Refeeding syndrome
Reading File
Finding Sources
Searching PubMed
"refeeding syndrome"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Refeeding Syndrome
Refeeding syndrome is a potentially life-threatening metabolic complication that occurs when nutrition is reintroduced - enterally, parenterally, or even orally - after a period of prolonged starvation or severe malnutrition. It was first described after World War II, when starved Japanese prisoners were refed and experienced sudden electrolyte crises and deaths.
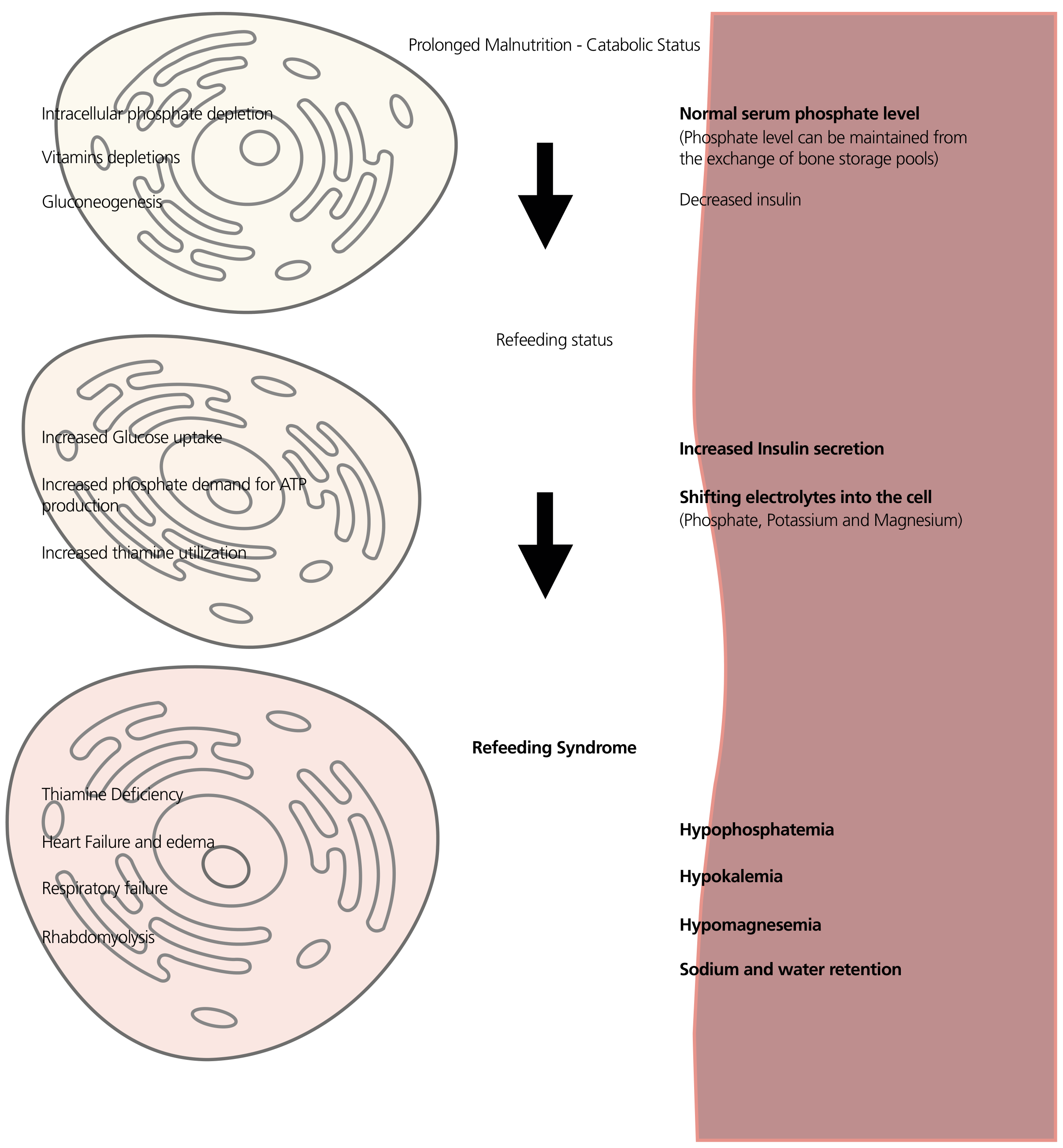
Pathophysiology
The central event is a shift from fat-based to carbohydrate-based metabolism, driven by reintroduction of glucose.
During starvation:
- Fatty acids and amino acids become the primary fuel
- Insulin levels fall; gluconeogenesis predominates
- Intracellular electrolytes (phosphate, potassium, magnesium) are progressively depleted
- Serum levels may remain deceptively normal because phosphate is mobilised from bone stores
When refeeding begins:
- Carbohydrate load stimulates a surge in insulin secretion
- Insulin activates Na-K ATPase, driving potassium (and phosphate, magnesium) into cells
- Phosphate is consumed rapidly in glycolysis and ATP synthesis
- The result: rapid, severe drops in serum phosphate, potassium, and magnesium
- Thiamine demand spikes (it is a cofactor for pyruvate dehydrogenase); without thiamine, pyruvate cannot enter the Krebs cycle, causing lactic acidosis
- Sodium and water retention occur alongside the electrolyte shifts
The hallmark biochemical abnormality is hypophosphataemia - Bailey and Love's, Sabiston, Yamada's, and Schwartz's all identify this as the primary driver. Incidence of refeeding-related hypophosphataemia in hospitalised patients on parenteral nutrition can be as high as 1 in 3 - Brenner & Rector's The Kidney.
Risk Factors and Risk Stratification
One criterion alone is sufficient for high risk:
- BMI < 16 kg/m²
- Unintentional weight loss > 15% over the last 3-6 months
- Nil or negligible oral intake for > 10 days
- Low potassium, phosphate, or magnesium before feeding
Two or more of the following also confer high risk:
- BMI < 18.5 kg/m²
- Weight loss > 10% over 3-6 months
- Nil or negligible intake for > 5 days
- History of alcohol abuse or use of insulin, chemotherapy, antacids, or diuretics
(Bailey & Love's Short Practice of Surgery 28e)
High-risk comorbidities include: anorexia nervosa, chronic alcoholism, cancer, AIDS, diabetes mellitus, post-bariatric surgery, kwashiorkor, chronic diarrhoea or fistula losses. Even short periods of starvation can precipitate the syndrome in these groups.
Clinical Features
Onset is typically within 4-7 days of starting nutrition. Features arise from the combined effects of electrolyte depletion and thiamine deficiency:
| System | Manifestations |
|---|---|
| Cardiovascular | Arrhythmias (most common cause of death), heart failure, oedema, cardiac arrest |
| Respiratory | Respiratory failure (diaphragm weakness from hypophosphataemia) |
| Neurological | Confusion, coma, seizures, Wernicke's encephalopathy (thiamine deficiency) |
| Musculoskeletal | Muscle weakness, rhabdomyolysis |
| Metabolic | Hypophosphataemia, hypokalaemia, hypomagnesaemia, hypocalcaemia, lactic acidosis |
| Endocrine | Hyperglycaemia (from blunted basal insulin secretion) |
(K.J. Lee's Essential Otolaryngology; Goldman-Cecil Medicine; Yamada's Textbook of Gastroenterology)
Prevention and Management
Before Starting Nutrition
- Screen all patients at risk using the criteria above
- Correct pre-existing electrolyte deficits (phosphate, potassium, magnesium, calcium) before beginning any nutritional support
- Thiamine first: Give thiamine 100 mg IV/PO before initiating feeding or any glucose-containing fluids. In severe starvation or chronic alcoholism, continue 100 mg/day for 5-7 days. This prevents Wernicke's encephalopathy
- Administer B-complex multivitamins and trace elements
(Schwartz's Principles of Surgery 11e; Tietz Textbook of Laboratory Medicine 7e)
Feeding Protocol
- Start at 10 kcal/kg/day (or 50% of estimated requirements) - not full caloric targets
- For highest-risk patients (prolonged starvation, chronic fistula losses), begin at < 10 kcal/kg/day
- Increase gradually to meet full requirements over 4-7 days
- For PN, provide only 50% of the dextrose requirement on day 1
- Include adequate phosphate in PN formulas: 20-30 mmol of inorganic phosphate per litre - higher amounts needed in diabetes and chronic alcoholism
(Yamada's; Sabiston; Brenner & Rector's The Kidney)
Monitoring
- Serum electrolytes (phosphate, potassium, magnesium) - monitor frequently, especially in the first week
- Blood glucose, fluid balance, vital signs daily
- Any deficit identified must be aggressively repleted as it appears
- If refeeding syndrome develops: reduce caloric delivery, then slowly advance once electrolytes are stabilised
Key Electrolyte Targets
| Electrolyte | Normal range | Action if low |
|---|---|---|
| Phosphate (Pi) | 0.8-1.5 mmol/L | IV/PO phosphate; ensure 20-30 mmol/L in PN |
| Potassium | 3.5-5.0 mmol/L | IV/PO potassium replacement |
| Magnesium | 0.7-1.0 mmol/L | IV/PO magnesium; hypomagnesaemia worsens hypokalaemia |
| Calcium | 2.1-2.6 mmol/L | Replace if symptomatic |
Recent Evidence (2024-2026)
Three recent systematic reviews are worth noting:
- A 2026 meta-analysis (PMID: 41735500) examined incidence and mortality of refeeding syndrome in critically ill patients - confirming it remains a significant clinical problem in the ICU
- A 2025 systematic review (PMID: 39187889) identified key risk factors for development in adults, reinforcing current screening criteria
- A 2024 systematic review (PMID: 39317131) specifically addressed nutritional therapy strategies in ICU patients at risk, supporting the low-and-slow caloric approach
Summary
Refeeding syndrome results from insulin-driven intracellular electrolyte shifts when carbohydrates are reintroduced after starvation. The triad of hypophosphataemia + hypokalaemia + hypomagnesaemia, compounded by thiamine deficiency, drives multi-organ dysfunction. Prevention hinges on risk identification, thiamine supplementation before feeding, starting low (10 kcal/kg/day), and aggressive electrolyte monitoring and replacement during the first week of nutrition.
Sources: Bailey & Love's Short Practice of Surgery 28e | Yamada's Textbook of Gastroenterology 7e | Sabiston Textbook of Surgery | Schwartz's Principles of Surgery 11e | Goldman-Cecil Medicine | K.J. Lee's Essential Otolaryngology | Brenner & Rector's The Kidney | Tietz Textbook of Laboratory Medicine 7e
This is a shared conversation. Sign in to Orris to start your own chat.