Anatomy and surgical importance of infraremporal fossa 20 marks answer for ms ent exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Excellent! I now have all the information needed for a comprehensive 20-mark MS ENT answer. Let me compile the complete answer:
Infratemporal Fossa: Anatomy and Surgical Importance
(20-mark answer for MS ENT examination)
Introduction
The infratemporal fossa (ITF) is a wedge-shaped, clinically vital deep space of the head located inferior to the temporal fossa and between the ramus of the mandible laterally and the pharyngeal wall medially. It is open to the neck posteroinferiorly. Its importance in ENT surgery lies in its complex neurovascular contents, its communications with surrounding spaces, and its involvement in both benign and malignant pathologies requiring skull base surgical approaches.
1. Boundaries
| Wall | Boundary |
|---|---|
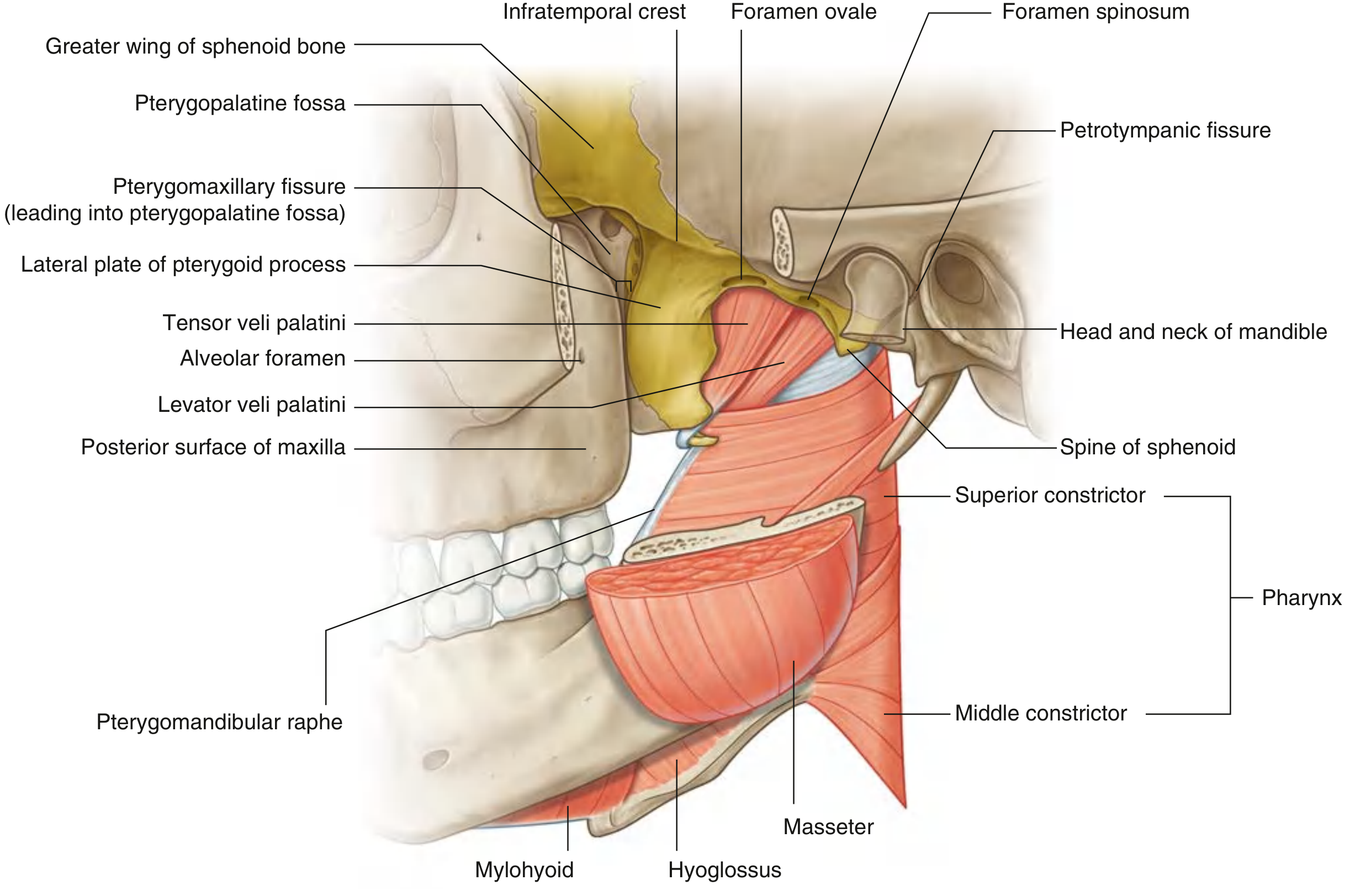
| Roof (superior) | Inferior surfaces of the greater wing of sphenoid and squamous temporal bone; contains foramen ovale, foramen spinosum, and petrotympanic fissure; open superiorly to temporal fossa lateral to the infratemporal crest |
| Anterior | Posterior surface of the maxilla; upper part opens into orbit via inferior orbital fissure; contains alveolar foramen |
| Posterior | Mastoid and tympanic portions of temporal bone |
| Lateral | Medial surface of the ramus of mandible (contains opening of mandibular canal); zygomatic arch |
| Medial | Lateral pterygoid plate anteriorly; pharynx and tensor/levator veli palatini muscles posteriorly; contains the pterygomaxillary fissure (leading to pterygopalatine fossa) |
| Inferior | Open (continuous with the neck); superior limit of posterior belly of digastric and angle of mandible |
2. Communications
The infratemporal fossa communicates with several adjacent spaces - these pathways are of major surgical and pathological importance:
| Structure | Pathway |
|---|---|
| Orbit | Inferior orbital fissure |
| Middle cranial fossa | Foramen ovale and foramen spinosum |
| Pterygopalatine fossa | Pterygomaxillary fissure |
| Temporal fossa | Between zygomatic arch and cranium |
Via its communications, the ITF provides surgical access to the cavernous sinus, sphenoid sinus, nasopharynx, petrous apex, clivus, and parasellar region.
3. Contents
A. Muscles
Lateral Pterygoid:
- Two heads: superior (from roof/infratemporal crest of greater wing of sphenoid) and inferior (from lateral surface of lateral pterygoid plate)
- Both portions insert onto the temporomandibular joint (articular disc and neck of condyle)
- Action: Protrusion of mandible; depression when acting bilaterally; side-to-side chewing
- Innervation: Nerve to lateral pterygoid (from V3)
Medial Pterygoid:
- Deep head: from medial surface of lateral pterygoid plate and pyramidal process of palatine bone
- Superficial head: from tuberosity of maxilla
- Insertion: Roughened medial surface of angle and ramus of mandible
- Action: Elevation and protrusion of mandible
- Innervation: Nerve to medial pterygoid (from V3)
Also present: Lower fibres of temporalis inserting on the coronoid process pass through this space.
B. Nerves
Mandibular nerve (V3) - the most important nerve in the ITF:
- Enters through foramen ovale
- Divides into anterior (mainly motor) and posterior (mainly sensory) trunks
- Motor branches: to all four muscles of mastication (masseter, temporalis, both pterygoids) + tensor tympani + tensor veli palatini
- Sensory branches:
- Auriculotemporal nerve - carries secretomotor fibres to parotid (via otic ganglion); also sensory to TMJ, external auditory canal, and skin of temporal region
- Inferior alveolar nerve - enters mandibular foramen; gives off motor branch to mylohyoid; provides sensation to lower teeth and lower lip (mental nerve)
- Lingual nerve - sensory to anterior 2/3 of tongue; joined by chorda tympani in the fossa
- Buccal nerve - sensory to cheek mucosa
Chorda tympani (branch of CN VII):
- Enters the ITF via the petrotympanic fissure
- Passes vertically and medially to the lateral pterygoid to join the lingual nerve
- Carries taste from anterior 2/3 of tongue and preganglionic parasympathetic secretomotor fibres to submandibular and sublingual glands
- Surgical importance: At risk during TMJ surgery, parotid approaches, and infratemporal dissections
Otic Ganglion:
- Lies medial to V3 just below foramen ovale
- Preganglionic parasympathetic input: lesser petrosal nerve (CN IX)
- Postganglionic fibres carried by the auriculotemporal nerve to the parotid gland
- Sympathetic input: from plexus on middle meningeal artery
Lesser petrosal nerve:
- From tympanic branch of CN IX (Jacobson's nerve)
- Passes through the middle ear and exits foramen ovale/small canal to reach the otic ganglion
C. Arteries
Maxillary artery (internal maxillary artery):
- Terminal branch of the external carotid artery
- Arises posterior to the neck of the mandible
- Passes lateral to the lateral pterygoid muscle into the ITF
- Courses anterior to the pterygomaxillary fissure and enters the pterygopalatine fossa
- Three parts/portions with branches:
| Part | Location | Key Branches |
|---|---|---|
| 1st (mandibular) | Behind neck of mandible | Deep auricular, anterior tympanic, middle meningeal, accessory meningeal, inferior alveolar |
| 2nd (pterygoid) | Superficial/deep to lateral pterygoid | Deep temporal (anterior & posterior), pterygoid branches, masseteric, buccal |
| 3rd (pterygopalatine) | Pterygopalatine fossa | Posterior superior alveolar, infraorbital, descending palatine, artery of pterygoid canal, sphenopalatine |
Middle meningeal artery - enters foramen spinosum; of critical surgical importance (epidural haematoma)
D. Veins
Pterygoid venous plexus:
- Dense network of veins surrounding the lateral pterygoid muscle
- Drains posteriorly into the maxillary vein (to retromandibular vein) and anteriorly into the facial vein
- Anastomoses with: cavernous sinus (via emissary veins through foramen ovale/spinosum), ophthalmic veins, pharyngeal venous plexus
- Surgical/clinical significance: Infection in the ITF can spread haematogenously via this plexus to the orbit (orbital cellulitis) and to the cavernous sinus (cavernous sinus thrombosis), with potentially fatal consequences
4. Pathology Involving the Infratemporal Fossa
The following conditions primarily involve or spread to the ITF in ENT practice:
- Juvenile nasopharyngeal angiofibroma (JNA) - Stage III/IV disease extends to the ITF (Andrews/Sessions staging)
- Deep lobe parotid tumours - extend medially into the prestyloid parapharyngeal/ITF space
- Glomus jugulare tumours - extend inferiorly into the ITF
- Nasopharyngeal carcinoma - lateral extension to the ITF via the sinus of Morgagni
- Maxillary sinus carcinoma (T4) - posterior extension into the ITF
- Cholesteatoma / petrous apex disease - surgical access via ITF approaches
- Trigeminal neuralgia - ITF is the approach zone for V3 block and percutaneous procedures
- Mandibular nerve block - performed in the ITF for lower dental anaesthesia
5. Surgical Importance and Approaches
Fisch Infratemporal Fossa Approaches
Ugo Fisch developed the landmark lateral skull base approaches to the ITF, classified as Types A, B, and C:
Type A (Postauricular - Access to temporal bone/jugular foramen)
Indications:
- Glomus jugulare/tympanicum tumours
- Squamous cell carcinoma of temporal bone
- Salivary gland cancers
- Cholesteatoma with complications
- Neurinoma (schwannoma) of jugular foramen
- Meningioma, rhabdomyosarcoma
Key steps:
- Large C-shaped postauricular incision extending into temporal scalp and into the neck
- Flap elevation superficial to temporalis, SCM, and postauricular muscles
- EAC transected at bony-cartilaginous junction; meatal skin everted and closed
- Anteriorly based mastoid periosteal flap reinforces closed EAC
- Radical mastoidectomy - removal of osseous EAC, all air cells lateral to otic capsule
- Stapes suprastructure removed; Eustachian tube obliterated
- Facial nerve skeletonised from geniculate ganglion to stylomastoid foramen and anteriorly translocated
- Mastoid tip removed; SCM detached
- Cervical dissection exposing CN IX, X, XI, XII, internal carotid artery, internal jugular vein
- Internal carotid artery dissected from neck to skull base
Type B (Access to petrous apex and clivus)
Indications:
- Chordoma, chondroma of clivus
- Dermoid/epidermoid cysts
- Meningioma, craniopharyngioma, plasmacytoma
- Squamous cell carcinoma of petrous apex
- Arachnoid cyst
Type C (Access to parasellar region and nasopharynx)
Indications:
- Advanced JNA (Stage III/IV)
- Salvage surgery for nasopharyngeal SCC
- Adenoid cystic carcinoma around the Eustachian tube
- Parasellar tumours
Preauricular Approaches (Anterolateral)
Provide access to: jugular bulb, ICA, petrous apex, clivus, pterygomaxillary fossa, and nasopharynx. Particularly useful for paramedian lesions involving the clivus, parasellar area, pterygomaxillary fossa, and nasopharynx.
Endoscopic Endonasal Approaches
Increasingly used as an alternative for paramedian lesions involving the clivus, parasellar area, pterygopalatine fossa, nasopharynx, and occasional ITF involvement - avoiding the morbidity of open lateral approaches.
6. Surgical Hazards in ITF Surgery
| Structure at Risk | Consequence of Injury |
|---|---|
| Facial nerve (CN VII) | Facial paralysis - requires anterior transposition in Type A |
| Internal carotid artery | Life-threatening haemorrhage |
| Internal jugular vein | Major haemorrhage, air embolism |
| Mandibular nerve (V3) | Anaesthesia/paraesthesia of lower face, jaw, tongue |
| Chorda tympani | Loss of taste (anterior 2/3 tongue), dry mouth |
| Maxillary artery branches | Haemorrhage; embolisation sometimes required preoperatively |
| Pterygoid venous plexus | Significant venous bleeding; route of septic spread |
| CN IX, X, XI, XII | Lower cranial nerve palsies (type A approach) |
7. Clinical Points for ENT Practice
- Trismus (restricted jaw opening) is a key clinical sign of ITF involvement by tumour or infection, as the pterygoid muscles are encased in this space.
- Infection in the ITF (e.g., from third molar periapical abscess, parapharyngeal abscess) can track to the orbit and cavernous sinus via the pterygoid venous plexus - a surgical emergency.
- Referred otalgia via the auriculotemporal nerve (branch of V3) is a presenting feature of ITF tumours.
- V3 blocks and otic ganglion blocks for pain management are performed within the ITF, guided by imaging or landmark technique.
- JNA staging specifically documents ITF extension as this determines surgical approach and resectability.
- Preoperative angiography and embolisation of the maxillary artery branches are often performed before ITF tumour surgery to reduce intraoperative blood loss.
Summary Table
| Category | Key Points |
|---|---|
| Boundaries | Roof: greater wing of sphenoid + squamous temporal; Lateral: ramus of mandible; Medial: lateral pterygoid plate + pharynx; Anterior: posterior maxilla |
| Contents | Pterygoid muscles, V3 + branches, chorda tympani, otic ganglion, maxillary artery + branches, pterygoid venous plexus |
| Communications | Orbit, middle cranial fossa, pterygopalatine fossa, temporal fossa |
| Common pathology | JNA, glomus tumours, deep parotid tumours, NPC extension, maxillary Ca, cholesteatoma |
| Surgical approaches | Fisch Type A (temporal bone), Type B (clivus), Type C (nasopharynx/parasellar) |
| Key hazards | Facial nerve, ICA, IJV, lower cranial nerves, pterygoid venous plexus |
Sources:
- Cummings Otolaryngology Head and Neck Surgery, Chapter 175 (Anatomy of the Infratemporal Fossa) and Chapter 178 (Infratemporal Fossa Approaches)
- K.J. Lee's Essential Otolaryngology, Chapter on Infratemporal Fossa and Surgery of the ITF
- Gray's Anatomy for Students, Head and Neck section
This is a shared conversation. Sign in to Orris to start your own chat.