Cerebral lesion of Epilepsy MRI image give
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the information and image URLs needed. Let me compile a comprehensive answer with all the MRI images of cerebral lesions in epilepsy.
Cerebral Lesions in Epilepsy - MRI Findings
Source: Grainger & Allison's Diagnostic Radiology (Chapter 59 - Epilepsy Imaging)
Overview
MRI is the gold standard for identifying structural brain lesions in epilepsy, with ~85% sensitivity for lesion detection in intractable epilepsy. The main role of MRI is to identify an underlying brain abnormality, characterise the pathological substrate, and guide surgical planning.
Dedicated MRI Protocol for Epilepsy includes:
- 3D T1 (1 mm isotropic)
- T2/STIR axial + coronal (≤3 mm)
- FLAIR axial + coronal (≤3 mm)
- Haemosiderin/calcium-sensitive sequence (GRE/SWI)
Categories of Epileptogenic Cerebral Lesions
1. Malformations of Cortical Development (MCD)
Account for up to 50% of paediatric and 25% of young adult intractable epilepsy cases.
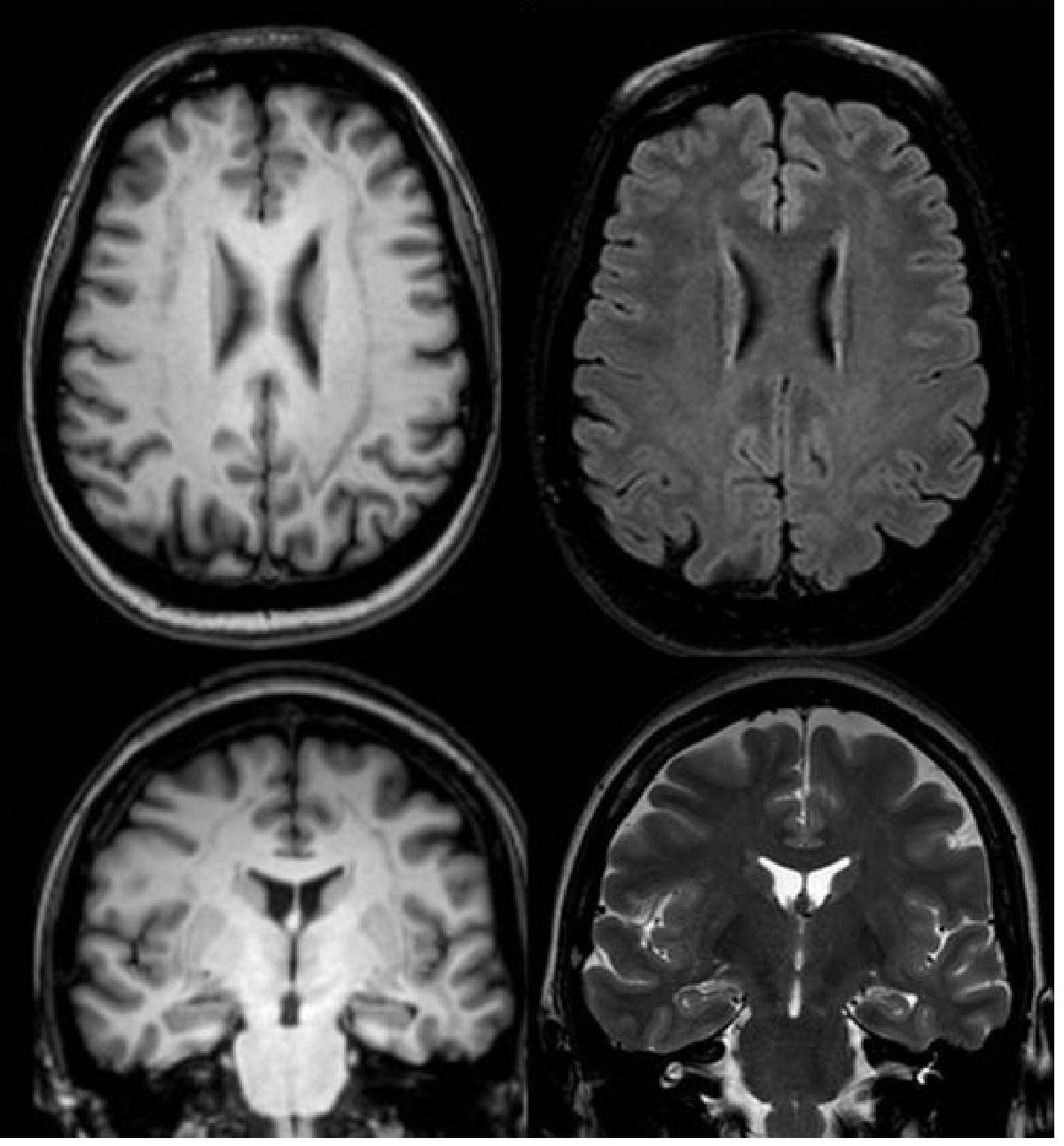
Focal Cortical Dysplasia (FCD) / Abnormal Gyration
MRI shows abnormal cortex with:
- Thickened cortex or abnormal gyri
- Faint cortical T2 hyperintensity
- Blurring of grey-white matter differentiation
- Abnormal sulci
Fig. 59.11 - Focal Cortical Dysplasia (right sylvian fissure/insula):
Band Heterotopia
Neurons in abnormal locations (subcortical band of grey matter). Mild form of lissencephaly. Shows same signal as cortical grey matter on all sequences.
Fig. 59.12 - Band Heterotopia (bilateral cerebral hemispheres):
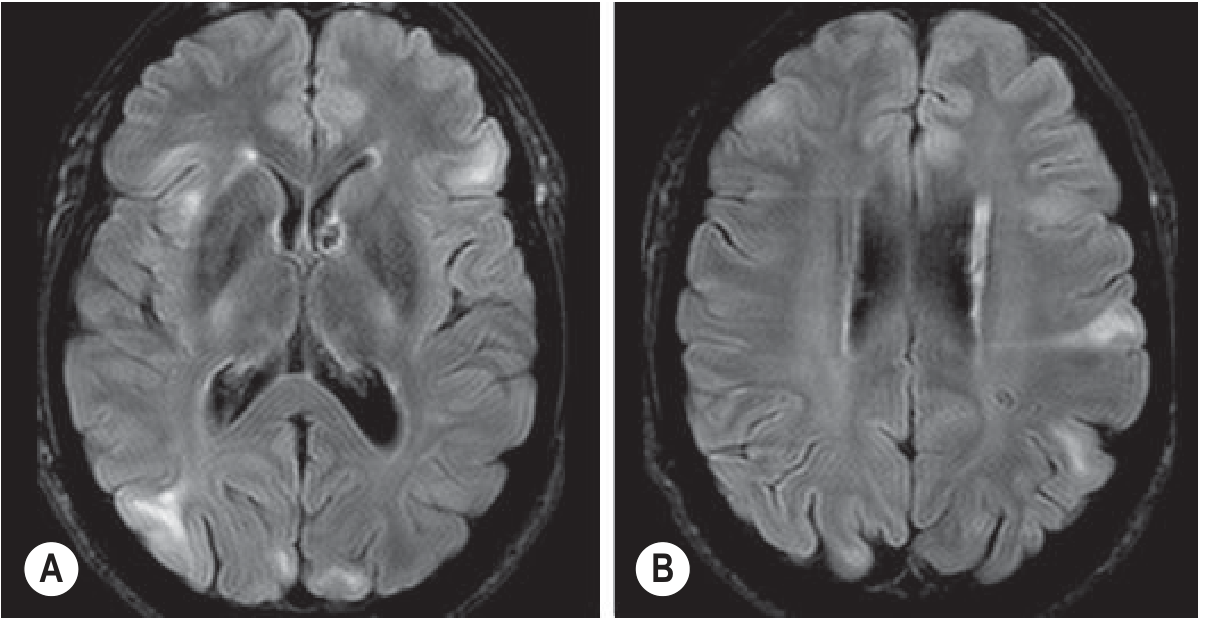
2. Tuberous Sclerosis Complex
~90% of patients develop seizures; 25-30% develop intractable epilepsy.
MRI findings:
- Cortical/subcortical tubers - hyperintense on T2/FLAIR
- Subependymal nodules on lateral ventricular walls
- Subependymal giant cell astrocytomas (can cause hydrocephalus)
- White matter radial migration lines
Fig. 59.13 - Tuberous Sclerosis:
3. Sturge-Weber Syndrome (Vascular/Neurocutaneous)
Facial port-wine stain + ipsilateral meningeal angiomatosis. Clinically: intractable seizures, hemiparesis, hemianopsia.
MRI findings:
- Pial angiomas (predominantly hypointense) in parieto-occipital regions
- Cortical calcifications on T2*/GRE
- Ipsilateral cerebral hemisphere atrophy
- Enlarged choroid plexus
Fig. 59.14 - Sturge-Weber Syndrome:
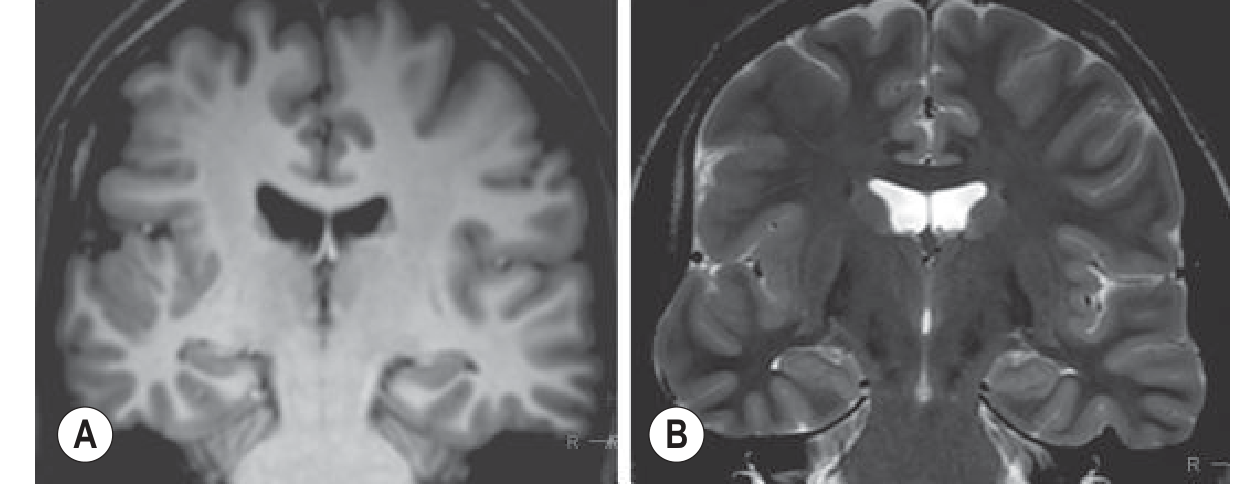
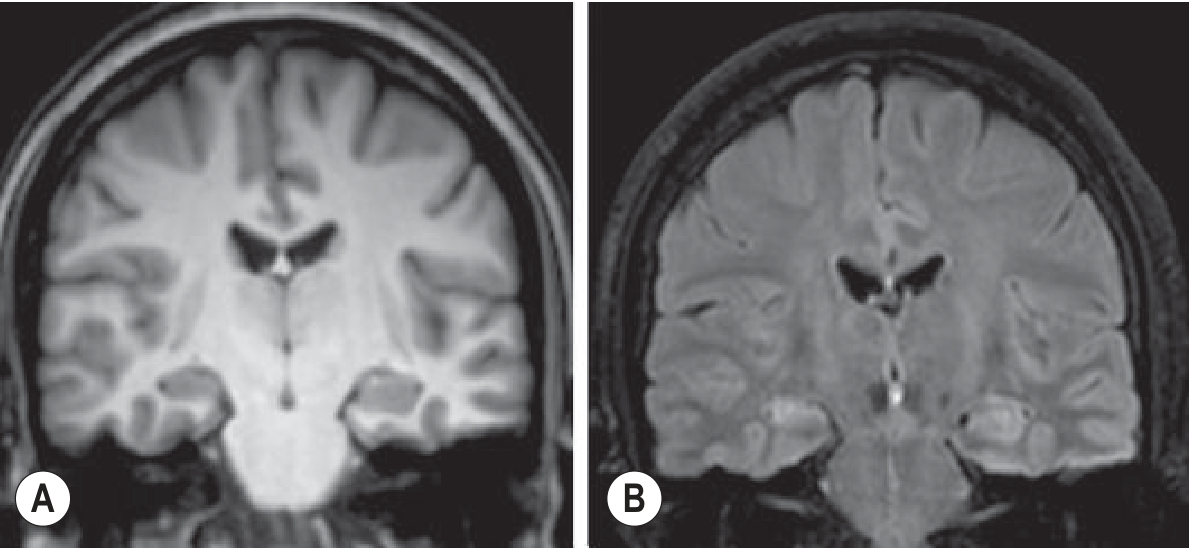
4. Hippocampal Sclerosis
The most common abnormality in temporal lobe resections for intractable epilepsy. Pathology: neuronal loss + gliosis. MRI identifies up to 90% of cases.
MRI findings:
- Hippocampal volume loss (best seen on coronal T1)
- Increased T2/FLAIR signal in the small hippocampus
- Loss of internal hippocampal architecture
- Atrophy of ipsilateral mammillary body and fornix
- Dilatation of adjacent temporal horn
Surgery is curative in up to 70% of patients.
Fig. 59.15 - Hippocampal Sclerosis (right):
5. Tumours (Epilepsy-Associated Neoplasms)
Found in ~4% of epilepsy patients; ~70% are in the temporal lobe.
Common types: Low-grade astrocytoma, Ganglioglioma, DNET, Oligodendroglioma, Pleomorphic xanthoastrocytoma
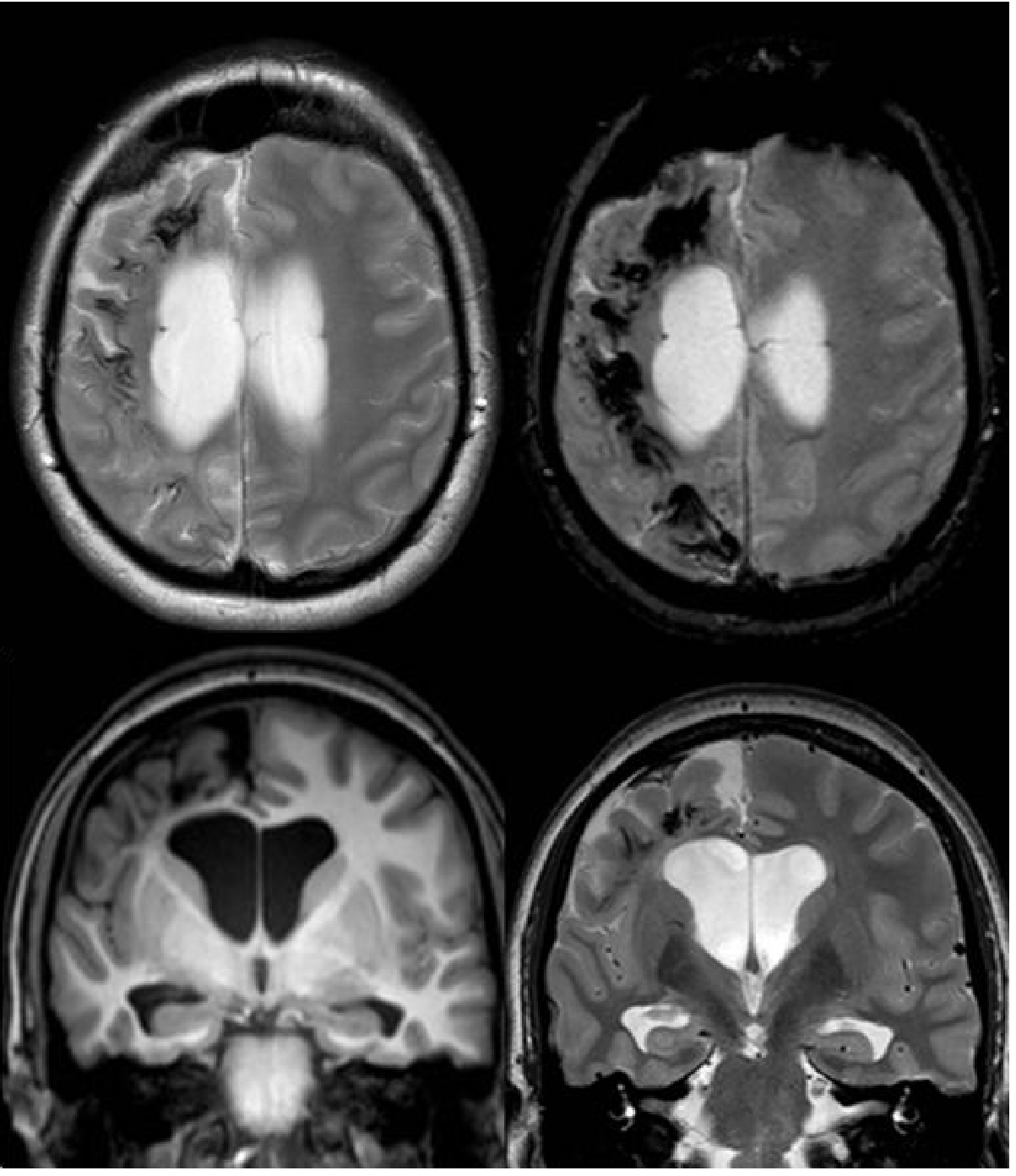
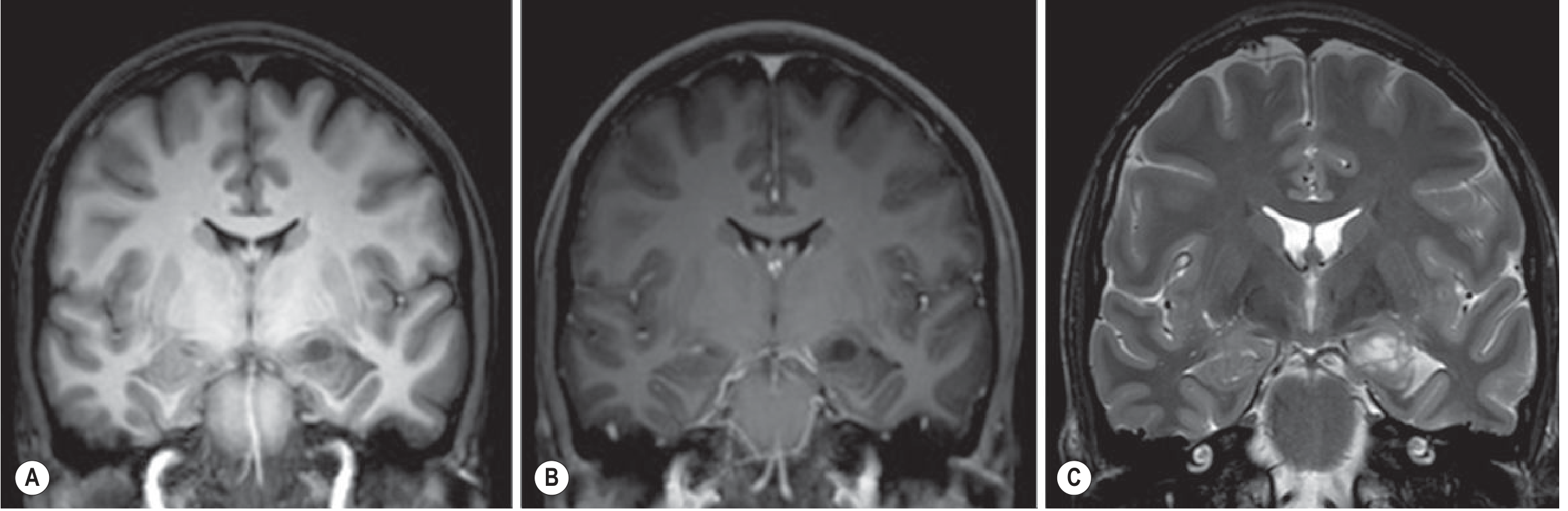
DNET (Dysembryoplastic Neuroepithelial Tumour)
- Cortically based, multicystic, low-grade
- Occurs in children/young adults
- T1: heterogeneously hypointense with cystic component
- T2: heterogeneously hyperintense
- No contrast enhancement (in most cases)
Fig. 59.16 - DNET in left medial temporal lobe:
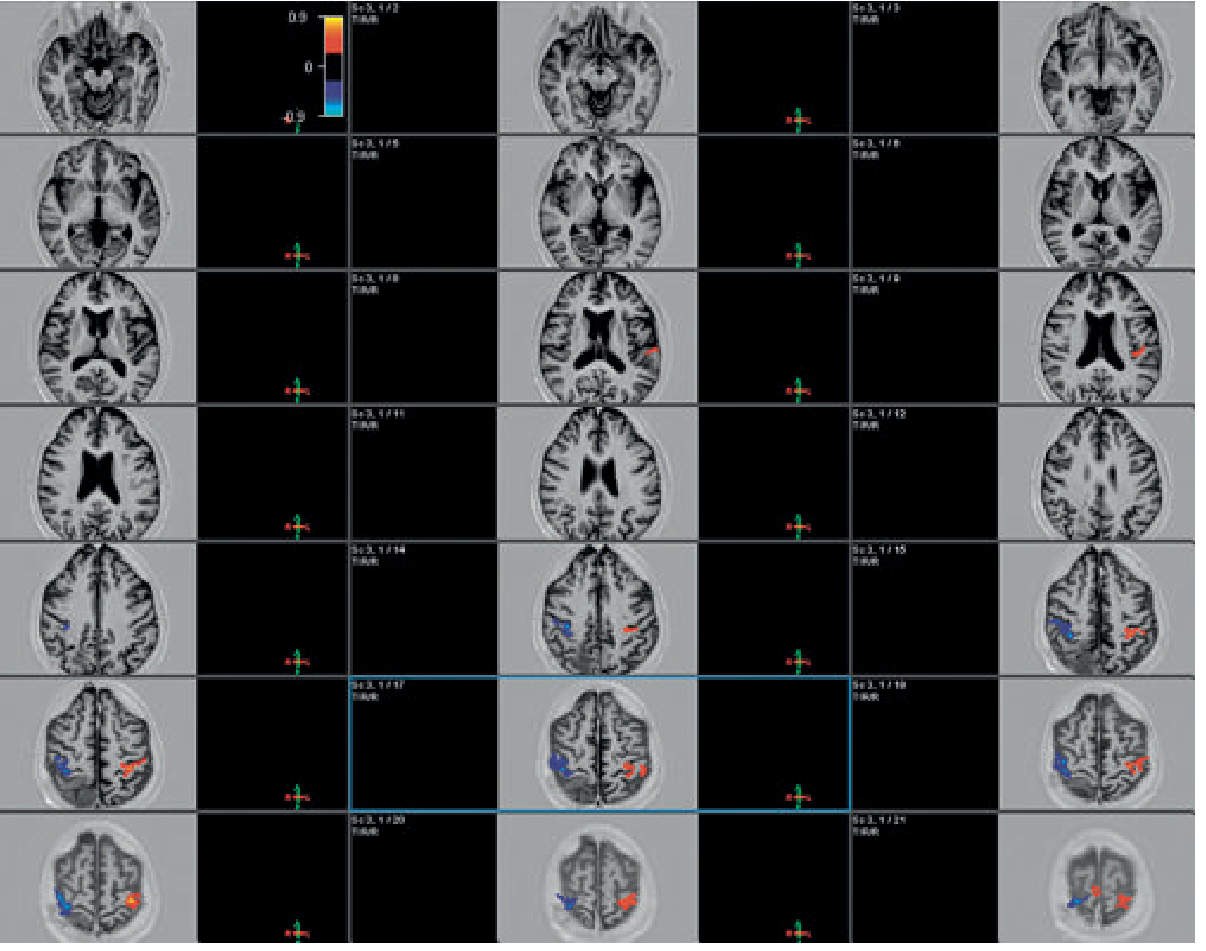
fMRI for Surgical Planning (Tumour-Related Epilepsy)
Fig. 59.17 - fMRI Motor Mapping (tumour adjacent to motor cortex):
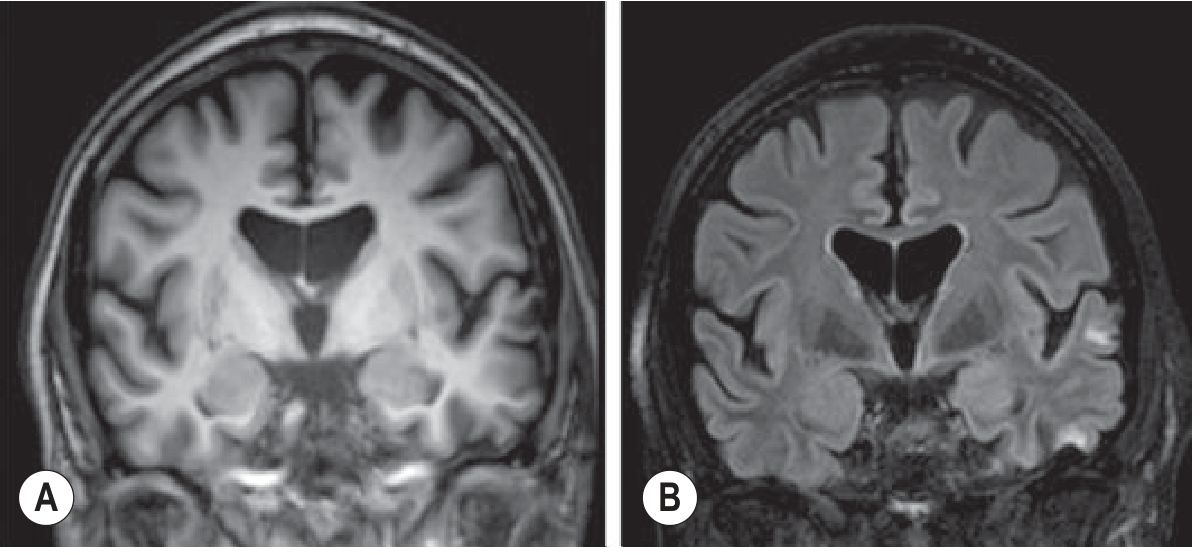
6. Post-Traumatic Epilepsy
Head injury leaves haemosiderin deposits and gliosis (especially in frontal and temporal lobes), which are epileptogenic. MRI (SWI/GRE) is best for detecting haemosiderin.
Fig. 59.18 - Post-Traumatic Epilepsy:
Summary Table
| Lesion Type | Key MRI Findings | Epilepsy Prevalence |
|---|---|---|
| Focal Cortical Dysplasia | Thick cortex, blurred GM-WM junction, T2 hyperintensity | Up to 50% pediatric intractable |
| Band Heterotopia | Subcortical grey matter bands, same signal as cortex | Less common; often drug-resistant |
| Tuberous Sclerosis | Tubers (T2/FLAIR bright), subependymal nodules, migration lines | ~90% have seizures |
| Sturge-Weber | Pial angioma (hypointense), cortical calcification, hemisphere atrophy | Intractable in most |
| Hippocampal Sclerosis | Volume loss + T2 signal ↑ on coronal FLAIR | Most common temporal lobe epilepsy lesion |
| DNET | Cortical cystic mass, T2 bright, no enhancement | Low-grade, young adults |
| Post-traumatic gliosis | Haemosiderin (SWI dark), gliosis (T2 bright) | Depends on injury severity |
- Grainger & Allison's Diagnostic Radiology, Chapter 59 (Epilepsy Imaging), pp. 1494-1497
This is a shared conversation. Sign in to Orris to start your own chat.