Compare neuromuscular transmission Single twitch, train of four,tetanus, double burst , post teatanic count
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I have all the information needed for a comprehensive comparison. Here is the full answer:
Neuromuscular Transmission Monitoring: A Comprehensive Comparison
Peripheral nerve stimulation (PNS) is the standard method for assessing neuromuscular blockade (NMB) during and after anesthesia. Five patterns are used clinically, each suited to different depths of block.
Underlying Principle: Why Fade Occurs
Fade — progressive reduction in twitch height with repeated stimulation — is the hallmark of nondepolarizing block. Nondepolarizing neuromuscular blocking agents (NMBAs) block presynaptic α3β2 nicotinic receptors, impairing the normal mobilization of acetylcholine (ACh) during repetitive stimulation. Each successive stimulus therefore produces less ACh release and a smaller contraction.
Depolarizing block (Phase I) does NOT produce fade — all twitches are equally depressed because the mechanism is sustained end-plate depolarization, not impaired ACh mobilization. Fade with succinylcholine indicates Phase II (desensitization) block.
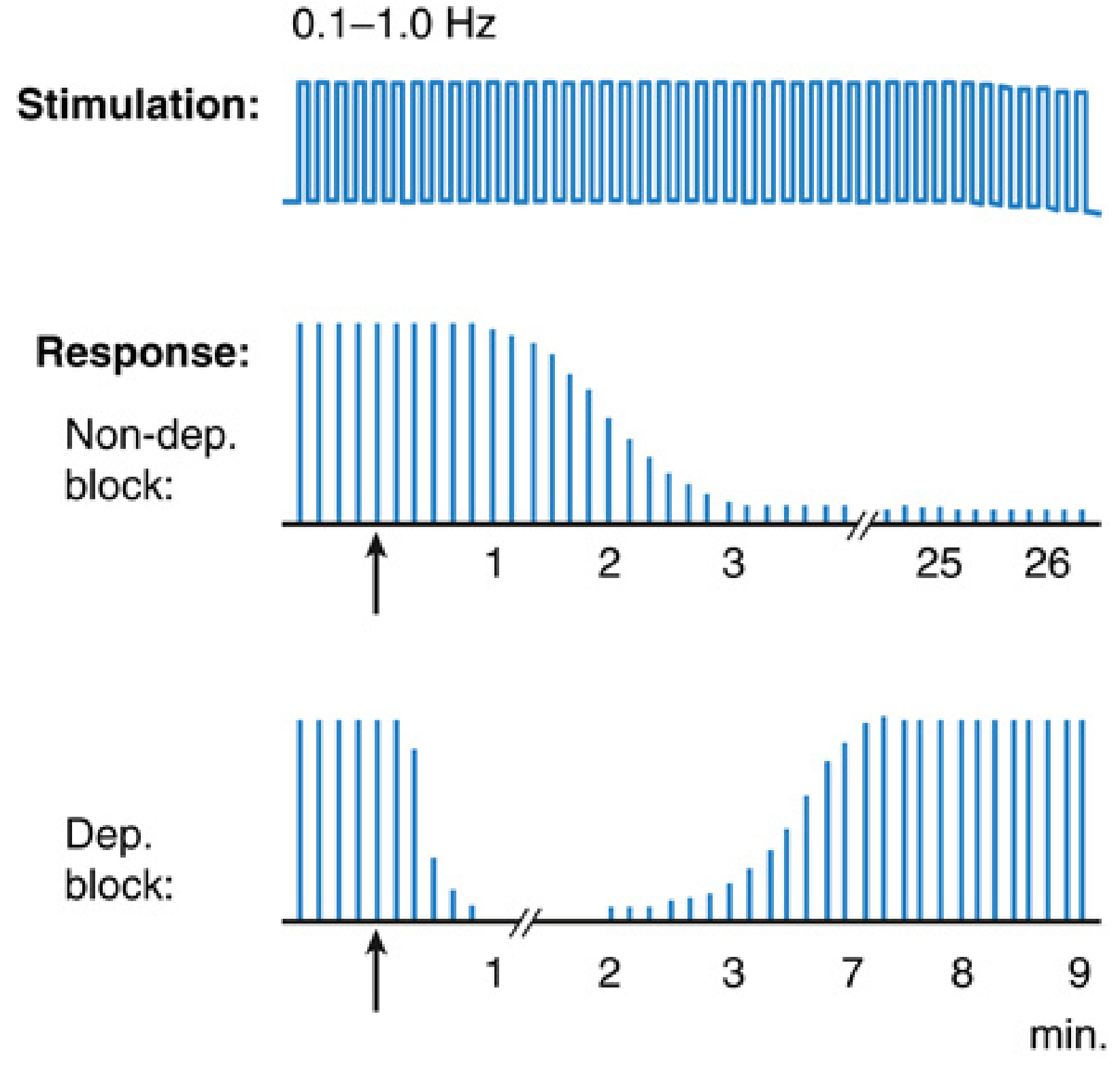
1. Single-Twitch Stimulation
| Feature | Detail |
|---|---|
| Stimulus | Single supramaximal stimulus applied at 0.1–1.0 Hz |
| Measured parameter | Twitch height (T1) compared to pre-drug baseline |
| Response — Non-dep block | Gradual reduction in twitch height; requires baseline for comparison |
| Response — Dep block | Uniform reduction proportional to dose; no fade; no baseline needed for diagnosis |
| Frequency dependency | Rate must be consistent — results at 1 Hz cannot be compared to 0.1 Hz (higher frequency → lower twitch height) |
| Depth of block | Requires ≥75–80% receptor occupancy before twitch height visibly decreases |
| Clinical use | Primarily used as a component within composite patterns (TOF, PTC); rarely used alone now |
| Limitations | Requires a pre-drug baseline; cannot distinguish depolarizing from non-depolarizing without context; least sensitive to partial block |
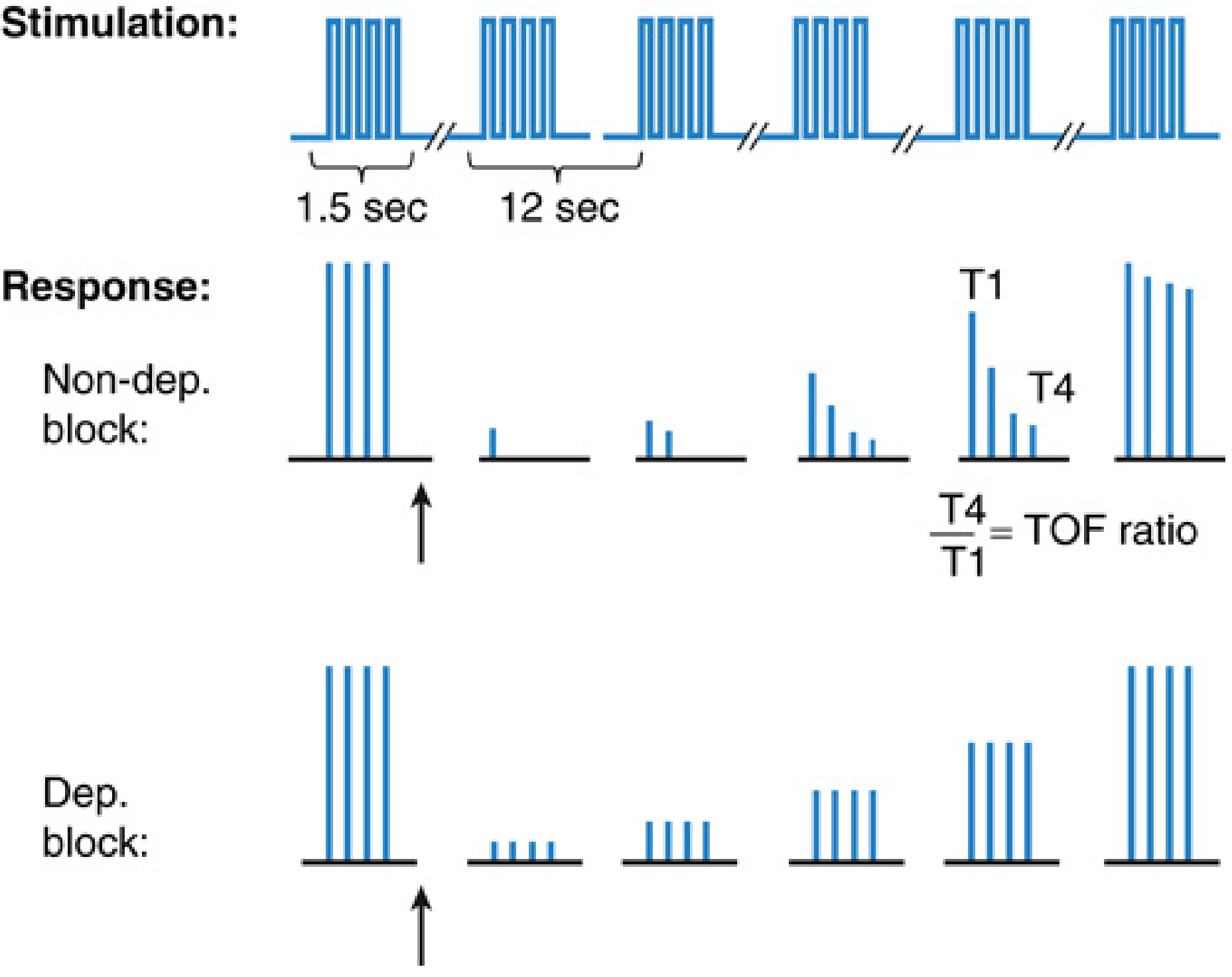
2. Train-of-Four (TOF) Stimulation
| Feature | Detail |
|---|---|
| Stimulus | 4 supramaximal stimuli at 2 Hz (0.5 sec intervals); 1.5-second total train |
| Measured parameter | TOF count (0–4) and TOF ratio (T4/T1) |
| Normal | TOF ratio = 1.0 (all 4 twitches equal) |
| Non-dep block | T4 disappears first → T3 → T2 → T1 as depth increases; recovery in reverse |
| Dep block (Phase I) | All 4 equally and uniformly reduced — no fade; TOF ratio = 1.0 |
| Dep block (Phase II) | Fade develops, mimicking non-dep block |
| TOF count interpretation | 0 twitches = deep block; 1–3 = surgical block; 4 = moderate block |
| TOF ratio and recovery | >0.7 = adequate for spontaneous ventilation; >0.9 = full clinical recovery |
| Key limitation | Subjective (tactile/visual) assessment of fade is only reliable when TOF ratio < 0.4; the "blind zone" of TOF ratio 0.4–0.9 represents undetected residual paralysis |
| Repeat interval | ≥10–15 seconds between trains to avoid artefactual fade |
| Advantage over single twitch | No baseline needed; works across all phases of block; most widely used pattern |
3. Tetanic Stimulation
| Feature | Detail |
|---|---|
| Stimulus | Rapid repetitive stimulation at 50 Hz (standard) or 100 Hz for 5 seconds |
| Normal response | Sustained, unfading contraction throughout 5 seconds |
| Non-dep block | Fade — contraction is not sustained; strength decreases during stimulus |
| Dep block (Phase I) | No fade — sustained contraction |
| Dep block (Phase II) | Fade present |
| Sensitivity | More sensitive than TOF for detecting residual block. 50 Hz ≈ TOF fade (detects TOF ratio <0.4); 100 Hz detects TOF ratio ≈ 0.85 — most sensitive subjective assessment |
| Important caveat | 100 Hz can produce physiologic fade in fully recovered patients; fade at this frequency may be misleading |
| Post-tetanic potentiation | Tetany causes a massive ACh release → temporarily improves subsequent twitch responses (exploited by PTC, see below) |
| Repeat interval | ≥2 min after 50-Hz tetany; ≥3 min after 100-Hz tetany — tetanic stimulation influences subsequent monitoring |
| Clinical use | Component of PTC; used in awake patients to confirm reversal (painful) |
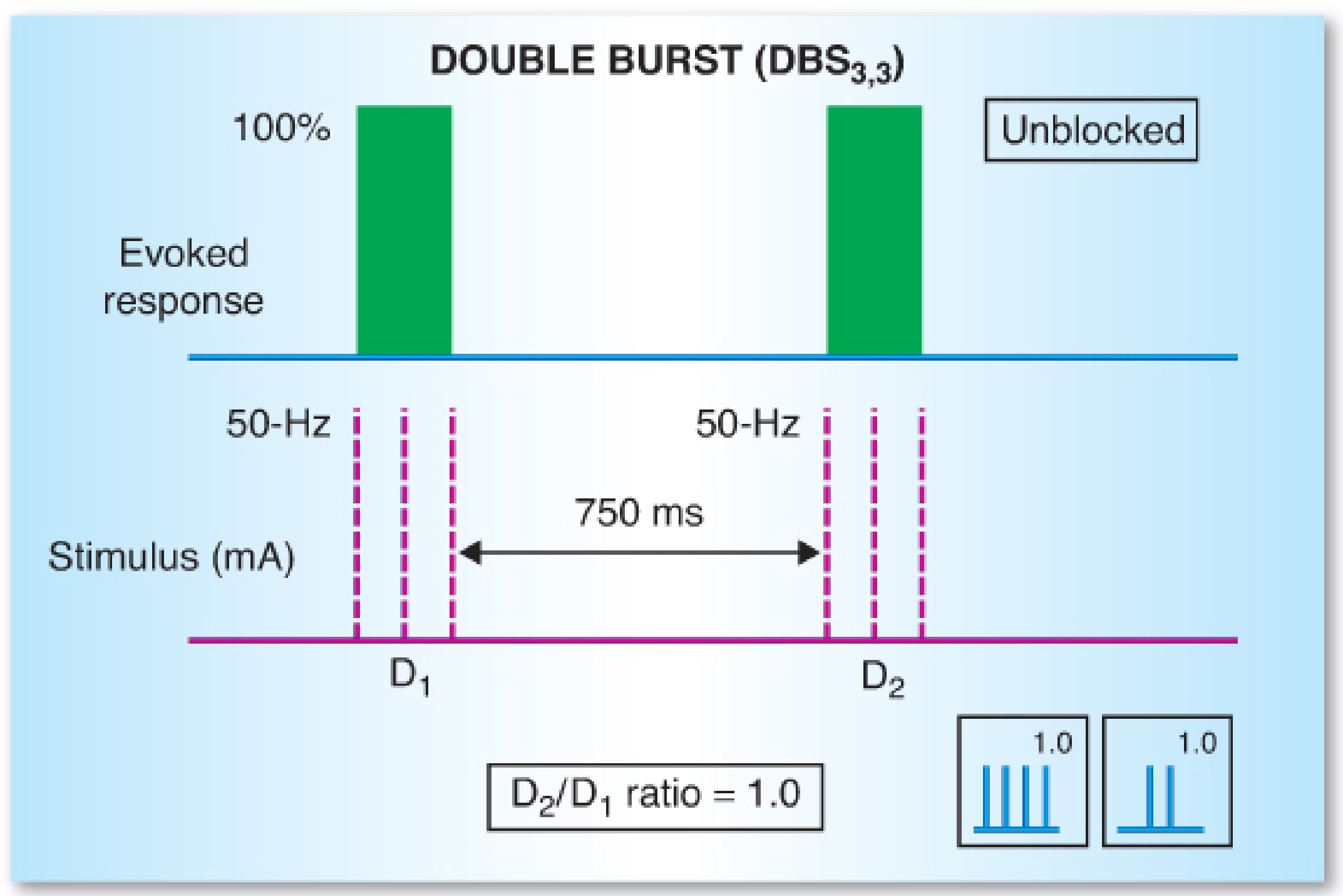
4. Double Burst Stimulation (DBS)
| Feature | Detail |
|---|---|
| Stimulus | Two short bursts of 50-Hz tetanic stimuli separated by 750 ms |
| Most common form | DBS₃,₃ — two bursts of 3 stimuli (60 ms each at 50 Hz) |
| Alternative | DBS₃,₂ — first burst of 3 stimuli, second of 2 |
| Perceived response | Two distinct muscle twitches (each burst fuses into one contraction) |
| Measured parameter | D2/D1 ratio (analogous to TOF ratio) |
| Rationale | Comparing only 2 responses (D1 vs D2) is perceptually easier than comparing T1 vs T4 across 4 twitches in TOF |
| Non-dep block | D2 < D1 (fade between the two twitches) |
| Dep block | D1 = D2 (no fade) |
| Sensitivity | Slightly more sensitive than TOF for subjective fade detection, but still cannot reliably detect TOF ratio between 0.6 and 0.9 — residual paralysis may still go undetected |
| Advantage over TOF | Better tolerated than tetany by awake patients; easier subjective comparison than 4-twitch TOF |
| Repeat interval | ≥20 seconds between assessments |
| Limitation | Still insufficient to exclude residual paralysis without objective monitoring |
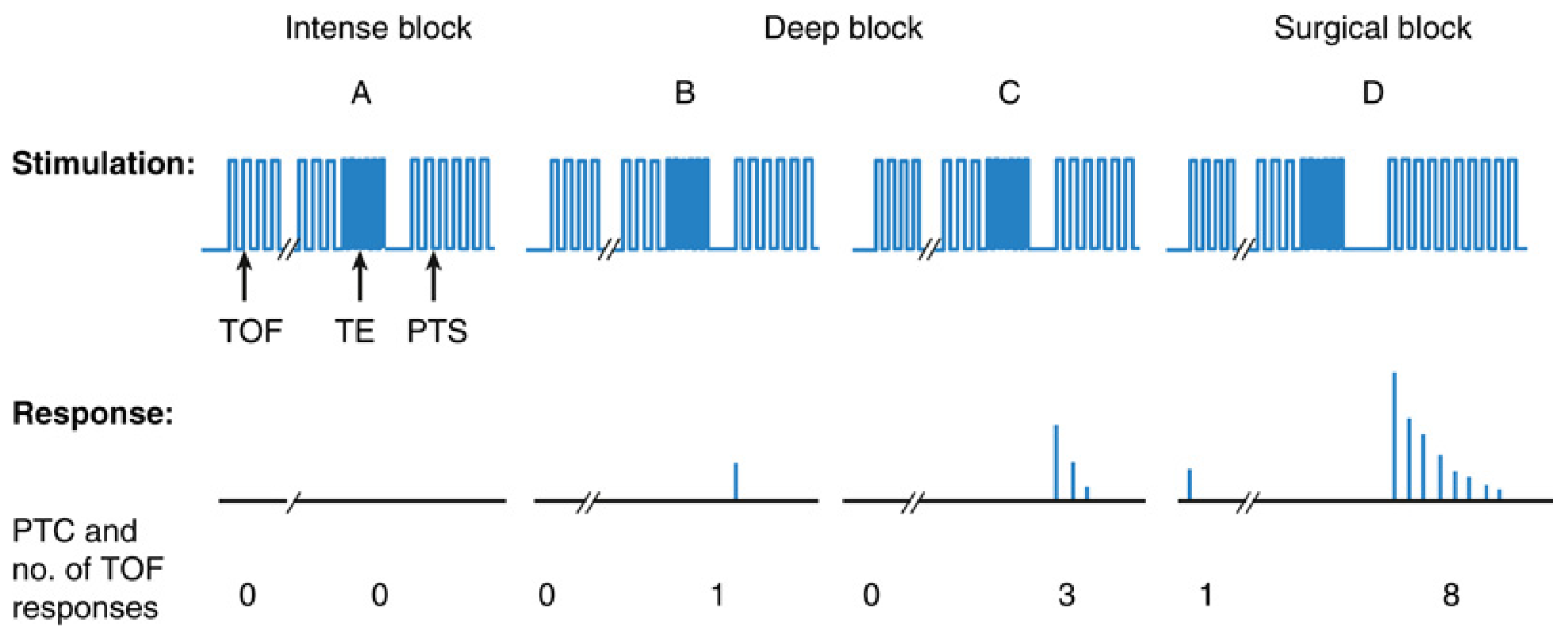
5. Post-Tetanic Count (PTC)
| Feature | Detail |
|---|---|
| Stimulus sequence | 50-Hz tetanic stimulation for 5 seconds → 3-second pause → 15–20 single twitches at 1 Hz |
| Measured parameter | Number of post-tetanic twitches observed (the PTC) |
| Principle | Tetany causes massive transient ACh release (post-tetanic potentiation) → even with no TOF response, brief facilitated twitches occur |
| Use | Only reliable method to quantify intense and deep block (TOF count = 0) |
| Interpretation | PTC 0 = intense block (no imminent TOF); PTC 1–2 = very deep; PTC 3–5 = deep; PTC 6–10 = TOF return imminent; PTC ≥ 8–10 → T1 of TOF will reappear soon |
| Non-dep block only | Not applicable for depolarizing block |
| Repeat interval | ≥2–3 minutes — tetanic stimulation must not be repeated sooner |
| Clinical use | Guides dosing of maintenance NMBA when complete block is required (e.g., intraocular surgery, open airway surgery, laparoscopy); deeper block management during sugammadex reversal planning |
Summary Comparison Table
| Feature | Single Twitch | TOF | Tetanus | DBS | PTC |
|---|---|---|---|---|---|
| Frequency | 0.1–1.0 Hz | 2 Hz (×4) | 50–100 Hz | 50 Hz (×2 bursts) | 50 Hz→1 Hz |
| No. of stimuli | 1 | 4 | Continuous | 3+3 (or 3+2) | 5 s burst + 15–20 |
| Baseline needed? | Yes | No | No | No | No |
| Non-dep fade? | No (just reduced) | Yes (T4 first) | Yes | Yes (D2 < D1) | N/A |
| Dep Phase I fade? | No | No | No | No | N/A |
| Depth detectable | Moderate–surgical | Surgical–moderate | Moderate–surgical | Moderate–surgical | Intense & deep (TOF=0) |
| Blind zone | All partial block | TOF 0.4–0.9 | TOF 0.4–0.85 | TOF 0.6–0.9 | None at deep block |
| Recovery endpoint | ≥25% T1 baseline | TOF ratio >0.9 | Sustained contraction | D2/D1 → 1.0 | Return of TOF |
| Repeat interval | Any | 10–15 sec | 2–3 min | 20 sec | 2–3 min |
| Painful (awake pt)? | Mild | Mild | Yes | Less than tetanus | Yes (tetanic component) |
Key Clinical Pearls
- TOF is the workhorse — used throughout all phases; TOF ratio >0.9 is the gold standard for full recovery but requires objective (acceleromyographic) measurement, not subjective assessment.
- PTC is essential for intense/deep block — when no TOF response is present, PTC is the only way to gauge depth.
- DBS is the subjective upgrade over TOF — it slightly improves manual fade detection but still cannot exclude residual paralysis (TOF ratio 0.6–0.9 remains undetectable).
- Tetanus is most sensitive subjectively (100 Hz ≈ TOF ratio 0.85) but risks physiologic fade and interferes with subsequent monitoring.
- Depolarizing (Phase I) block never fades — its hallmark is uniform symmetric depression across all stimulation modes; fade signals Phase II.
Sources: Miller's Anesthesia, 10e (Chapter 39); Barash's Clinical Anesthesia, 9e (Chapter 21); Katzung's Basic and Clinical Pharmacology, 16e (Chapter 27)
This is a shared conversation. Sign in to Orris to start your own chat.