Give me detail about vitamin D metabolism, take reference from Lippincott biochem and vasudewan biochem
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from both textbooks with excellent diagrams. Let me compose the full detailed answer.
Vitamin D Metabolism
Sources: Lippincott Illustrated Reviews: Biochemistry, 8th ed (p. 1085-1093) | Basic Medical Biochemistry: A Clinical Approach, 6th ed (Vasudevan, p. 1221-1222)
1. Nature and Overview
Vitamin D vitamins are a group of sterols with hormone-like function. The active molecule, 1,25-dihydroxycholecalciferol (1,25-diOH-D3, calcitriol), binds to intracellular receptor proteins. The 1,25-diOH-D3-receptor complex interacts with response elements in nuclear DNA of target cells - similar to how vitamin A acts - to selectively stimulate or repress gene transcription. Its most prominent actions are to regulate serum levels of calcium and phosphorus.
(Lippincott, p. 1085)
2. Sources of Vitamin D
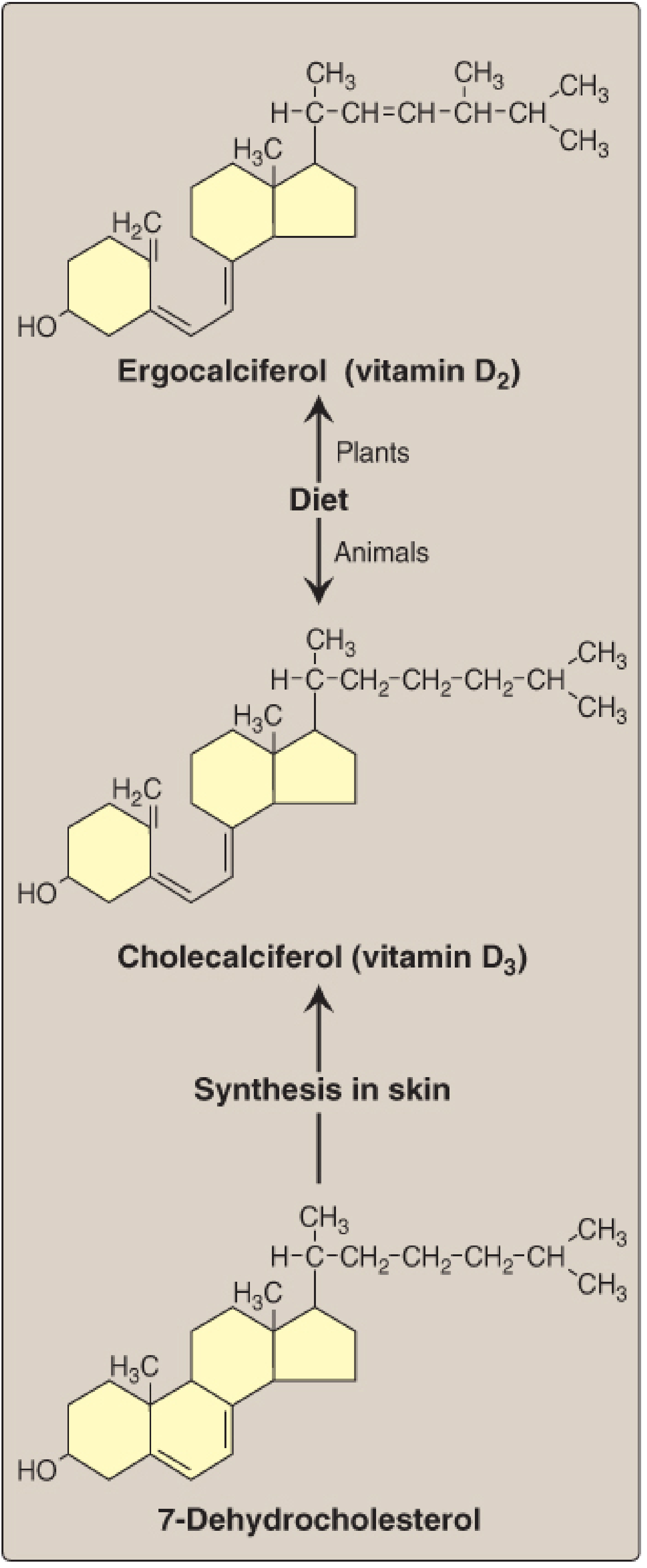
Fig. 28.22 - Sources of vitamin D (Lippincott, p. 1085)
There are two main sources:
A. Endogenous synthesis
- 7-Dehydrocholesterol (an intermediate in cholesterol synthesis) is present in the dermis and epidermis.
- UV light from sunlight cleaves the C9-C10 bond of the B-ring, converting 7-dehydrocholesterol into cholecalciferol (vitamin D3).
- Cholecalciferol is then transported to the liver bound to vitamin D-binding protein (DBP), also called transcalciferin.
- Note: 7-Dehydrocholesterol decreases in the skin of older adults, reducing endogenous synthesis.
(Lippincott p. 1086; Vasudevan p. 1221)
B. Dietary sources
- Ergocalciferol (vitamin D2) - found in plants (derived from ergosterol)
- Cholecalciferol (vitamin D3) - found in animal tissues (fatty fish, liver, egg yolk)
- D2 and D3 differ only in the presence of an extra double bond and methyl group in the plant sterol.
- Dietary vitamin D is packaged into chylomicrons for absorption.
- Preformed dietary vitamin D is only strictly required in individuals with limited sun exposure.
(Lippincott, p. 1086)
3. Metabolic Activation - Two Sequential Hydroxylations
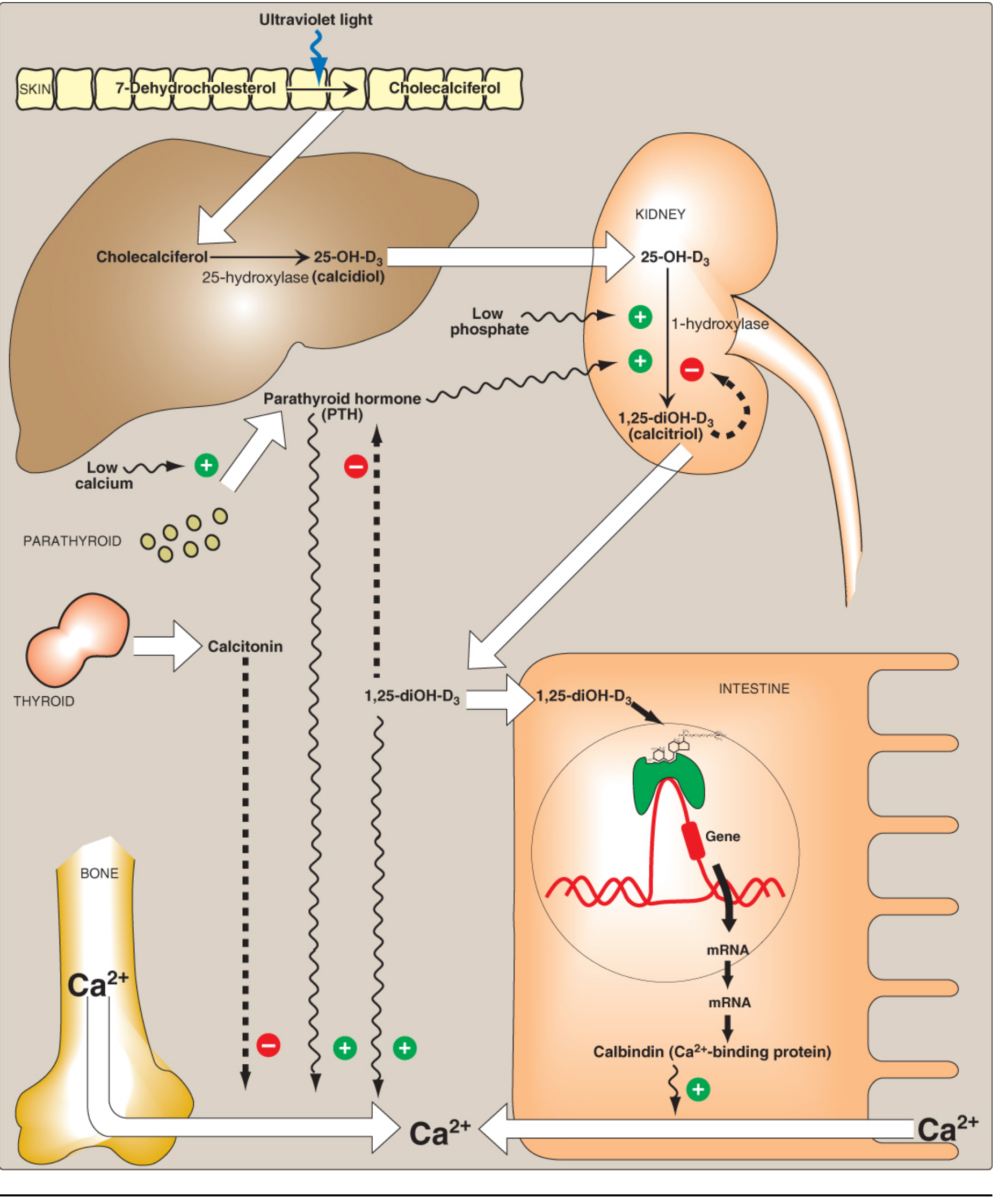
Fig. 28.23 - Metabolism and actions of vitamin D (Lippincott, p. 1088)
Vitamins D2 and D3 are not biologically active themselves. They undergo two sequential hydroxylations to produce calcitriol.
Step 1 - Hepatic 25-Hydroxylation (Liver)
- Enzyme: 25-hydroxylase (a cytochrome P450 protein, CYP25)
- Location: hepatic microsomes
- Product: 25-hydroxycholecalciferol (calcidiol, 25-OH-D3)
- Calcidiol is the predominant circulating form and major storage form of vitamin D in serum.
- It circulates bound to vitamin D-binding globulin (transcalciferin) to the kidney.
Step 2 - Renal 1-Hydroxylation (Kidney - Rate-Limiting Step)
- Enzyme: 25-hydroxycholecalciferol 1-hydroxylase (a mixed-function oxidase, CYP1α; also a cytochrome P450 protein)
- Location: proximal convoluted tubule of kidney
- Cofactors: molecular O2 and NADPH
- Product: 1,25-dihydroxycholecalciferol (calcitriol, 1,25-(OH)2D3) - the active form
- This is the rate-limiting, tightly regulated step.
(Lippincott p. 1087; Vasudevan p. 1222)
Vasudevan adds: 1,25-(OH)2D3 (calcitriol) is approximately 100 times more potent than 25-(OH)D3, yet 25-(OH)D3 is present in blood at concentrations ~100 times greater, suggesting calcidiol may also play some role in calcium/phosphorus homeostasis. (Vasudevan, p. 1222)
4. Regulation of Calcitriol Formation
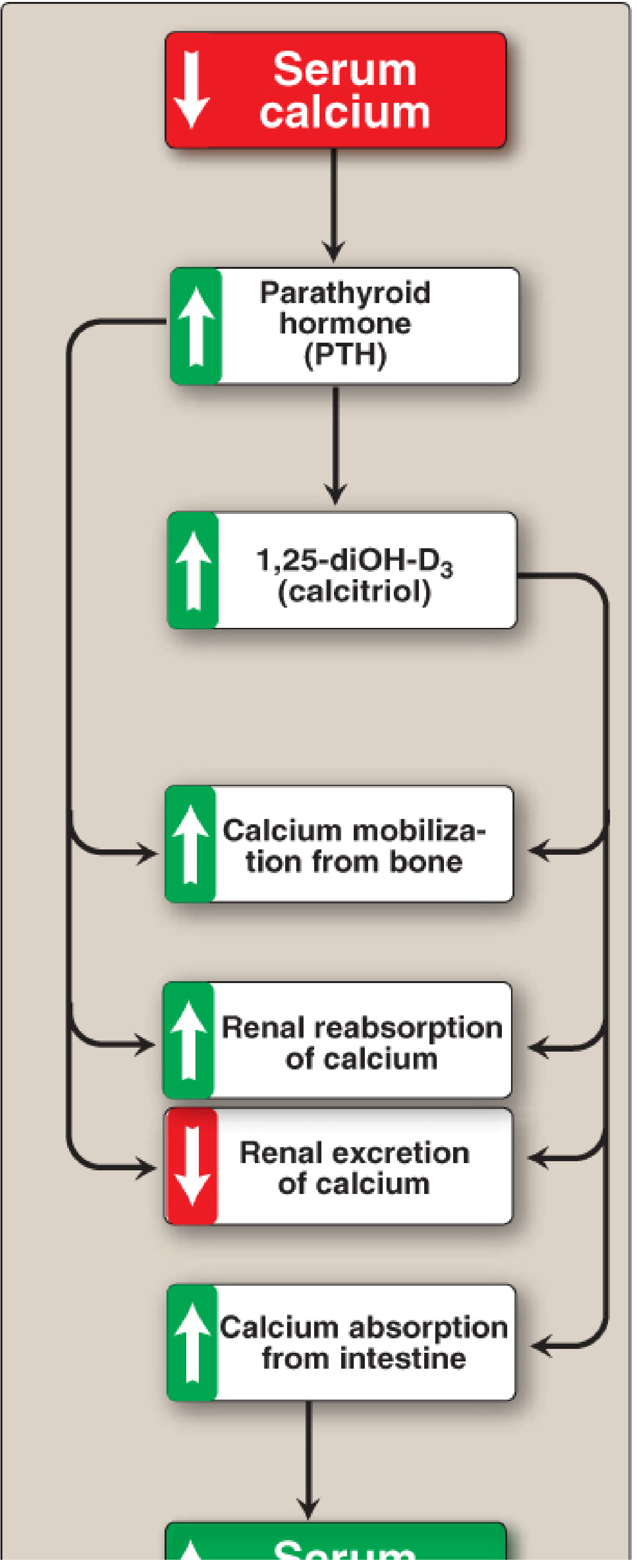
Fig. 28.24 - Response to low serum calcium (Lippincott, p. 1089)
The 1-hydroxylase activity (Step 2) is tightly regulated:
| Stimulus | Effect on 1-hydroxylase | Result |
|---|---|---|
| Low serum phosphate (PO4³⁻) | Direct stimulation (+) | More calcitriol formed |
| Low serum Ca²⁺ | Triggers PTH secretion → PTH upregulates 1-hydroxylase | More calcitriol formed |
| PTH (from parathyroid chief cells) | Activates 1-hydroxylase | More calcitriol |
| Calcitriol itself (1,25-diOH-D3) | Inhibits 1-hydroxylase (negative feedback) AND inhibits PTH expression | Less calcitriol formed |
- Low Ca²⁺ → PTH secretion → 1-hydroxylase activation → calcitriol production → raises serum Ca²⁺.
- Calcitriol then feeds back to inhibit PTH and the 1-hydroxylase, forming a classic negative-feedback loop.
- Calcitonin (thyroid hormone) opposes PTH: it decreases blood Ca²⁺ by inhibiting mobilization from bone, absorption from intestine, and reabsorption by kidney.
(Lippincott, p. 1087-1090)
5. Mechanism of Action (Molecular)
Calcitriol acts as a steroid hormone:
- Being lipid-soluble, it diffuses passively through the plasma membrane.
- It binds to specific cytosolic/nuclear Vitamin D Receptors (VDR) in the intestine, bone, and kidney.
- The calcitriol-VDR complex moves into the nucleus.
- It binds to Vitamin D Response Elements (VDREs) on DNA, activating or repressing gene transcription.
- In the intestinal mucosal cell, for example, genes encoding calcium-transporting proteins (notably calbindin, a Ca²⁺-binding protein) are activated, increasing Ca²⁺ absorption.
(Lippincott p. 1091; Vasudevan p. 1222)
6. Functions of Calcitriol
The overall function is to maintain adequate serum Ca²⁺ levels:
A. Intestine
- Stimulates intestinal Ca²⁺ absorption by inducing calbindin (calcium-binding protein).
- Also increases intestinal absorption of phosphate.
B. Kidney
- Increases renal reabsorption of Ca²⁺ (minimizes urinary loss).
- Increases renal reabsorption of phosphate (in contrast, PTH decreases phosphate reabsorption).
C. Bone
- Bone is composed of collagen + hydroxyapatite crystals [Ca5(PO4)3OH].
- When blood Ca²⁺ is low, calcitriol stimulates bone resorption (enhanced by PTH), releasing Ca²⁺ into the bloodstream.
- Bone serves as a key Ca²⁺ reservoir.
- PTH and calcitriol work together to prevent renal Ca²⁺ loss.
(Lippincott, p. 1091)
7. Dietary Requirement
- RDA: 15 μg/day (600 IU) for ages 1-70 years; 20 μg/day (800 IU) if over age 70 years.
- Conversion: 1 μg vitamin D = 40 IU.
- Dietary sources: fatty fish, liver, egg yolk; milk (unless fortified) is not a good source.
- Breast milk is a poor source - supplementation is recommended for breastfed babies.
- Deficiency is more common in northern latitudes due to reduced UV light exposure.
(Lippincott, p. 1091-1092)
8. Deficiency - Clinical Disorders
A. Nutritional Rickets (children)
- Vitamin D deficiency → net demineralization of bone.
- Continued collagen matrix formation but incomplete mineralization → soft, pliable bones.
- Skeletal deformities in children with low serum calcium and phosphorus.
- Low levels of serum Ca²⁺ and phosphate are hallmarks.
- Caused by insufficient sun exposure and/or dietary deficiency.
- Loss-of-function mutations in the VDR cause hereditary vitamin D-deficient rickets.
B. Osteomalacia (adults)
- Demineralization of pre-existing bones → increased susceptibility to fractures.
C. Renal Osteodystrophy
- Chronic kidney disease → decreased 1-hydroxylase activity → reduced calcitriol formation.
- Also: increased PO4³⁻ retention → hyperphosphatemia → hypocalcemia → elevated PTH → bone demineralization.
- Treatment: vitamin D supplementation + phosphate reduction therapy.
D. Hypoparathyroidism
- Lack of PTH → hypocalcemia + hyperphosphatemia (PTH normally increases phosphate excretion).
- Treatment: vitamin D + calcium supplementation.
(Lippincott, p. 1092-1093)
9. Toxicity
Vitamin D is fat-soluble and stored slowly metabolized in the body.
- High doses (100,000 IU for weeks/months) cause:
- Loss of appetite, nausea, thirst, weakness
- Enhanced Ca²⁺ absorption + bone resorption → hypercalcemia
- Hypercalcemia → deposition of calcium salts in soft tissue (metastatic calcification)
- The Tolerable Upper Limit (UL) is 100 μg/day (4,000 IU).
(Lippincott, p. 1093)
Summary Pathway
7-Dehydrocholesterol (skin)
↓ UV light (B-ring cleavage)
Cholecalciferol (D3) ←── Diet (D2/D3)
↓ Liver: 25-hydroxylase (CYP450)
↓ transported by DBP
25-OH-D3 (Calcidiol) ← Major serum/storage form
↓ Kidney: 1-hydroxylase (CYP1α) ← Rate-limiting
↓ Regulated by PTH↑, PO4↓, Ca²⁺↓
1,25-(OH)2-D3 (Calcitriol) ← ACTIVE FORM
↓
VDR binding → Gene transcription
→ ↑Calbindin (intestine) → ↑Ca²⁺ absorption
→ ↑Renal Ca²⁺ reabsorption
→ ↑Bone resorption (with PTH when Ca²⁺ low)
Key Distinction between the two books:
- Lippincott provides extensive mechanistic detail: the negative feedback loop (calcitriol inhibits both PTH and 1-hydroxylase), the role of calbindin, calcitonin's opposing effects, and detailed clinical applications.
- Vasudevan emphasizes that the 1-hydroxylation in the PCT is catalyzed by a mixed-function oxidase requiring O2 and NADPH, stresses the rate-limiting nature of this step, and highlights the potency comparison: calcitriol is 100× more potent than calcidiol, yet calcidiol circulates at 100× higher concentration.
Condition that cause increased vitamin D esp 25 OH In body
Finding Sources
Finding Sources
Searching PubMed
"25-hydroxyvitamin D" elevated causes conditions
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have rich, comprehensive content from multiple authoritative sources. Let me compile the complete answer.
Conditions Causing Elevated 25-OH Vitamin D (Calcidiol)
Important distinction: 25-OH-D3 (calcidiol) is the storage/circulating form whose level reflects total body vitamin D load. It is less tightly regulated than 1,25-(OH)2-D3 (calcitriol). An elevated 25-OH-D specifically signals excess substrate (too much input) or impaired downstream metabolism, while elevated 1,25-(OH)2-D signals increased activation (as in granulomatous disease).
Why 25-OH-D Rises More Easily Than Calcitriol
The production of 25-OH-D3 is less tightly regulated than the production of 1,25-(OH)2-D3. Hence, concentrations of 25-OH-D can be elevated severalfold when vitamin D intake is excessive - while 1,25-(OH)2-D (calcitriol) may actually remain within normal range due to its tight feedback regulation. In vitamin D intoxication, the hypercalcemia is due more to elevated 25-OH-D acting directly on intestine and bone (since 25-OH-D has definite, if low, biologic activity) than to elevated calcitriol.
(Harrison's Principles of Internal Medicine 22E, p. 1333)
CONDITIONS CAUSING ELEVATED 25-OH-D
1. Vitamin D Intoxication (Most Direct Cause)
Mechanism: Overwhelming hepatic 25-hydroxylation substrate → massive 25-OH-D accumulation.
- Chronic ingestion of >10,000 IU/day is usually required to produce significant hypercalcemia in otherwise healthy individuals.
- The stated safe upper limit is 2,000 IU/day (50 μg/day) in adults, though some elderly individuals in northern latitudes may require ≥2,000 IU/day.
- Goodman & Gilman's states: continued daily ingestion of ≥50,000 units or more may result in poisoning.
- Diagnostic threshold: 25-OH-D >100 ng/mL (>250 nmol/L) substantiates the diagnosis; many experts define intoxication at >375 nmol/L (150 ng/mL) (Scott-Brown's, p. 878).
Sources of excess vitamin D:
| Source | Details |
|---|---|
| Excessive supplementation | Iatrogenic overtreatment of hypoparathyroidism, osteoporosis |
| Fortified foods | Overly fortified dairy/food products |
| "Faddist" megadosing | Unsupervised high-dose supplement use |
| Excessive sun exposure | Prolonged UV exposure (though skin has protective mechanisms that limit excess) |
Why 25-OH-D accumulates: The hepatic 25-hydroxylase has no tight feedback regulation - it continues producing calcidiol proportionally to substrate. Additionally, 25-OH-D is fat-soluble and stored in adipose tissue, meaning intoxication can persist for weeks after stopping vitamin D intake.
Consequences of high 25-OH-D:
- 25-OH-D has direct (low-level) biologic activity at intestine and bone
- → Increased intestinal Ca²⁺ absorption
- → Increased Ca²⁺ release from bone resorption
- → Hypercalcemia and hypercalciuria
Treatment: Restrict dietary calcium + hydration + discontinue vitamin D. Glucocorticoids (40-100 mg/day prednisone) restore serum Ca²⁺ to normal by blocking excessive vitamin D action.
(Harrison's 22E, p. 1331-1335; Goodman & Gilman's, p. 208-210)
2. Excessive Sun Exposure
- UV light converts 7-dehydrocholesterol → cholecalciferol in skin → hepatic 25-hydroxylation → 25-OH-D rises.
- However, prolonged sun exposure has some built-in protection (excess pre-vitamin D3 is photodegraded to inert products), so sun exposure alone rarely causes clinical toxicity, but contributes to elevated 25-OH-D levels.
3. Primary Hyperparathyroidism (PHPT)
- PTH stimulates renal 1-hydroxylase → converts more 25-OH-D to 1,25-(OH)2-D.
- With long-standing PHPT, the substrate 25-OH-D can become progressively depleted as more is converted.
- Serum 1,25-(OH)2-D is typically elevated or in the upper half of the reference range (PTH drives its production).
- 25-OH-D itself is typically normal or low in PHPT (consumed as substrate), NOT elevated.
Note: PHPT elevates 1,25-(OH)2-D, not 25-OH-D. However, coexisting vitamin D supplementation in PHPT patients can raise 25-OH-D above baseline. (Tietz, p. 2137; Scott-Brown's, p. 878)
4. Impaired Conversion to Calcitriol (25-OH-D Accumulates)
When the 1-hydroxylation step is blocked or impaired, 25-OH-D piles up as the pathway is blocked downstream:
A. Chronic Kidney Disease (CKD)
- Loss of renal proximal tubular 1α-hydroxylase activity.
- 25-OH-D cannot be converted to active calcitriol.
- 25-OH-D levels may be elevated in early CKD if supplements are given without adequate conversion, or simply accumulate if input continues without conversion.
B. CYP24A1 (24-Hydroxylase) Loss-of-Function Mutations
- 24-hydroxylase is the enzyme that inactivates both 25-OH-D and 1,25-(OH)2-D.
- Biallelic (homozygous) loss-of-function mutations in CYP24A1 → impaired catabolism of 25-OH-D.
- 25-OH-D AND 1,25-(OH)2-D both accumulate → idiopathic infantile hypercalcemia (IIH).
- Also described in adults as a cause of nephrolithiasis and hypercalciuria.
(Harrison's 22E, p. 1072-1074)
C. Mutations in Renal Sodium-Dependent Phosphate Co-Transporters (SLC34A1/SLC34A3)
- Inactivating biallelic mutations → increased 1,25-(OH)2-D synthesis + accumulation.
- Upstream 25-OH-D may also rise.
(Harrison's 22E, p. 1074)
5. Granulomatous Diseases (Elevated 1,25-(OH)2-D, Secondarily Depletes 25-OH-D - BUT can elevate if D intake is high)
The granulomatous disease mechanism is primarily one of elevated 1,25-(OH)2-D, not 25-OH-D. However, it is clinically critical to understand:
Mechanism:
- Activated macrophages and epithelioid cells within granulomas express 1α-hydroxylase (CYP1α)
- This extrarenal 1α-hydroxylase converts 25-OH-D → 1,25-(OH)2-D without the normal feedback regulation (not suppressed by high Ca²⁺, high phosphate, or low PTH)
- Inflammatory mediators (TNF-α and others) increase both vitamin D receptor expression and 1α-hydroxylase activity in macrophages
Key feature (Harrison's): There is a positive correlation in sarcoidosis between 25-OH-D levels (reflecting vitamin D intake) and circulating 1,25-(OH)2-D. Normally, 1,25-(OH)2-D does not rise with increasing 25-OH-D due to tight renal feedback. In granulomatous disease, this control is lost.
Causes include:
| Disease | Notes |
|---|---|
| Sarcoidosis | Most common; hypercalciuria >hypercalcemia; 1,25-(OH)2-D elevated |
| Tuberculosis | Macrophage 1α-hydroxylase activation |
| Fungal infections (histoplasmosis, coccidioidomycosis, candidiasis) | Same mechanism |
| Berylliosis | Industrial exposure granulomatous disease |
| Leprosy | |
| Silicone-induced granulomas |
Lab pattern in granulomatous disease:
- PTH: low/suppressed
- 25-OH-D: normal or low (being consumed as substrate) - BUT if patient is simultaneously taking vitamin D supplements, 25-OH-D will be elevated and drives even more 1,25-(OH)2-D production
- 1,25-(OH)2-D: elevated (the primary abnormality)
- Phosphate: high-normal or elevated (vitamin D increases phosphate reabsorption)
(Harrison's 22E, p. 1337; Goldman-Cecil Medicine; Tietz Laboratory Medicine, p. 2137; Fitzpatrick's Dermatology)
6. Lymphoma
- Certain lymphomas (especially HTLV-1 associated lymphoma, Hodgkin lymphoma, non-Hodgkin lymphoma) produce ectopic 1α-hydroxylase in tumor tissue.
- Mechanism is similar to granulomatous disease - unregulated conversion of 25-OH-D → 1,25-(OH)2-D.
- Results in elevated 1,25-(OH)2-D and hypercalcemia; 25-OH-D may be consumed.
- 5-15% of malignancy-associated hypercalcemia cases. (Tietz, p. 2137)
7. Williams' Syndrome (Hypercalcemia of Infancy)
- Autosomal dominant condition with abnormal sensitivity to vitamin D.
- Impaired catabolism of 25-OH-D and calcitriol, leading to accumulation.
- Associated with supravalvular aortic stenosis, elfin facies, intellectual disability.
- Presentation in infancy with hypercalcemia. (Harrison's 22E)
Summary Comparison Table
| Condition | 25-OH-D | 1,25-(OH)2-D | PTH | Ca²⁺ | Mechanism |
|---|---|---|---|---|---|
| Vitamin D intoxication | ↑↑↑ | Normal/↑ | ↓ suppressed | ↑ | Excess substrate accumulation |
| Excess sun/diet | ↑ | Normal | Normal-↓ | Normal-↑ | Excess substrate |
| CYP24A1 mutation | ↑ | ↑ | ↓ | ↑ | Impaired catabolism |
| Granulomatous disease (sarcoid, TB) | Normal/↓ | ↑↑ | ↓ | ↑ | Extrarenal 1α-hydroxylase |
| Lymphoma | Normal/↓ | ↑ | ↓ | ↑ | Ectopic 1α-hydroxylase |
| PHPT | Normal/↓ | ↑ | ↑↑ | ↑ | PTH drives 1-hydroxylase |
| CKD | Normal/↑ (if supplemented) | ↓ | ↑ | ↓ | Loss of 1α-hydroxylase |
| Williams' syndrome | ↑ | ↑ | ↓ | ↑ | Impaired catabolism |
Key Clinical Point
An elevated 25-OH-D >100 ng/mL specifically points to excess vitamin D intake (the most common cause). An elevated 1,25-(OH)2-D with normal/low 25-OH-D points to granulomatous disease or lymphoma with ectopic 1α-hydroxylase. Measuring both metabolites together is essential to differentiate the cause of vitamin D-related hypercalcemia.
(Scott-Brown's Otorhinolaryngology, p. 878; Harrison's 22E, p. 1335)
Detail UTI guidelines of KDIGO and IDSA
Finding Sources
Searching the Web
IDSA UTI guidelines 2024 2025 uncomplicated complicated catheter-associated
Searching PubMed
"urinary tract infection" AND "guidelines" AND ("IDSA" OR "KDIGO")
Searching the Web
KDIGO UTI guidelines kidney transplant urinary tract infection 2024 2025
Finding Sources
Searching PubMed
"urinary tract infection" AND "treatment" AND "guideline"
Reading Web Page
https://www.the-hospitalist.org/hospitalist/article/40900/cr…
Reading File
Reading File
Finding Sources
Searching the Web
KDIGO UTI kidney transplant guidelines recommendations prophylaxis 2023 2024
Reading File
Reading Web Page
https://kdigo.org/wp-content/uploads/2017/02/KITxpGL_summary…
Reading File
Reading File
UTI Guidelines: IDSA (2025) and KDIGO (Kidney Transplant)
Sources: IDSA Complicated UTI Guidelines 2025 | KDIGO Clinical Practice Guideline for the Care of Kidney Transplant Recipients | Harrison's Principles of Internal Medicine 22E (2025) | Brenner & Rector's The Kidney
PART 1 - IDSA UTI GUIDELINES (2025 Update)
The 2025 IDSA guidelines are the first major update since 2010 and the first-ever IDSA guidelines specifically for complicated UTI (cUTI). The prior guidelines addressed only uncomplicated cystitis and pyelonephritis in women. This update is co-sponsored by the Society of Hospital Medicine.
1. New Definitions (2025 Revision)
The 2025 guidelines fundamentally revised the classification of UTI to align with clinical reality rather than patient demographics.
| Term | 2025 IDSA Definition |
|---|---|
| UTI | Symptomatic disease only - bacteria in urine WITHOUT symptoms = ASB, NOT UTI |
| Uncomplicated UTI | Infection confined to the bladder in a woman or man, WITHOUT a urinary catheter |
| Complicated UTI (cUTI) | Infection that has extended beyond the bladder - i.e., to the kidneys, prostate, or bloodstream |
| CAUTI | UTI in the setting of intermittent or indwelling urinary catheterization |
| Recurrent UTI | Not automatically complicated; individual episodes can be uncomplicated |
| ASB | Bacteria in urine without symptoms - usually does NOT require treatment |
Critical departure from old classification:
- Conditions like diabetes, immunocompromise, BPH, cystocele, male sex - these NO LONGER automatically make a UTI complicated.
- These factors may still influence treatment decisions but do not define the classification.
- Both men and women can now have uncomplicated UTIs.
- The definition focuses on systemic symptoms (fever, flank pain, chills, rigors, CVA tenderness), upper tract obstruction (stone), renal parenchymal involvement, or indwelling hardware (catheter, nephrostomy tube, ureteral stent).
"The key considerations for the frontline clinician include whether the patient is stable for outpatient management, whether a source of recalcitrant infection needs to be identified, and whether the antimicrobial must achieve adequate levels in blood and renal tissue." - Harrison's 22E
2. What Is EXCLUDED from These Guidelines
- Bacterial prostatitis (acute and chronic) - requires separate approach; prolonged therapy with prostate-penetrating antibiotics may be needed
- Epididymitis and orchitis
- Urethritis (predominantly STI-related: N. gonorrhoeae, C. trachomatis, M. genitalium)
- Pediatric UTI
3. Asymptomatic Bacteriuria (ASB) - When NOT to Treat
General rule: Do NOT treat ASB. Evidence shows:
- Treatment of ASB does not decrease frequency of subsequent true UTIs.
- In renal transplant recipients, ASB treatment may even increase future infection risk.
- Treating ASB promotes colonization with more virulent and antibiotic-resistant pathogens.
Exceptions - TREAT ASB in:
- Pregnant patients - untreated ASB linked to pyelonephritis, preterm delivery, and low birth weight. Screen and treat routinely.
- Patients undergoing high-risk urologic procedures that cause mucosal injury (e.g., lithotripsy, transurethral resection of the prostate [TURP]) - risk of bacterial translocation to blood.
4. Antibiotic Principles - Collateral Damage Concept
IDSA emphasizes collateral damage = adverse ecologic effects of antibiotics including:
- Killing of normal flora → risk of Clostridioides difficile infection
- Selection of drug-resistant organisms
Drugs with MINIMAL effect on fecal flora (preferred):
- Nitrofurantoin
- Fosfomycin
- Pivmecillinam
Drugs with SIGNIFICANT collateral damage (use cautiously):
- TMP-SMX
- Fluoroquinolones
- Late-generation cephalosporins
5. Uncomplicated Cystitis - IDSA Recommendations
| Antibiotic | Dose | Duration | Notes |
|---|---|---|---|
| Nitrofurantoin macrocrystals | 100 mg BD | 5 days | First-line; minimal collateral damage; avoid if eGFR <30 |
| TMP-SMX | 160/800 mg BD | 3 days | First-line if local resistance <20%; check local antibiogram |
| Fosfomycin trometamol | 3 g single dose | 1 day | First-line; single dose convenience; less data vs cystitis |
| Pivmecillinam | 400 mg BD | 3-7 days | Where available; minimal collateral damage |
| Fluoroquinolones (ciprofloxacin, levofloxacin) | Standard doses | 3 days | NOT first-line; reserve due to resistance, collateral damage, and adverse effects |
| Beta-lactams (amoxicillin-clavulanate, cefdinir) | Standard doses | 3-7 days | Inferior to nitrofurantoin/TMP-SMX; use if others unsuitable |
Note: Fluoroquinolones should NOT be used as first-line for uncomplicated cystitis per IDSA - they are effective but cause too much collateral damage and their use should be reserved for more serious infections.
6. Acute Uncomplicated Pyelonephritis - IDSA
Outpatient management (majority of cases):
| Antibiotic | Dose | Duration |
|---|---|---|
| Ciprofloxacin | 500 mg BD | 7 days |
| Levofloxacin | 750 mg OD | 5 days |
| TMP-SMX | 160/800 mg BD | 14 days (if susceptible) |
| Oral beta-lactams | Standard doses | 10-14 days |
- Urine culture should be obtained before treatment.
- If fluoroquinolone resistance >10% locally, give an initial single dose of IV ceftriaxone or aminoglycoside, then switch to oral therapy.
- Obtain blood cultures if systemic toxicity or hospitalization required.
Inpatient management (severe/unable to tolerate oral):
- IV ciprofloxacin, ceftriaxone, aminoglycoside, or piperacillin-tazobactam
- Transition to oral once improving and afebrile for 24-48 hours
7. Complicated UTI (cUTI) - The New 4-Step Empiric Antibiotic Framework
Step 1 - Assess severity (sepsis vs. no sepsis)
- If sepsis present: requires broad-spectrum IV antibiotics
- If no sepsis: can consider oral therapy depending on clinical stability
Step 2 - Review recent urine cultures (within 3-6 months)
- Prior culture results significantly improve empiric selection
- If prior resistant organism - avoid that antibiotic class empirically
Step 3 - Account for patient-specific resistance risk factors
- Prior antibiotic exposures (especially fluoroquinolones, highest risk)
- Recent hospitalization or urinary catheterization
- Travel to high-resistance areas
- History of ESBL or other resistant organisms
Step 4 - Incorporate local antibiogram (for sepsis patients)
- For cUTI with sepsis: use local antibiogram to tailor empiric choice (conditional recommendation, very low certainty)
- For cUTI without sepsis: no specific antibiogram recommendation (knowledge gap)
8. Empiric Antibiotic Selection for cUTI
cUTI WITHOUT Sepsis (preferred options):
- Third- or fourth-generation cephalosporins (ceftriaxone, cefepime)
- Piperacillin-tazobactam
- Fluoroquinolones (if local susceptibility favorable)
Agents generally NOT appropriate for cUTI because they may not achieve adequate renal parenchymal/bloodstream levels:
- Nitrofurantoin
- Oral fosfomycin
- Amoxicillin-clavulanate / 1st-2nd generation cephalosporins / TMP-SMX (less studied; may be appropriate in select settings)
cUTI WITH Suspected or Confirmed ESBL/MDR Organisms:
- Carbapenems (ertapenem, meropenem, imipenem) - for ESBL-producing organisms
- Novel beta-lactam/beta-lactamase inhibitors (ceftazidime-avibactam, ceftolozane-tazobactam, meropenem-vaborbactam) - for carbapenem-resistant organisms (CRO/CRKP)
- Cefiderocol - for difficult MDR organisms
- Plazomicin - aminoglycoside option for MDR
- Newer agents reserved for confirmed resistant organisms; not for routine empiric use
9. IV-to-Oral (IV-to-PO) Transition
IDSA 2025 Recommendation (conditional, very low certainty):
In patients with cUTI (including acute pyelonephritis) with gram-negative bacteremia who are:
- Clinically improving
- Able to tolerate oral medication
- Have an effective oral option available
→ Transition to oral antibiotics rather than continuing parenteral therapy for the remaining treatment duration.
This supports early oral switch - patients do not need to complete a full IV course.
10. Duration of Therapy for cUTI
| Scenario | Recommended Duration | Agent |
|---|---|---|
| cUTI clinically improving | 5-7 days | Fluoroquinolone |
| cUTI clinically improving | 7 days | Non-fluoroquinolone |
| cUTI with gram-negative bacteremia, improving | 7 days total | Any effective antibiotic |
| Suspected acute bacterial prostatitis in men | 10-14 days | Prostate-penetrating antibiotic |
| cUTI with oral beta-lactams | 10-14 days (individualized) | Most studies used this duration |
Important caveat: Studies supporting shorter durations EXCLUDED patients with:
- Indwelling urinary catheters
- Severe sepsis
- Significant immunocompromise
- Urinary tract abscesses
- CKD
- Complete urinary obstruction
- Recent urologic procedures → These patients may still require 10-14 days.
11. Definitive Therapy - De-escalation
Once culture results are available:
- Select a targeted-spectrum antibiotic based on susceptibility results.
- De-escalate from broad-spectrum empiric therapy whenever possible.
- Continue broad-spectrum antibiotics for the full duration only if clinically necessary.
12. Recurrent UTI in Women - Prevention Strategies
Non-antimicrobial approaches (preferred when possible):
- Increased fluid intake - reduces recurrence (well-tolerated)
- Methenamine hippurate (converted to formaldehyde antiseptic in bladder) - may reduce recurrences as much as antibiotic prophylaxis
- Cranberry products - Cochrane review found significant benefit in women and children
- Intravaginal Lactobacillus - one factorial trial showed benefit (NOT oral probiotics)
- D-Mannose - mixed results
- Caution with probiotics in immunocompromised patients (invasive probiotic infections reported)
Antibiotic prophylactic strategies:
| Strategy | Regimen | Duration |
|---|---|---|
| Continuous prophylaxis | Low-dose TMP-SMX or nitrofurantoin daily or 3x/week | 6 months, can be extended |
| Postcoital prophylaxis | Single dose TMP-SMX or nitrofurantoin after intercourse | As needed |
| Patient-initiated therapy | Self-treatment at first symptoms with short course | Per episode |
Threshold: ≥3 symptomatic episodes/year is the typical threshold to initiate prophylaxis, but shared decision-making is recommended.
PART 2 - KDIGO GUIDELINES ON UTI
KDIGO addresses UTI in two specific contexts:
- Kidney Transplant Recipients (KTRs) - KDIGO Clinical Practice Guideline for the Care of Kidney Transplant Recipients (Chapter 14)
- ADPKD patients - KDIGO 2025 ADPKD Guidelines (Section 2.6)
KDIGO UTI Recommendations for Kidney Transplant Recipients
Grading System
- Grade 1 = We RECOMMEND (strong)
- Grade 2 = We SUGGEST (weak)
- A = High quality evidence | B = Moderate | C = Low | D = Very low
Recommendation 14.1.1 - UTI Prophylaxis
"We suggest that all KTRs receive UTI prophylaxis with daily trimethoprim-sulfamethoxazole for at least 6 months after transplantation." (Grade 2B)
- TMP-SMX serves a dual purpose: prophylaxis against both UTIs AND Pneumocystis jirovecii pneumonia (PCP)
- Duration: minimum 6 months post-transplant
- Short-term antibiotic prophylaxis (e.g., ciprofloxacin) at the time of urinary catheter removal can significantly reduce early post-transplant UTI risk
- If TMP-SMX intolerant: alternatives include fluoroquinolone or dapsone (for PCP) + targeted UTI prophylaxis
Recommendation 14.1.2 - Allograft Pyelonephritis
"We suggest initial hospitalization and treatment with intravenous antibiotics for allograft pyelonephritis." (Grade 2C)
Why hospitalization?
- Immunosuppressed state = higher risk of sepsis and rapid deterioration
- Graft at risk (pyelonephritis can precipitate acute rejection and graft dysfunction)
- IV antibiotics required until clinical improvement demonstrated
Empiric IV regimens for allograft pyelonephritis:
- Amoxicillin + aminoglycoside
- Second-generation cephalosporin + aminoglycoside
- Third-generation cephalosporin IV (e.g., ceftriaxone)
- Adjust based on local resistance patterns and prior culture data
KDIGO ADPKD 2025 - UTI Recommendations (Section 2.6)
Recommendation 2.6.1 (1B - STRONG):
"Clinicians should NOT treat asymptomatic bacteriuria (ASB) in patients with ADPKD."
Recommendation 2.6.2 (1B - STRONG):
"Clinicians should use first-line therapy (nitrofurantoin, TMP-SMX, fosfomycin) dependent on the local antibiogram for treatment of symptomatic UTIs in women."
Recommendation 2.6.3 (2B - WEAK):
"Clinicians should treat recurrent UTI patients experiencing acute cystitis episodes with as short a duration of antibiotics as reasonable, generally no longer than 7 days."
Practice Point 2.6.1:
Recurrent UTIs in ADPKD should be investigated for possible underlying predisposition (structural abnormalities, cyst infections)
Practice Point 2.6.2:
A urine culture should be obtained before antibiotics are started for UTI, especially for upper UTI and/or suspected kidney cyst infection. Blood cultures should be obtained if upper UTI or kidney cyst infection is suspected.
Special Considerations in ADPKD - Cyst Infection
This is a unique complication requiring specific management:
| Feature | Cyst Infection | Uncomplicated UTI |
|---|---|---|
| Presentation | Flank/abdominal pain, fever, nausea | Dysuria, frequency, urgency |
| Risk of sepsis | High - treat aggressively | Lower |
| Culture | Urine + blood cultures | Urine culture (if upper UTI) |
| Antibiotic penetration | Must penetrate cyst wall - fluoroquinolones preferred | Standard antibiotics |
| Duration | Longer than pyelonephritis | Shorter courses |
| Drainage | May be necessary for refractory cases | Not needed |
| Role of imaging | Abdominal imaging to rule out cyst infections | Not routine |
| Inpatient? | Yes - hospitalize | Outpatient usually |
Why fluoroquinolones for cyst infections? They have excellent lipid solubility and penetrate cyst walls, unlike beta-lactams which have poor cyst penetration.
Nephrectomy (last resort): May be indicated for emphysematous cysts, patients with recurrent/refractory infections planning kidney transplantation, or staghorn calculi causing recurrent UTIs in a nonfunctioning kidney.
Comparison: IDSA vs. KDIGO on Key Points
| Parameter | IDSA 2025 | KDIGO (Transplant) | KDIGO (ADPKD) |
|---|---|---|---|
| Scope | General population cUTI | Kidney transplant recipients | ADPKD patients |
| ASB treatment | Only in pregnancy + pre-procedure | Do NOT treat (may increase future UTI) | Do NOT treat (1B) |
| Uncomplicated UTI | Bladder-confined, any gender | N/A | First-line: nitrofurantoin/TMP-SMX/fosfomycin |
| cUTI definition | Beyond bladder or catheter-associated | Allograft pyelonephritis = hospitalize | Cyst infection = prolonged therapy |
| Empiric antibiotics (cUTI) | 3rd/4th gen cephalosporin, pip-tazo, FQ | Amox+aminoglycoside, 3rd gen ceph | Local antibiogram |
| Prophylaxis | TMP-SMX or nitrofurantoin (recurrent) | TMP-SMX x 6 months post-transplant (2B) | Short duration, ≤7 days |
| Duration (cUTI) | 5-7 days FQ; 7 days non-FQ | IV until improvement, then step-down | As short as reasonable |
| IV-to-oral switch | Early switch if improving | Transition once clinical improvement | N/A |
| De-escalation | Strongly emphasized | Culture-guided | Culture before starting |
Key Antibiograms and Resistance Thresholds (IDSA)
| Antibiotic | Resistance Threshold to AVOID empiric use |
|---|---|
| TMP-SMX | >20% local resistance → avoid for uncomplicated cystitis |
| Fluoroquinolones | >10% local resistance → add initial IV dose for uncomplicated pyelonephritis |
| Any antibiotic | If prior resistant culture in past 3-6 months → avoid |
Summary of Stewardship Principles (Both Guidelines)
- Treat symptoms, not cultures - never treat ASB (except pregnancy/pre-procedure)
- Culture before treating in complicated, upper, or recurrent UTIs
- De-escalate to targeted narrow-spectrum once sensitivities known
- Shortest effective duration - 5-7 days is adequate for most cUTI
- Early oral switch - IV is not superior to oral in clinically improving patients
- Avoid fluoroquinolones as first-line for uncomplicated cystitis - reserve for more serious infections
- Local antibiogram - always consult when sepsis is present
- In transplant patients - TMP-SMX prophylaxis x 6 months covers both UTI and PCP
This is a shared conversation. Sign in to Orris to start your own chat.