He
Hey! How can I help you today?
Noramal ecg
Reading File
Finding Sources
Searching Images
normal ECG electrocardiogram waves intervals
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a comprehensive overview of the Normal ECG (Electrocardiogram):
Normal ECG — Overview
The ECG measures tiny potential differences on the body surface that reflect the electrical activity of the heart. Electrodes detect the sequence and timing of depolarization and repolarization across the myocardium.
ECG Diagram — Waves, Segments & Intervals


Waves and What They Represent
| Wave / Feature | Electrical Event | Normal Value |
|---|---|---|
| P wave | Atrial depolarization (SA node → atria) | Duration < 120 ms; upright in leads I, II, aVF |
| PR interval | Atrial depol. → start of ventricular depol. (includes AV node delay) | 120–200 ms (normal ~160 ms) |
| QRS complex | Ventricular depolarization | < 120 ms (≈ 80–100 ms) |
| ST segment | Between end of ventricular depol. and start of repolarization | Isoelectric (flat); no elevation or depression |
| T wave | Ventricular repolarization | Upright in most leads; concordant with QRS |
| QT interval | Ventricular depol. + repolarization (QRS onset → T wave end) | QTc: 350–440 ms (men), up to 460 ms (women) |
| J point | Junction of QRS end and ST segment start | At baseline (isoelectric) |
| U wave | Possibly Purkinje fiber repolarization (not always visible) | Small, positive deflection after T wave |
Key distinction: Intervals include waves; segments do not.
Normal Sinus Rhythm Criteria
- Rate: 60–100 beats/min (measured by R-R interval: HR = 1/cycle length)
- Rhythm: Regular — consistent R-R intervals
- P wave before every QRS — upright in leads I, II; negative in aVR
- 1:1 P:QRS relationship
- PR interval: 120–200 ms
- QRS duration: < 120 ms (narrow)
- ST segment: Isoelectric — no elevation or depression
- T waves: Upright and concordant with QRS in lateral leads
ECG Paper & Calibration
| Measurement | Value |
|---|---|
| Paper speed | 25 mm/sec |
| Small box (1 mm) | 0.04 sec (40 ms) horizontally; 0.1 mV vertically |
| Large box (5 mm) | 0.2 sec (200 ms) horizontally; 0.5 mV vertically |
| Standard gain | 10 mm = 1 mV |
12-Lead ECG — A Normal Example
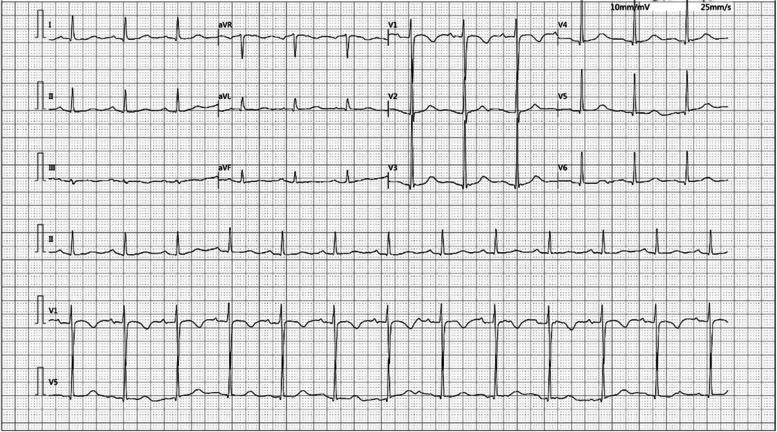
This 12-lead tracing shows:
- Regular P waves preceding every QRS in all leads
- Narrow QRS complexes with normal morphology
- No ST elevation or depression
- Upright T waves in V2–V6
- No pathological Q waves
Why the QRS Isn't Wider Than the P Wave
Though the ventricles are much larger than the atria, the His-Purkinje system conducts at very high velocity, allowing the entire ventricular myocardium to depolarize almost as quickly as the atria. This keeps QRS duration similar to P wave duration.
Sources: Costanzo Physiology 7th Ed., p. 149 | Goldman-Cecil Medicine, p. 421
Heart attack ecg
Finding Sources
Searching Images
myocardial infarction heart attack ECG ST elevation STEMI changes
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Finding Sources
Searching Images
ECG evolution myocardial infarction sequence hyperacute T wave ST elevation Q wave changes over time
Loading Image
Loading Image
Here is a comprehensive guide to the Heart Attack (Myocardial Infarction) ECG:
Heart Attack ECG — Overview
A myocardial infarction (MI) occurs when a coronary artery is occluded, cutting off blood supply to heart muscle. The ECG is the first-line diagnostic tool — in STEMI, it is diagnostic on its own. ECG changes evolve over time in a predictable sequence.
The 4 Classic ECG Changes of MI (in order of appearance)
| Stage | ECG Finding | Timing | Meaning |
|---|---|---|---|
| 1. Hyperacute | Tall, broad-based, symmetric T waves | Minutes | Very early ischemia (often missed) |
| 2. Acute | ST-segment elevation (convex/tombstone) | Minutes–hours | Active transmural injury — call for reperfusion NOW |
| 3. Evolving | Q wave formation + T wave inversion | Hours–days | Myocardial necrosis developing |
| 4. Old/Chronic | Persistent pathological Q waves | Days–weeks onward | Permanent scar |
Stage 1 — Hyperacute T Waves (Earliest Sign)
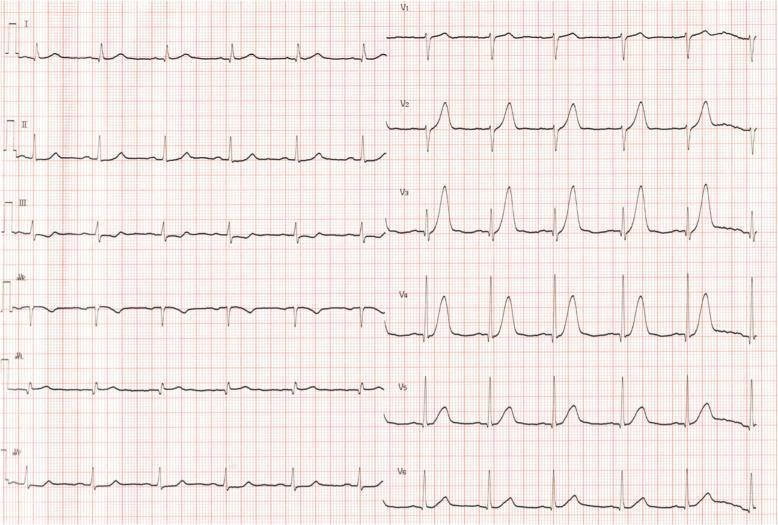
- Disproportionately tall, broad, symmetric T waves in precordial leads (V2–V4 here)
- Mild ST elevation beginning
- Seen within minutes of coronary occlusion — often missed clinically
Stage 2 — Acute STEMI (Anterolateral)

This is a classic anterolateral STEMI (LAD occlusion):
- Convex ("tombstone") ST elevation in V1–V6, I, aVL
- Reciprocal ST depression in inferior leads (II, III, aVF) — this confirms true elevation
- Peaked hyperacute T waves in V2–V4
Stage 2 — Acute Inferior STEMI
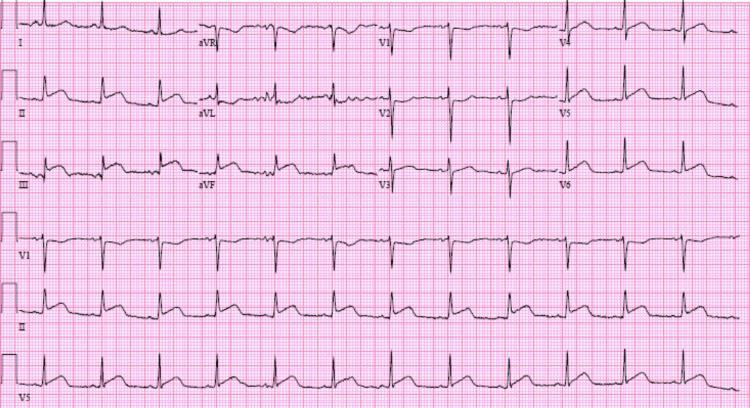
Classic inferior STEMI (RCA or circumflex occlusion):
- ST elevation in II, III, aVF
- Reciprocal ST depression + T wave inversion in I, aVL
- Usually due to right coronary artery (RCA) occlusion
Stages 2→4 Evolution — Inferior MI Before & After
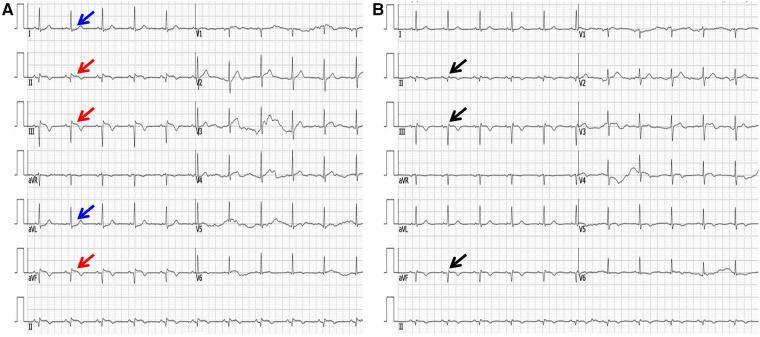
- Panel A (Acute): Red arrows = ST elevation in II, III, aVF; Blue arrows = reciprocal depression in I, aVL
- Panel B (1 week later): ST normalized; Black arrows = pathological Q waves now permanent in inferior leads → confirms old infarction
STEMI Diagnostic Criteria (Fourth Universal Definition)
| Lead Group | Cut-off for STEMI |
|---|---|
| Most leads (≥2 contiguous) | ST elevation ≥ 1 mm |
| V2–V3, females | ≥ 1.5 mm |
| V2–V3, males ≥ 40 yrs | ≥ 2 mm |
| V2–V3, males < 40 yrs | ≥ 2.5 mm |
MI Localization by Lead
| MI Territory | Leads with Changes | Artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Anterolateral | V1–V6, I, aVL | Proximal LAD |
| Lateral | I, aVL, V5–V6 | LCx or diagonal |
| Inferior | II, III, aVF | RCA (or LCx) |
| Posterior | Reciprocal depression V1–V3 (mirror image) | RCA or LCx |
| Septal | V1–V2 | Septal LAD branches |
Pathological Q Wave Criteria
A Q wave is pathological (indicating necrosis) when:
- Width ≥ 0.04 sec (1 small box)
- Depth ≥ 25% of the R wave amplitude
- Present in ≥ 2 contiguous leads
Q waves usually appear 8–12 hours after infarction onset, but can appear within the first hour. They may persist permanently as markers of old MI.
NSTEMI vs STEMI
| Feature | STEMI | NSTEMI |
|---|---|---|
| ECG | ST elevation | ST depression / T inversion / normal |
| Artery | Complete occlusion | Partial occlusion |
| Q waves | Usually develop | Usually absent |
| Treatment | Emergency PCI / fibrinolysis | Anticoagulation, urgent PCI |
| Biomarkers | Elevated (troponin, CK-MB) | Elevated |
Sources: Rosen's Emergency Medicine | Harrison's Principles of Internal Medicine 22E | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.