild: observation
- Moderate-severe: balloon pulmonary valvuloplasty (procedure of choice) or surgical valvotomy
6. Aortic Stenosis (AS)
Types
| Type | Description |
|---|---|
| Valvular AS (most common; 80% isolated) | Hypoplastic, dysplastic, or abnormal number of cusps; bicuspid aortic valve |
| Subaortic (subvalvular) AS | Thickened ring/collar of dense endocardial fibrous tissue below cusps |
| Supravalvular AS | Congenital aortic dysplasia; thickening and constriction of ascending aortic wall; associated with elastin gene mutations |
Pathophysiology
- Left ventricular outflow obstruction → concentric left ventricular hypertrophy
- Severe: hypoplastic LV + ascending aorta → Hypoplastic Left Heart Syndrome (HLHS)
- HLHS: ductus must remain patent; duct closure in first week of life is lethal
Clinical Features
- Generally well tolerated unless severe
- LVH carries risk of sudden cardiac death even in apparently mild disease
- Narrow pulse pressure if severe
Auscultation
- Systolic thrill at RUSB, suprasternal notch, or over carotids
- Ejection click at RUSB (valvular AS) - does NOT vary with respiration
- Harsh SEM grade 2-4/6 at 2nd RICS or 3rd LICS, radiating to neck and apex
- ± early diastolic decrescendo murmur (aortic regurgitation)
- Narrow pulse pressure if severe
ECG
| AS Severity | ECG |
|---|---|
| Mild | Normal |
| Moderate-Severe | LVH ± strain |
CXR
- Usually normal (LV is a pressure-loaded chamber - concentric hypertrophy, not dilation)
7. Coarctation of the Aorta
Definition & Epidemiology
- Narrowing (constriction) of the aorta - ranks high in frequency among structural anomalies
- Occurs in ~10% of children with CHD
- Male:Female = 2:1 (twice as common in males)
- Associated with bicuspid aortic valve in 50-70% of cases
- Associated with Turner syndrome (45,X) in females
- Other associations: berry aneurysms of circle of Willis, ASD, VSD, mitral regurgitation
Location
- Most coarctations occur distal to the origin of the left subclavian artery at the entrance of the ductus arteriosus (juxtaductal)
Types
| Type | Description | Presentation |
|---|---|---|
| Preductal (infantile) | Coarctation proximal to ductus arteriosus; often associated with tubular hypoplasia of aortic arch; PDA is the main source of blood to distal aorta (unoxygenated) | Symptomatic in early childhood; severe CHF at birth if duct closes |
| Postductal (adult) | Discrete ridge-like infolding just opposite the closed ductus (ligamentum arteriosum); collateral circulation develops (intercostal arteries) | Often asymptomatic until adulthood |
Embryological Theories (3 main theories)
- Ductal muscle tissue is incorporated into the aortic wall; when ductus constricts at birth, ductal muscle in aorta also constricts
- Abnormal involution of a small segment of the left dorsal aorta → stenotic segment
- The aortic isthmus (segment between left subclavian and ductus) carries very little blood in fetal life → fails to enlarge normally after ductus closes
Pathophysiology
- Proximal to coarctation: hypertension (upper body, arms)
- Distal to coarctation: hypotension, weak pulses (lower body, legs)
- Collateral circulation via intercostal and internal mammary arteries → delivers blood below obstruction
- Long-standing pressure overload → concentric left ventricular hypertrophy
Clinical Features
- Classic finding: Upper limb hypertension + lower limb hypotension/weak femoral pulses
- Radio-femoral delay (femoral pulse delayed compared to radial)
- Headache, epistaxis (from hypertension)
- Leg claudication (from reduced lower limb perfusion)
- Infants with severe preductal coarctation: closure of PDA causes acute decompensation → prostaglandin E2 infusion used to reopen ductus as emergency measure
Auscultation
- Grade 2-3/6 SEM at left infraclavicular area and/or interscapular area (over the back)
- May have continuous murmur from collateral vessels
ECG
- LVH in older children/adults
CXR (Key Exam Finding)
- "3 sign" or reversed E-sign - indentation of aorta at coarctation site, with pre- and post-stenotic dilation
- Rib notching - erosion of inferior rib margins from dilated intercostal collateral arteries (seen in children >5 years, at ribs 3-8 bilaterally)
Management
- Infants: prostaglandin E2 to maintain PDA patency, then surgical repair
- Older children/adults: balloon angioplasty ± stenting (preferred) or surgical resection with end-to-end anastomosis / prosthetic graft
- Results are excellent with early intervention
Summary Table - Acyanotic CHD at a Glance
(From Harriet Lane Handbook - The Johns Hopkins Hospital)
| Lesion | Key Murmur | ECG | CXR | Classic Feature |
|---|---|---|---|---|
| VSD | 2-5/6 holosystolic at LLSB; ± thrill | Small: normal; Medium: LVH ± LAE; Large: BVH | Cardiomegaly + ↑PVMs | Most common CHD at birth |
| ASD | 2-3/6 SEM at LUSB; wide FIXED split S2 | RBBB with RSR' in V1; RAD | Cardiomegaly + ↑PVMs | Most common CHD in adults |
| PDA | Continuous "machinery" murmur at LUSB | Small-mod: normal/LVH; Large: BVH | Cardiomegaly + ↑PVMs | Wide pulse pressure |
| AVSD | Holosystolic at LLSB ± MR murmur | Superior QRS axis | Cardiomegaly + ↑PVMs | Down syndrome |
| Pulmonary Stenosis | SEM at LUSB ± thrill; ejection click varies with respiration | Mod: RAD+RVH; Severe: RAE+RVH | Normal size; normal/↓PVMs | Click softens on inspiration |
| Aortic Stenosis | Harsh SEM at RUSB; ejection click (no respiratory variation) | Mild: normal; Mod-severe: LVH | Usually normal | Ejection click fixed (no variation) |
| Coarctation of Aorta | SEM at infraclavicular/interscapular | LVH | Rib notching; 3-sign | Upper limb HTN + lower limb hypotension |
Eisenmenger Syndrome (High-Yield Complication)
- Definition: Reversal of a left-to-right shunt to right-to-left due to progressive pulmonary hypertension, resulting in late-onset cyanosis
- Occurs with: large VSD > PDA > ASD (in order of frequency and speed of onset)
- VSD causes Eisenmenger syndrome earlier than ASD due to higher flow volumes and pressure transmitted to pulmonary circulation
- Once established, the shunt cannot be reversed - heart-lung transplant required
- Prevention: Early surgical/catheter-based closure of the defect is the key
Key Points for Exam
- VSD = most common CHD at birth; ASD = most common CHD in adults (because VSDs close spontaneously)
- ASD hallmark auscultatory finding = wide, fixed split S2 (does not vary with respiration)
- PDA = continuous "machinery" murmur + wide pulse pressure; close with indomethacin (premature infants)
- Coarctation = rib notching on CXR + upper limb HTN with radio-femoral delay; associated with bicuspid AorV + Turner syndrome
- AVSD = Down syndrome association; superior QRS axis on ECG
- Pulmonary stenosis ejection click decreases with inspiration (diagnostic of valvular PS)
- Eisenmenger syndrome = late reversal of any left-to-right shunt; VSD most aggressive in causing it
- Indomethacin closes PDA (inhibits prostaglandin); Prostaglandin E2 infusion keeps PDA open (used therapeutically in duct-dependent lesions)
- Supravalvular AS is associated with elastin gene mutations
- Infective endocarditis risk is elevated with small/medium VSDs (jet lesions) and PDA (high-pressure shunts)
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (10th ed.); Robbins & Kumar - Basic Pathology; Harriet Lane Handbook 23rd ed. (Johns Hopkins Hospital); The Developing Human - Clinically Oriented Embryology (Moore & Persaud)
Give me details on Acyanotic heart disease from ghai textbook
Finding Sources
Finding Sources
Finding Sources
Searching the Web
Ghai Essential Pediatrics acyanotic heart disease VSD ASD PDA congenital
Reading Web Page
https://jasu.kg/wp-content/uploads/2024/04/Ghai-Essential-Pe…
Reading Web Page
https://dokumen.pub/ghai-essential-pediatrics-10e-tenth-edit…
Reading Web Page
https://dokumen.pub/ghai-essential-pediatrics-10e-tenth-edit…
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.