I now have all the content needed from the textbooks. Let me compile the complete, comprehensive teaching guide:
CONGESTIVE HEART FAILURE (CHF)
A Complete Exam-Oriented Clinical Teaching Guide
1. DEFINITION
One-line exam definition:
Congestive Heart Failure is a clinical syndrome in which the heart is unable to pump sufficient blood to meet the metabolic demands of the body, or can only do so at elevated filling pressures, leading to congestion of the pulmonary and/or systemic circulation.
Simple explanation:
Think of the heart as a pump. In CHF, this pump becomes weak (systolic failure - can't squeeze) OR stiff (diastolic failure - can't relax and fill). The result: blood backs up behind the failing ventricle causing congestion (fluid buildup in lungs and body), and forward flow drops causing poor organ perfusion (fatigue, kidney failure). The body tries to compensate through the sympathetic nervous system and RAAS - but these compensatory mechanisms ultimately make things worse.
Exam tip: "Congestive" = fluid congestion from backup pressure. The heart fails forward (low output) AND backward (raised venous pressure).
2. CAUSES (ETIOLOGY)
Common Causes
| Category | Left-Sided HF | Right-Sided HF |
|---|
| Ischemic | IHD / MI (most common cause overall) | Secondary to left HF (most common) |
| Hypertensive | Systemic hypertension | Pulmonary hypertension |
| Valvular | Mitral regurgitation, Aortic stenosis, Aortic regurgitation | Tricuspid regurgitation, Pulmonary stenosis |
| Cardiomyopathy | Dilated cardiomyopathy | Cor pulmonale |
| Inflammatory | Myocarditis, Endocarditis | - |
| Arrhythmia | AF with rapid ventricular rate | - |
| Congenital | VSD, PDA | ASD, Eisenmenger syndrome |
Important Risk Factors
- Hypertension (single most prevalent risk factor)
- Coronary artery disease / prior MI
- Diabetes mellitus
- Obesity
- Atrial fibrillation
- Valvular heart disease
- Alcohol abuse (alcoholic cardiomyopathy)
- Chemotherapy (anthracyclines - doxorubicin)
- Family history / genetic cardiomyopathy
- Sleep apnea
High-output failure (rare but examinable)
Causes: Hyperthyroidism, Beriberi (Vit B1 deficiency), severe anemia, AV fistula, Paget's disease. Heart works harder than normal but can't meet demands.
3. TYPES / CLASSIFICATION
A. By Ejection Fraction (Most Clinically Used)
| Type | EF | Description | Common Causes |
|---|
| HFrEF (Heart Failure with Reduced EF) | <40% | Systolic dysfunction - pump can't squeeze | MI, dilated CMP, alcohol |
| HFmrEF (Mildly Reduced EF) | 40-49% | "Grey zone" - intermediate | Mixed |
| HFpEF (Heart Failure with Preserved EF) | ≥50% | Diastolic dysfunction - heart can't relax/fill | HTN, DM, obesity, elderly |
Key point: Normal EF is >60%. HFpEF is increasingly common, especially in elderly hypertensive women.
B. By Side of Failure
| Type | Congestion Site | Key Features |
|---|
| Left-sided HF | Lungs (pulmonary congestion) | Dyspnea, orthopnea, PND, crackles |
| Right-sided HF | Systemic (venous congestion) | JVD, pitting edema, hepatomegaly, ascites |
| Biventricular HF | Both | All features combined |
C. By Onset
- Acute HF - sudden onset (e.g., flash pulmonary edema after MI)
- Chronic HF - gradual onset with compensation
D. NYHA Functional Classification (Exam Favorite)
| Class | Symptoms | Description |
|---|
| I | None | Cardiac disease but no symptoms with ordinary activity |
| II | Mild | Comfortable at rest; slight limitation with ordinary activity |
| III | Moderate | Comfortable at rest; marked limitation with less-than-ordinary activity |
| IV | Severe | Symptoms at rest; unable to carry on any activity without discomfort |
4. PATHOPHYSIOLOGY
Step-by-Step Flowchart
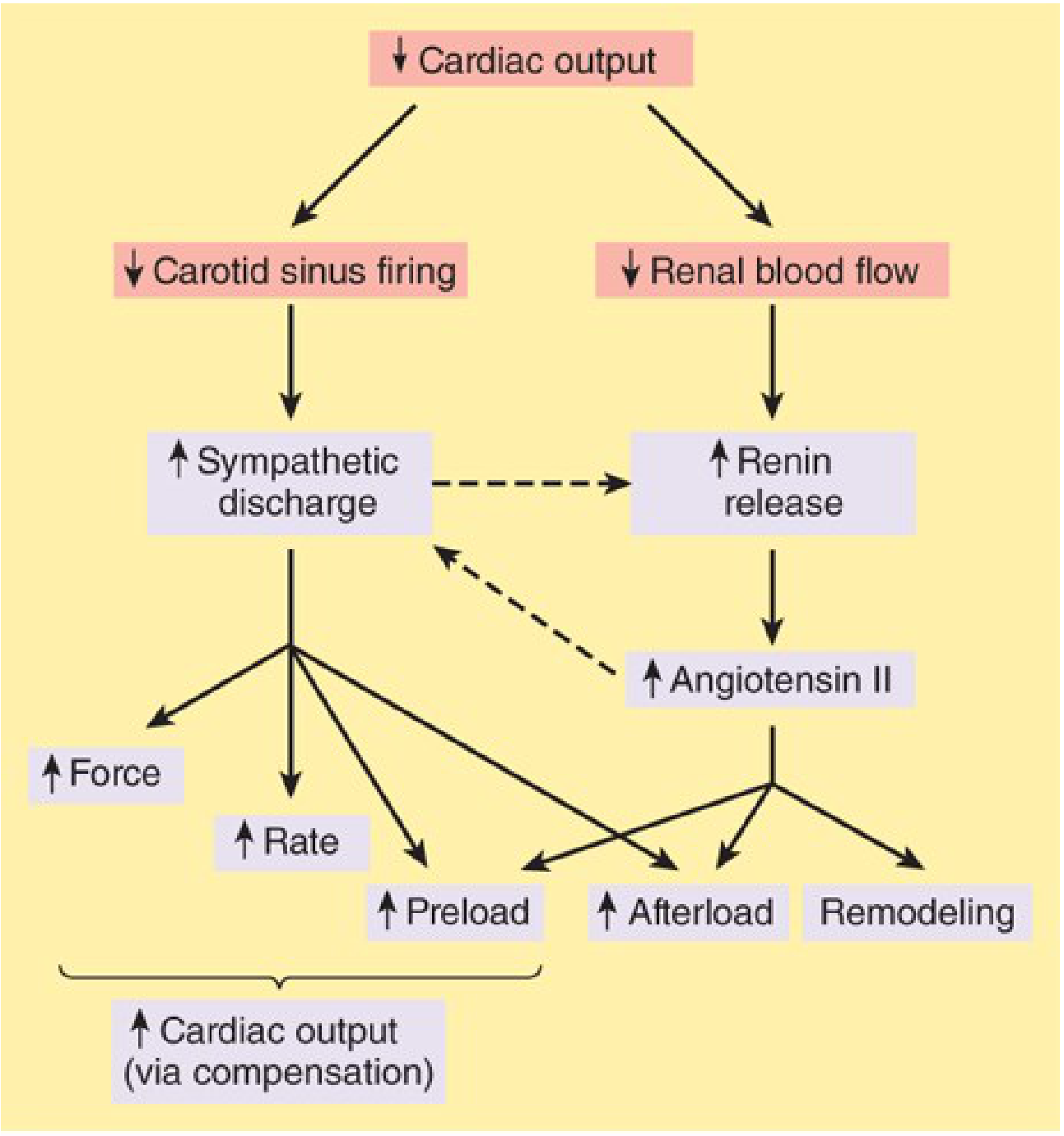
Here is the compensatory neurohumoral response in CHF (from Katzung's Basic and Clinical Pharmacology, 16th Ed.):
Simplified Pathophysiology Flowchart
INITIAL MYOCARDIAL INJURY (MI, HTN, cardiomyopathy)
↓
↓ Cardiac Output (CO)
↙ ↘
↓ Carotid sinus ↓ Renal blood flow
firing ↓
↓ ↑ Renin → ↑ Angiotensin II
↑ Sympathetic ↓
discharge ↑ Aldosterone → Na+ & H2O retention
↓ ↓
↑ HR, ↑ Contractility ↑ Preload (fluid overload)
↑ Vasoconstriction → ↓
↑ Afterload Pulmonary & Systemic Congestion
↓
FURTHER ↓ in CO (vicious cycle)
↓
Cardiac REMODELING (hypertrophy → dilation)
↓
Myocyte apoptosis → Worsening failure
Why the Compensation Fails:
- Sympathetic overstimulation → Beta-1 receptor downregulation → reduced response + arrhythmias
- Angiotensin II → vasoconstriction + aldosterone release → more fluid retention = worse congestion
- Cardiac hypertrophy → initially helps, but capillary density doesn't increase proportionally → ischemia of hypertrophied muscle → fibrosis → reduced function
- Ventricular remodeling → pathological dilation → mitral regurgitation from papillary muscle displacement → further worsens function
Morphological Changes (Robbins Pathology):
- Left heart failure: LV hypertrophy + dilation, LA dilation, pulmonary edema, "heart failure cells" (hemosiderin-laden macrophages) in lungs
- Right heart failure: RV hypertrophy + dilation, hepatomegaly (nutmeg liver), peripheral edema, ascites, pleural effusions
5. CLINICAL FEATURES
Left-Sided Heart Failure (Pulmonary Congestion)
| Symptom | Why It Occurs |
|---|
| Dyspnea on exertion (DOE) | Pulmonary congestion → interstitial edema → reduced lung compliance → increased work of breathing |
| Orthopnea | When supine, venous return increases → more blood enters already-congested pulmonary circulation → worse dyspnea when lying flat. Relieved by sitting up (2-3 pillow orthopnea) |
| Paroxysmal Nocturnal Dyspnea (PND) | Patient wakes 1-3 hours after sleeping, gasping. Fluid redistribution when supine causes acute pulmonary edema. HIGHLY SPECIFIC for left HF |
| Cough | Pulmonary congestion; can be pink/frothy in acute pulmonary edema |
| Fatigue & weakness | Low cardiac output → reduced skeletal muscle perfusion |
| Nocturia | At rest, redistributed fluid mobilized → increased renal perfusion → increased urine output at night |
Signs of Left HF:
- Tachycardia (compensatory)
- Displaced apex beat (cardiomegaly)
- S3 gallop (volume overload, most specific sign of systolic HF)
- S4 gallop (stiff ventricle, diastolic HF)
- Functional mitral regurgitation murmur (pansystolic)
- Bilateral basal crackles (fine, crepitations) - don't clear with coughing
- Cheyne-Stokes respiration (in severe HF)
Right-Sided Heart Failure (Systemic Venous Congestion)
| Symptom/Sign | Why It Occurs |
|---|
| Raised JVP (Jugular Venous Pressure) | Venous blood cannot drain into right heart → backs up into jugular veins |
| Hepatomegaly | Blood backs up into hepatic veins → "nutmeg liver" / congestive hepatopathy; tender hepatomegaly |
| Pitting pedal edema | Raised venous pressure → fluid transudation into interstitium (dependent areas - ankles first, then legs) |
| Ascites | Portal hypertension from hepatic congestion |
| Anorexia/Nausea | Gut congestion → bowel edema |
Biventricular HF: All of the above combined
6. KEY SYMPTOMS THAT SUGGEST THE DIAGNOSIS
Hallmark Symptom
Orthopnea + Paroxysmal Nocturnal Dyspnea (PND) = almost pathognomonic for left-sided HF
Classic Clinical Triad (Exam):
- Dyspnea (exertional, then at rest)
- Orthopnea (needs 2-3 pillows to sleep)
- Bilateral ankle edema
Classic Clinical Clues
- History of MI / HTN / valve disease
- S3 gallop on auscultation (most specific physical sign)
- Raised JVP + bilateral crackles + ankle edema = classic presentation
- Displaced apex beat (cardiomegaly)
- Hepatojugular reflux (HJR) - pressing on liver raises JVP
Red Flag Findings (Acute Decompensation)
- Pink frothy sputum = acute pulmonary edema (emergency!)
- SpO2 <90% on room air
- Resting tachycardia >120 bpm
- BP drop (cardiogenic shock)
- Altered mental status (cerebral hypoperfusion)
- Oliguria/anuria (renal failure from reduced perfusion)
7. LABORATORY INVESTIGATIONS
| Investigation | Expected Finding | Clinical Significance |
|---|
| CBC | Anemia (normocytic or microcytic) | Anemia worsens HF (high-output state); exclude as precipitant |
| CBC | Leukocytosis | Suggests infection as precipitant |
| Serum Na+ | Hyponatremia (<135) | Poor prognosis; dilutional from water retention via ADH |
| Serum K+ | Hypo or Hyperkalemia | Hypokalemia from diuretics; Hyperkalemia from ACE-i/ARBs/spironolactone - important before starting drugs |
| Serum Creatinine / BUN | Elevated (prerenal azotemia) | Reduced renal perfusion; BUN:Cr ratio >20:1 |
| LFTs | Elevated AST/ALT/ALP | Congestive hepatopathy from RHF |
| Blood glucose / HbA1c | Elevated | DM as etiology/risk factor |
| Thyroid Function (TSH) | Low TSH (hyperthyroidism) or High TSH (hypothyroid) | Both can cause/worsen HF |
| BNP (B-type Natriuretic Peptide) | >400 pg/mL = HF likely; <100 = HF unlikely | Most important biomarker for HF diagnosis. Released by ventricles under stretch/stress. Class I recommendation for diagnosis and prognosis |
| NT-proBNP | >900 pg/mL (age <75); >1800 (age >75) | More sensitive than BNP; longer half-life; used for same purpose |
| Troponin-I/T | Elevated in acute MI precipitating HF | Rule out ACS as precipitant |
| ABG | Respiratory alkalosis (early) → Metabolic acidosis (late) | Early: hyperventilation from pulmonary edema. Late: poor perfusion → lactic acidosis |
| ECG | LVH, AF, Q waves (prior MI), LBBB, ST changes | Identifies arrhythmias, prior MI, conduction disease |
| Chest X-ray (CXR) | Cardiomegaly (CTR >0.5), Kerley B lines, cephalization of vessels, bilateral perihilar "bat wing" opacity, pleural effusion | "Bat wing" = acute pulmonary edema; Kerley B = interstitial edema; cephalization = redistribution of blood to upper lobes |
| Echocardiogram (TTE) | Reduced EF (<40% in systolic HF), wall motion abnormalities, LV dilation, valve pathology, diastolic dysfunction parameters | Gold standard to confirm diagnosis, classify type, assess severity, and guide treatment |
| Coronary Angiogram | Coronary artery obstruction | If ischemic etiology suspected; guides revascularization |
| Urine output | Oliguria | Reduced GFR from low CO |
Exam Pearl: BNP is the single most important blood test to order when CHF is suspected. It distinguishes cardiac dyspnea (high BNP) from pulmonary dyspnea (low/normal BNP).
8. DIFFERENTIAL DIAGNOSIS
| Disease | Similar Features | Differentiating Features |
|---|
| COPD/Asthma | Dyspnea, cough, wheeze | No JVP rise, no S3, no Kerley B lines; FEV1/FVC reduced; responds to bronchodilators; BNP normal |
| Pulmonary Embolism | Dyspnea, tachycardia, hypoxia | Sudden onset, pleuritic chest pain, no cardiomegaly; D-dimer elevated; CT-PA shows filling defect; BNP usually normal or mildly elevated |
| Pneumonia | Dyspnea, crackles, hypoxia | Fever, productive cough, lobar consolidation on CXR, leukocytosis, no cardiac history; BNP normal |
| Cardiac Tamponade | Raised JVP, hypotension, dyspnea | Beck's triad (raised JVP + hypotension + muffled heart sounds); pulsus paradoxus; no pulmonary edema; echo shows pericardial effusion |
| Nephrotic Syndrome | Pitting edema, ascites | Massive proteinuria (>3.5g/day), hypoalbuminemia, no raised JVP, no crackles, BNP normal |
| Cirrhosis | Ascites, ankle edema | Spider nevi, jaundice, palmar erythema, history of alcohol; no raised JVP; BNP normal |
| Constrictive Pericarditis | Raised JVP, edema, ascites | Kussmaul's sign (JVP rises on inspiration), pericardial knock on auscultation; CT shows pericardial calcification |
| Hypoalbuminemia (any cause) | Pitting edema | No raised JVP, no pulmonary crackles, low serum albumin |
9. SHORT CLINICAL CASES
Case 1 - Acute Decompensated Left HF
"A 68-year-old male with known hypertension and previous MI presents to the ED at 2 AM with sudden onset breathlessness that woke him from sleep. He can only sleep on 3 pillows. On examination: RR 32/min, SpO2 84%, BP 180/100 mmHg, HR 112/min. Auscultation reveals bilateral crackles up to mid-zones, S3 gallop, and a displaced apex beat. CXR shows cardiomegaly with bilateral perihilar 'bat-wing' opacities. BNP = 1450 pg/mL."
Diagnosis: Acute Decompensated Left-Sided Heart Failure (HFrEF) with Acute Pulmonary Edema
Reasoning:
- Paroxysmal nocturnal dyspnea (woke at 2 AM) + orthopnea (3 pillows) = classic left HF
- Bilateral crackles + S3 = pulmonary congestion + volume overload
- CXR "bat-wing" = acute pulmonary edema
- BNP markedly elevated confirms cardiac cause
- Hypertension + prior MI = known risk factors and likely precipitant
Case 2 - Right-Sided HF / Cor Pulmonale
"A 62-year-old male with 40-pack-year smoking history presents with progressive swelling of both legs for 3 months, abdominal distension, and decreased appetite. On examination: JVP raised 6 cm above sternal angle, pitting edema up to the knees bilaterally, tender hepatomegaly 3 cm below the costal margin. CXR shows hyperinflated lungs with right ventricular prominence. Echo shows RV dilation with RVSP of 55 mmHg. BNP = 480 pg/mL."
Diagnosis: Right-Sided Heart Failure secondary to Cor Pulmonale (COPD-related pulmonary hypertension)
Reasoning:
- Heavy smoker + hyperinflated lungs = COPD
- COPD → pulmonary hypertension → RV strain → RV failure
- JVD + hepatomegaly + pitting edema = classic right HF triad
- No pulmonary edema / crackles = not primarily left-sided
- Elevated RVSP on echo confirms pulmonary hypertension
10. TREATMENT
A. Non-Pharmacological Treatment
| Intervention | Details |
|---|
| Salt restriction | <2g sodium/day; reduces fluid retention |
| Fluid restriction | 1.5-2 L/day in severe/symptomatic HF |
| Weight monitoring | Daily weight; >2 kg gain in 2 days = alert for fluid accumulation |
| Cardiac rehabilitation | Supervised exercise program for stable NYHA Class I-III improves exercise tolerance and QoL |
| Treat underlying cause | Revascularization for ischemic HF; valve repair/replacement for valvular disease |
| Smoking cessation | Mandatory |
| Alcohol cessation | Mandatory (esp. alcoholic cardiomyopathy) |
| Vaccination | Influenza + pneumococcal vaccines to prevent cardiac decompensation |
| Device therapy | ICD (if EF <35% to prevent SCD); CRT (if LBBB + EF <35% + NYHA II-III to resynchronize ventricles) |
| Cardiac transplant | End-stage HF refractory to all treatment (EF <20%, NYHA IV) |
B. Pharmacological Treatment
Drug of Choice (DOC): ACE inhibitor + Beta blocker + Mineralocorticoid Receptor Antagonist (MRA) = the neurohormonal "triple therapy" backbone for HFrEF. SGLT2 inhibitors are now added as the 4th pillar.
| Drug | Drug Group | Mechanism of Action | Indication | Dose | Major Adverse Effects |
|---|
| Furosemide (Frusemide) | Loop Diuretic | Inhibits Na-K-2Cl transporter in thick ascending limb of loop of Henle → massive natriuresis and diuresis | Symptomatic relief of fluid overload; acute pulmonary edema (IV) | PO: 20-80 mg/day; IV: 40-200 mg in acute HF | Hypokalemia, hyponatremia, ototoxicity (high dose IV), dehydration, hyperuricemia |
| Enalapril / Ramipril | ACE Inhibitor | Blocks conversion of Ang I → Ang II → reduces vasoconstriction, aldosterone release, and cardiac remodeling | HFrEF (EF <40%) - reduces mortality, hospitalizations, and progression; all NYHA classes | Enalapril: 2.5-20 mg BD; Ramipril: 2.5-10 mg OD | Dry cough (bradykinin accumulation - most common reason to switch to ARB), hyperkalemia, angioedema (rare, switch to ARB), hypotension, acute kidney injury |
| Losartan / Valsartan / Candesartan | ARB (Angiotensin Receptor Blocker) | Blocks AT1 receptor → vasodilation, reduced aldosterone, anti-remodeling; no bradykinin accumulation | Alternative to ACE-i when cough/angioedema occurs | Losartan: 25-100 mg OD; Candesartan: 4-32 mg OD | Hyperkalemia, hypotension, renal impairment; NO cough |
| Sacubitril/Valsartan (Entresto) | ARNI (Angiotensin Receptor-Neprilysin Inhibitor) | Valsartan blocks AT1 receptor; Sacubitril inhibits neprilysin → prevents degradation of natriuretic peptides → vasodilation, natriuresis | Superior to ACE-i for HFrEF (PARADIGM-HF trial); NYHA II-III; replaces ACE-i/ARB | 24/26 mg - 97/103 mg BD | Hypotension, hyperkalemia, angioedema (avoid with ACE-i; washout 36 hrs before starting) |
| Carvedilol / Bisoprolol / Metoprolol succinate | Beta Blocker (Cardioselective or Non-selective) | Blocks beta-1 (and beta-2 for carvedilol) receptors → reduces HR, reduces sympathetic-driven remodeling, anti-arrhythmic, reverses beta-receptor downregulation | HFrEF; reduces sudden cardiac death; start LOW, go SLOW | Carvedilol: 3.125-25 mg BD; Bisoprolol: 1.25-10 mg OD | Bradycardia, hypotension, worsen acute decompensated HF (never start in wet/decompensated HF!), fatigue, bronchospasm (carvedilol) |
| Spironolactone / Eplerenone | Mineralocorticoid Receptor Antagonist (MRA) | Aldosterone receptor blockade → reduces Na+/water retention, reduces cardiac fibrosis and remodeling | HFrEF with EF <35%; NYHA III-IV; reduces mortality (RALES trial) | Spironolactone: 25-50 mg OD | Hyperkalemia (monitor K+ closely!), gynecomastia (spironolactone - switch to eplerenone), renal impairment |
| Dapagliflozin / Empagliflozin | SGLT2 Inhibitor | Inhibits sodium-glucose co-transporter-2 in proximal tubule → glucosuria + natriuresis + osmotic diuresis; also reduce cardiac fibrosis and oxidative stress | HFrEF (and HFpEF for dapagliflozin); reduces HF hospitalizations and CV death (DAPA-HF, EMPEROR-Reduced trials) | Dapagliflozin: 10 mg OD; Empagliflozin: 10 mg OD | Genital mycotic infections, UTI, euglycemic DKA (rare), volume depletion; avoid if eGFR <20 |
| Digoxin | Cardiac Glycoside | Inhibits Na+/K+-ATPase → increases intracellular Ca2+ → positive inotropy; also increases vagal tone → reduces HR | HFrEF with AF (rate control); symptomatic HF not responding to other drugs (NYHA III-IV); does NOT improve mortality | 0.125-0.25 mg OD (adjust for renal function and age) | Narrow therapeutic index! Nausea, vomiting, yellow-green vision (xanthopsia), AV block, ventricular arrhythmias; toxicity worsened by hypokalemia |
| Hydralazine + Isosorbide Dinitrate | Vasodilator combination | Hydralazine (arterial dilator) reduces afterload; nitrate (venous dilator) reduces preload | Alternative when ACE-i AND ARB/ARNI are both contraindicated; especially effective in African Americans (A-HeFT trial); NYHA III-IV | Hydralazine: 75 mg TDS + ISDN: 40 mg TDS | Headache, reflex tachycardia, drug-induced lupus (hydralazine), hypotension |
| Tolvaptan | Vasopressin V2 receptor antagonist (Aquaretic) | Blocks ADH → free water excretion without Na+ loss | Hyponatremia in HF; resistant fluid overload | 15-60 mg OD | Rapid sodium correction risk (osmotic demyelination), thirst, dry mouth, hepatotoxicity |
| IV Dobutamine | Beta-1 agonist (Inotrope) | Stimulates beta-1 receptors → ↑ CO and ↑ contractility | Acute decompensated HF with cardiogenic shock / low output state | 2-20 mcg/kg/min IV infusion | Tachycardia, arrhythmias, ischemia; only short-term bridge |
| IV Norepinephrine / Dopamine | Vasopressor / Inotrope | Alpha-1 + beta-1 agonism → vasoconstriction + inotrope | Cardiogenic shock with hypotension | NE: 0.1-1 mcg/kg/min | Arrhythmias, limb ischemia, tachycardia |
| Morphine (with caution) | Opioid | Venodilation + reduces anxiety + mild respiratory depression | Acute pulmonary edema (adjunct); controversial | 2-4 mg IV slow | Respiratory depression, hypotension; use with caution in acute HF |
Treatment Summary by Stage
| NYHA Class | Treatment |
|---|
| Class I (Asymptomatic, EF reduced) | ACE-i + Beta-blocker + treat risk factors |
| Class II | ACE-i (or ARNI) + Beta-blocker + MRA + SGLT2-i; add diuretic for fluid control |
| Class III | All of above + optimize doses; consider CRT/ICD if indicated |
| Class IV | IV diuretics, IV inotropes (dobutamine); palliative care / transplant |
Emergency drugs for Acute Pulmonary Edema:
- Sit patient upright + high-flow oxygen
- IV Furosemide 40-80 mg stat
- IV/sublingual Nitrates (reduces preload)
- IV Morphine 2-4 mg (with caution)
- Non-invasive ventilation (CPAP/BiPAP) if SpO2 <90%
- If hypotensive + shock → IV Dobutamine/Norepinephrine
11. CLINICAL PEARLS
- S3 gallop = "Ken-tuc-KY" rhythm = most specific auscultatory finding of systolic HF (volume overload). S4 = "TEN-nes-see" = diastolic dysfunction.
- BNP is synthesized in ventricular myocytes in response to wall stretch. It is a marker of wall stress, not just fluid.
- Never start a beta-blocker in acutely decompensated ("wet") HF - wait until the patient is "dry" (euvolemic). But never stop a beta-blocker in a CHF patient unless in cardiogenic shock.
- The CXR triad of HF: Cardiomegaly (CTR >0.5) + Kerley B lines (interstitial edema) + Cephalization of pulmonary vessels
- "Heart failure cells" = hemosiderin-laden alveolar macrophages = pathological sign of repeated pulmonary edema episodes
- Digoxin toxicity is worsened by hypokalemia (both compete at Na+/K+ATPase); always check potassium before giving digoxin
- SGLT2 inhibitors (dapagliflozin, empagliflozin) are now the 4th pillar of HFrEF treatment alongside ACE-i/ARNI + BB + MRA (2022 ESC Guidelines)
- ACE inhibitor causes DRY COUGH (bradykinin); ARBs do NOT (no bradykinin)
- Sacubitril/Valsartan MUST NOT be started within 36 hours of ACE inhibitor use (risk of angioedema)
- Spironolactone causes gynecomastia → switch to eplerenone
12. COMMON DIAGNOSTIC MISTAKES
| Mistake | Why It Happens | How to Avoid |
|---|
| Missing HF in COPD patient | Both cause dyspnea and crackles; COPD is common | Always check BNP and CXR in COPD patients with atypical/worsening dyspnea. Crackles in COPD are usually coarser and improve with coughing; HF crackles are fine and basal |
| Diagnosing HF when BNP is mildly elevated | BNP rises in PE, CKD, AF, sepsis, obesity (falsely low in obese!) | Use BNP in context; get echocardiogram to confirm |
| Attributing ankle edema to HF | Bilateral edema has many causes | Always look for raised JVP and lung crackles before attributing edema to HF |
| Starting Beta-blocker in decompensated HF | Confusing chronic stable HF management with acute management | Beta-blockers are contraindicated in wet/decompensated HF; only start when euvolemic |
| Missing HFpEF (normal EF) | Assuming normal echo rules out HF | HFpEF patients have normal EF; diagnosis requires diastolic dysfunction parameters on echo (E/e' ratio, tissue Doppler) |
| Digoxin toxicity missed | Toxicity symptoms are non-specific early on | Yellow vision, bradycardia, new arrhythmias = think digoxin toxicity. Always check digoxin level + K+ together |
| Stopping ACE-i due to mild creatinine rise | Mild rise (up to 30%) is acceptable and expected; only stop if rise >50% | Small rise in Cr = normal hemodynamic effect of ACE-i; indicates it's working on efferent arteriole |
| Missing AF as precipitant of HF | Atrial fibrillation with rapid rate may be the cause, not just the result | Always ask "what came first - AF or HF?" Check ECG immediately; rate control can dramatically improve EF |
13. 5-MINUTE REVISION SUMMARY
DEFINITION:
Heart unable to pump blood to meet body's demands → forward failure (low output)
+ backward failure (venous congestion)
↓
CAUSES:
IHD/MI (most common) → HTN → Valvular disease → Dilated CMP → Myocarditis → AF
↓
PATHOPHYSIOLOGY:
↓CO → ↑Sympathetic + ↑RAAS → ↑HR + ↑Preload + ↑Afterload + Remodeling
→ Vicious cycle → Cardiac hypertrophy → Fibrosis → Apoptosis → Worsening failure
↓
SYMPTOMS:
Left HF: DOE → Orthopnea → PND → Pink frothy sputum
Right HF: JVD, Pitting edema, Hepatomegaly, Ascites
Signs: S3 gallop, displaced apex, bilateral crackles, raised JVP
↓
INVESTIGATIONS:
BNP >400 (diagnostic) | Echo (gold standard - EF, wall motion)
CXR (cardiomegaly + Kerley B + bat-wing) | ECG (AF, LVH, Q waves)
K+, Na+, Creatinine, TFT | Troponin (if ACS suspected)
↓
TREATMENT (HFrEF - 4 pillars):
1. ACE-i or ARNI (Sacubitril/Valsartan) - anti-remodeling
2. Beta-blocker (Carvedilol/Bisoprolol) - anti-arrhythmic
3. MRA (Spironolactone) - anti-fibrotic
4. SGLT2-i (Dapagliflozin) - cardioprotective
+ Diuretics (Furosemide) for symptom relief
Acute: O2 + IV Furosemide + IV Nitrates + CPAP
↓
COMPLICATIONS:
Arrhythmias (AF, VF) → Sudden cardiac death
Cardiogenic shock | Pulmonary edema | Renal failure (Cardiorenal syndrome)
Liver failure (Cardiac cirrhosis) | Stroke (AF + LV thrombus)
Cachexia (cardiac cachexia - poor prognosis sign)
Recent Evidence Update (PubMed 2025): A meta-analysis published in Circulation (PMID: 40884036, Berg DD et al., Nov 2025 - DAPA ACT HF-TIMI 68 trial) confirmed that dapagliflozin initiated in-hospital for acute heart failure reduces the composite of worsening HF or CV death at 30 days. SGLT2 inhibitors are now supported for initiation even in the acute/hospitalized setting, not just stable outpatients.
Sources: Braunwald's Heart Disease (Cardiovascular Medicine Textbook) | Robbins & Cotran Pathologic Basis of Disease | Katzung's Basic & Clinical Pharmacology 16th Ed. | Goodman & Gilman's Pharmacological Basis of Therapeutics | Fuster & Hurst's The Heart 15th Ed.