Antiarrhythmic Drugs - classify, MOA, theraputic uses adverse effect precautions Propranolol - antiarrhythmic effects, therapeutic uses precautions
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed to compile a thorough answer. Let me write the comprehensive response:
Antiarrhythmic Drugs
Mechanisms of Arrhythmias (Background)
Arrhythmias arise from two basic mechanisms:
-
Abnormal automaticity - Ectopic pacemakers outside the SA node fire at inappropriate rates. Most antiarrhythmics suppress this by blocking Na+ or Ca2+ channels, decreasing the slope of phase 4 (diastolic) depolarization and/or raising the threshold to a less negative voltage.
-
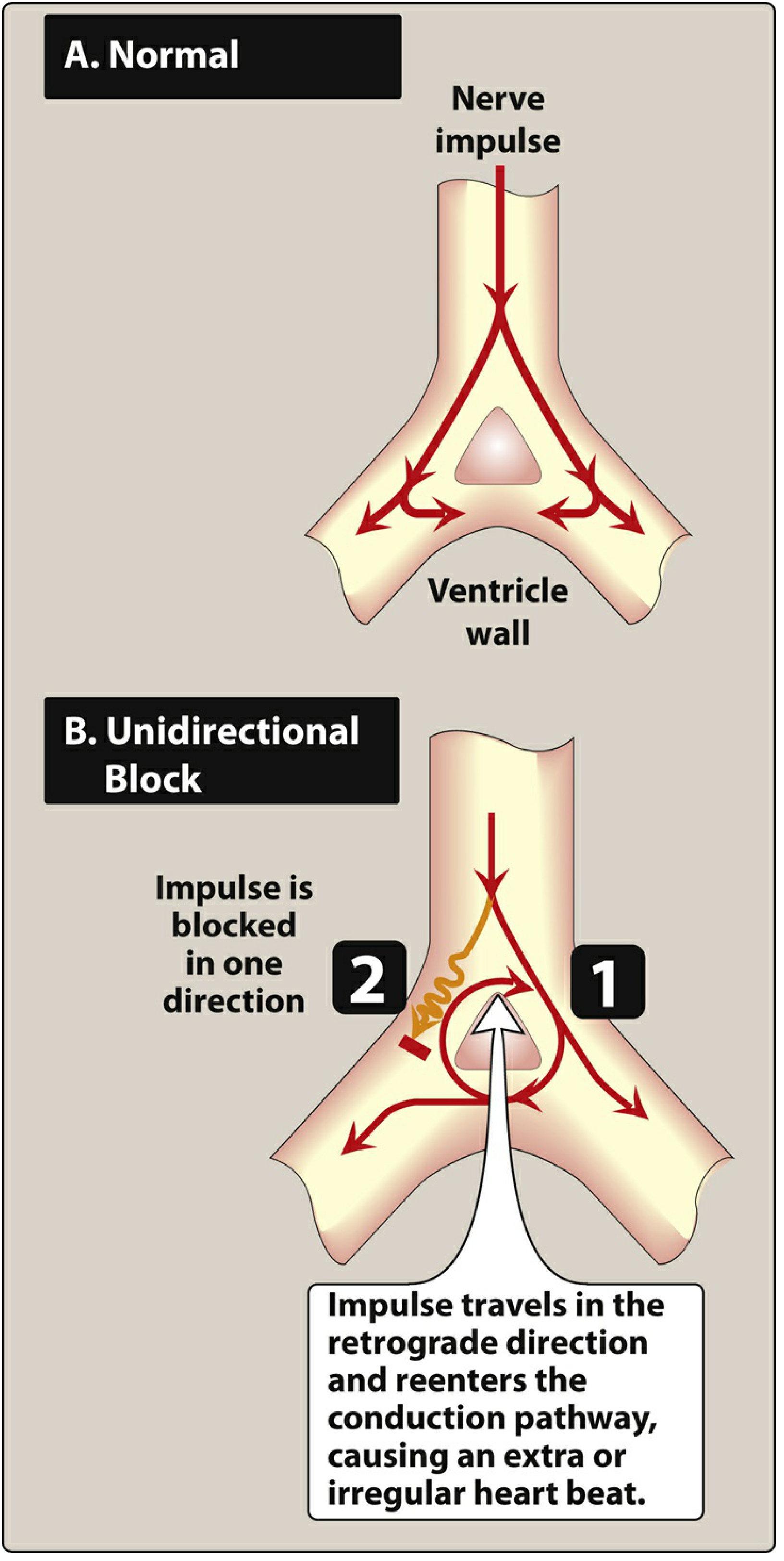
Reentry - The most common cause of arrhythmias. A unidirectional block (from myocardial injury or prolonged refractory period) creates a short-circuit pathway that re-excites cardiac muscle. Class I drugs prevent reentry by slowing conduction; Class III drugs prevent it by increasing the refractory period, both converting a unidirectional block into a bidirectional block.
Vaughan-Williams Classification
The Singh-Vaughan Williams classification groups antiarrhythmic agents by their predominant effect on the cardiac action potential. Note that many drugs have actions spanning more than one class.
CLASS I - Sodium Channel Blockers
All Class I drugs block fast Na+ channels, slowing phase 0 depolarization. They are subdivided based on their effect on repolarization:
Class IA - Na+ Block + K+ Block (Intermediate Dissociation)
Drugs: Quinidine, Procainamide, Disopyramide
MOA:
- Block Na+ channels (open-state dependent) - slow phase 0 depolarization
- Also block K+ channels, prolonging phase 3 repolarization
- Net effect: slow conduction velocity AND prolong action potential duration (APD) / QT interval
- Moderate rate of dissociation from Na+ channels
Therapeutic Uses:
- Atrial fibrillation / flutter (rhythm conversion and maintenance)
- Ventricular tachycardia
- Paroxysmal SVT (quinidine, procainamide)
- WPW syndrome (slows accessory pathway conduction)
Adverse Effects:
- QT prolongation → torsades de pointes (life-threatening)
- Pro-arrhythmia, ventricular arrhythmias
- Acute heart failure, syncope, dizziness
- Quinidine specific: cinchonism (tinnitus, headache, visual disturbances), hemolytic anemia, esophagitis, thrombocytopenia, diarrhea
- Procainamide specific: drug-induced lupus-like syndrome (anti-histone antibodies), hypotension (especially IV)
- Disopyramide specific: strong anticholinergic effects (dry mouth, urinary retention, blurred vision, constipation) - avoid in elderly; potent negative inotrope - avoid in heart failure
Class IB - Na+ Channel Block (Fast Dissociation)
Drugs: Lidocaine, Mexiletine, Phenytoin
MOA:
- Block Na+ channels with preference for inactivated state (ischemic/depolarized tissue)
- Shorten phase 3 repolarization (shorten APD)
- Very rapid dissociation from channels - minimal effect at normal heart rates
- Little effect on normal tissue; selectively suppress ectopic activity in ischemic tissue
Therapeutic Uses:
- Lidocaine: IV treatment of acute ventricular arrhythmias, especially post-MI and digitalis-induced VT; first-line IV agent for acute VT/VF
- Mexiletine: Oral equivalent of lidocaine; chronic ventricular arrhythmias; also used in long QT syndrome (type 3) and myotonic dystrophy
- Phenytoin: Digitalis-induced arrhythmias (historical use)
Adverse Effects:
- CNS toxicity (lidocaine): dizziness, tremor, ataxia, paresthesia, confusion, seizures (dose-dependent)
- Worsening ventricular arrhythmias
- Liver failure (mexiletine)
- Mexiletine: nausea, vomiting, dyspepsia, dysphagia
Class IC - Na+ Channel Block (Slow Dissociation - Marked)
Drugs: Flecainide, Propafenone
MOA:
- Most potent Na+ channel blockers - markedly slow phase 0 depolarization and conduction velocity
- Slow dissociation from Na+ channels → use-dependent block accumulates
- Minimal effect on repolarization
- Propafenone: also has mild beta-blocking and Ca2+ channel blocking properties
Therapeutic Uses:
- Atrial fibrillation / flutter (rhythm control) - well tolerated in patients with structurally normal hearts
- "Pill-in-the-pocket" approach for paroxysmal AF
- Propafenone: also SVT, accessory pathway tachycardias (WPW)
Adverse Effects:
- Bradycardia, QT prolongation, worsening ventricular arrhythmias (pro-arrhythmic)
- Hypotension, heart failure, syncope
- Tremor, headache, visual disturbances, constipation
- CAST Trial Warning: Flecainide/encainide increased mortality in post-MI patients with asymptomatic ventricular ectopy - Class IC drugs are CONTRAINDICATED in structural heart disease (post-MI, LVH, heart failure)
- Propafenone: bronchospasm (beta-blocking effect), hepatic failure, agranulocytosis, anemia, edema
Precaution: Avoid in any patient with structural heart disease.
CLASS II - Beta-Adrenergic Blockers
Drugs: Propranolol, Metoprolol, Atenolol, Esmolol, Carvedilol
MOA:
- Competitively block beta-1 (and beta-2 for non-selective agents) adrenergic receptors
- Inhibit phase 4 (spontaneous diastolic) depolarization in SA and AV nodes
- Decrease SA node automaticity → reduce heart rate
- Slow AV nodal conduction → increase PR interval, reduce ventricular rate in AF/flutter
- Reduce intracellular Ca2+ overload
- Inhibit afterdepolarization-mediated automaticity
- Increase energy required to fibrillate the heart in ischemic tissue
Therapeutic Uses:
- Atrial fibrillation/flutter (rate control)
- SVT - slow or terminate AVNRT
- Prevention of post-MI arrhythmias (proven mortality benefit)
- Ventricular arrhythmias associated with sympathetic excess (exercise-induced, stress-induced)
- Catecholamine-sensitive VT (e.g., CPVT)
- Thyrotoxicosis-related arrhythmias
- Long QT syndrome (beta-blocker is first-line for LQT1 and LQT2)
- Electrical storm (propranolol specifically shown superior to metoprolol)
Adverse Effects:
- Bradycardia, heart block
- Hypotension
- Worsening heart failure (acute decompensation)
- Bronchospasm (especially non-selective agents - avoid in asthma)
- Masking of hypoglycemia symptoms (in diabetics)
- Fatigue, sleep disturbances, depression, sexual dysfunction
- Cold extremities (peripheral vasoconstriction)
- Hyperlipidemia, hypertriglyceridemia
Precautions:
- Caution in asthma/COPD (use cardioselective agents if necessary)
- Avoid in high-degree AV block without pacemaker
- Do NOT abruptly discontinue - withdrawal syndrome (rebound tachycardia, angina, possible MI) due to beta-receptor up-regulation
CLASS III - Potassium Channel Blockers
Drugs: Amiodarone*, Sotalol*, Dronedarone*, Dofetilide, Ibutilide
MOA:
- Block delayed rectifier K+ channels → prolong phase 3 repolarization
- Widen action potential and prolong effective refractory period
- Prolong QT interval
- Prevent reentry by increasing the refractory period
Therapeutic Uses:
- Atrial fibrillation/flutter (rhythm control)
- Ventricular tachycardia/fibrillation
- Amiodarone: Most effective antiarrhythmic overall; used for both AF and life-threatening VT/VF, especially with structural heart disease; safe in heart failure
- Dofetilide/Ibutilide: AF/flutter cardioversion and maintenance
- Sotalol: AF maintenance, ventricular arrhythmias (also has Class II properties)
Adverse Effects (Class III general):
- QT prolongation → torsades de pointes (paradoxically most with dofetilide/ibutilide/sotalol; less with amiodarone)
- Worsening ventricular arrhythmias
Amiodarone-specific (extensive multi-organ toxicity):
- Pulmonary toxicity (pneumonitis, fibrosis) - most serious
- Hepatic failure, transaminitis
- Thyroid dysfunction (hypo- and hyperthyroidism) - contains iodine
- Peripheral neuropathy, paresthesia
- Corneal microdeposits, optic neuritis (visual disturbances)
- Blue-gray skin discoloration (with prolonged use)
- Bradycardia, hypotension
- Drug interactions via CYP450 (inhibits warfarin metabolism, raises digoxin levels)
Precautions:
- Monitor thyroid, liver, and pulmonary function with amiodarone
- Amiodarone has extremely long half-life (~40-55 days) - effects persist months after discontinuation
- Sotalol/dofetilide: dose-adjust in renal impairment; monitor QTc
CLASS IV - Calcium Channel Blockers (Non-Dihydropyridines)
Drugs: Verapamil, Diltiazem
MOA:
- Block L-type Ca2+ channels in SA and AV nodes
- Inhibit phase 0 of the action potential in SA/AV nodal tissue (which is Ca2+-dependent, unlike fast-response tissue)
- Slow SA node automaticity and AV node conduction
- Prolong AV nodal refractory period
Therapeutic Uses:
- Rate control in atrial fibrillation/flutter
- Termination of AVNRT (adenosine preferred first)
- Prevention of AVNRT recurrence
- Verapamil: effective in some idiopathic left VT (verapamil-sensitive VT)
- Inappropriate sinus tachycardia
Adverse Effects:
- Bradycardia, AV heart block
- Acute heart failure / negative inotropic effect (more so with verapamil)
- Peripheral edema, hypotension, dizziness
- Constipation (especially verapamil)
- Gingival hyperplasia (verapamil)
- Gynecomastia, sexual dysfunction
Precautions:
- Avoid verapamil + beta-blocker combination (risk of severe bradycardia/block)
- Contraindicated in WPW with AF (can increase accessory pathway conduction and cause VF)
- Avoid in severe LV dysfunction
Other Antiarrhythmic Agents (Not Formally Classified)
| Drug | MOA | Key Uses |
|---|---|---|
| Adenosine | Activates K+ current in AV node (hyperpolarization); inhibits cAMP-mediated Ca2+ current | Acute termination of AVNRT; diagnosis of SVT; very short half-life (<10 sec) |
| Digoxin | Inhibits Na+/K+-ATPase; enhances vagal tone; slows AV conduction | Rate control in AF (especially with heart failure) |
| Magnesium | Inhibits triggered afterdepolarizations | Torsades de pointes (treatment of choice); digitalis-induced arrhythmias |
PROPRANOLOL - Detailed Focus
Classification
Class II antiarrhythmic - non-selective beta-adrenergic blocker (blocks both beta-1 and beta-2 receptors). The first beta-blocker proven effective in cardiovascular disease.
Antiarrhythmic Effects and MOA
Propranolol's antiarrhythmic actions operate through several mechanisms:
-
Beta-1 receptor blockade at SA node - decreases the slope of phase 4 diastolic depolarization, reducing SA node automaticity and heart rate
-
Beta-1 receptor blockade at AV node - slows AV nodal conduction velocity, prolongs AV nodal refractory period → increases PR interval, limits ventricular rate in AF/flutter
-
Suppression of catecholamine-driven arrhythmias - blocks adrenergic effects on the heart. Beta blockade reduces intracellular Ca2+ overload and inhibits afterdepolarization-mediated automaticity (both DADs and EADs triggered by sympathetic excess)
-
Non-selective beta-2 blockade - prevents epinephrine-induced hypokalemia (mediated via beta-2 receptors), which can be pro-arrhythmic in ischemic states. Propranolol's non-selectivity is actually an advantage here over cardioselective agents
-
Anti-ischemic effect - in acutely ischemic tissue, propranolol increases the energy required to fibrillate the heart, providing additional protection against VF
-
Membrane-stabilizing effect - at high concentrations, propranolol has a direct Na+ channel blocking action (local anesthetic/quinidine-like effect), though this is not thought to be clinically significant at therapeutic doses
The net electrophysiologic effect: decreased automaticity, slowed AV conduction, prolonged AV nodal refractory period with little effect on ventricular myocardium or QT interval.
Therapeutic Uses (Antiarrhythmic)
- Atrial fibrillation/flutter - ventricular rate control
- Paroxysmal SVT (AVNRT, AVRT) - slows or terminates by blocking AV nodal conduction
- Post-myocardial infarction arrhythmias - beta-blockers are the standard of care for preventing ventricular arrhythmias after MI; reduce sudden cardiac death (proven mortality benefit)
- Electrical storm (refractory VT/VF) - non-selective propranolol has shown superiority over metoprolol in one key study, highlighting the benefit of beta-2 blockade in preventing epinephrine-induced hypokalemia
- Exercise-induced/stress-induced ventricular arrhythmias - catecholamine-sensitive tachycardias
- Catecholaminergic polymorphic VT (CPVT) - propranolol is first-line
- Long QT syndrome (LQT1, LQT2) - beta-blockade is the primary medical treatment
- Thyrotoxicosis - controls tachyarrhythmias caused by excess thyroid-driven adrenergic sensitization
- Hypertrophic obstructive cardiomyopathy - controls outflow tract obstruction and associated arrhythmias
- Arrhythmias associated with pheochromocytoma - ONLY after alpha-blockade is established first
Other Therapeutic Uses (Non-Antiarrhythmic)
- Hypertension (decreases cardiac output; inhibits renin release)
- Angina pectoris (reduces O2 demand)
- Migraine prophylaxis
- Essential tremor
- Portal hypertension / variceal bleeding prophylaxis
- Anxiety / situational performance anxiety
- Infantile hemangiomas (topical/oral)
Precautions and Contraindications
| Precaution | Reason |
|---|---|
| Asthma / reactive airway disease | Beta-2 blockade causes bronchoconstriction; use cardioselective agent if absolutely necessary |
| Bradycardia / sick sinus syndrome | Further slows SA node; may cause symptomatic bradycardia |
| High-degree AV block (2nd/3rd) | Worsens AV conduction block; use only if pacemaker in place |
| Decompensated heart failure | Acute negative inotropy; can worsen acute decompensation (though proven beneficial in chronic stable HF) |
| Diabetes mellitus | Masks tachycardia (key warning symptom of hypoglycemia); can blunt hypoglycemia recovery; beta-2 blockade inhibits glycogenolysis |
| Peripheral vascular disease / Raynaud's | Beta-2 blockade causes vasoconstriction, worsening limb ischemia |
| Abrupt withdrawal | Beta-receptor up-regulation during chronic use leads to rebound tachycardia, angina exacerbation, and possible MI on sudden discontinuation - always taper |
| Pheochromocytoma | Never give propranolol without prior alpha-blockade (causes paradoxical hypertension due to unopposed alpha-adrenergic stimulation) |
| WPW syndrome with AF | Beta-blockers are relatively contraindicated; they slow the AV node but do not block accessory pathway conduction (Ca2+ channel blockers also contraindicated) |
| Myasthenia gravis | Beta-blockers can impair neuromuscular junction function |
| Depression | May worsen CNS symptoms - fatigue, depression, sleep disturbances |
| Renal/hepatic impairment | Propranolol is hepatically metabolized; dose may need adjustment in severe hepatic impairment |
Key Clinical Points:
- Propranolol's non-selectivity (beta-1 + beta-2) makes it uniquely effective in catecholamine excess states (pheochromocytoma crisis post-alpha-block, thyroid storm, CPVT, electrical storm) but also makes it riskier in asthmatics and diabetics compared to cardioselective agents like metoprolol
- Among antiarrhythmics, propranolol and beta-blockers as a class have the best survival data post-MI
- In heart failure with AF, amiodarone or dofetilide are preferred for rhythm control; beta-blockers remain useful for rate control in chronic stable HF
- Class IC agents (flecainide, propafenone) are contraindicated where propranolol is often safe - patients with structural heart disease
Sources: Lippincott Illustrated Reviews: Pharmacology; Goodman & Gilman's The Pharmacological Basis of Therapeutics; Katzung's Basic and Clinical Pharmacology, 16th Edition; Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.