Literature Review: Physiology and Pathology of the Female Reproductive System, Menstrual Cycle Disorders, and Female Infertility
PART I: PHYSIOLOGY OF THE FEMALE REPRODUCTIVE SYSTEM
1.1 Anatomical Overview
The female reproductive system comprises the ovaries, fallopian tubes, uterus, cervix, and vagina. The ovaries are the primary female gonads, attached to the uterus by ligaments through which ovarian arteries, veins, lymphatics, and nerves travel. The ovary is divided into three zones: the cortex (outermost layer, lined by germinal epithelium, containing all follicles and oocytes), the medulla (middle zone, mixed cell types), and the hilum (inner zone, traversed by blood and lymphatic vessels). The functional unit of the ovary is the ovarian follicle - a single oocyte enclosed by endocrine-active cells - which serves the dual role of oogenesis and steroid hormone secretion. - Costanzo Physiology 7th Ed., p.474
The ovarian steroid hormones (estrogen and progesterone) exert both paracrine (local, within the ovary, supporting oocyte development) and endocrine (systemic, acting on uterus, breast, bone, and other targets) functions. - Costanzo Physiology 7th Ed., p.474
1.2 Neuroendocrine Axis: Hypothalamus-Pituitary-Ovarian (HPO) Axis
The reproductive process in women depends on a carefully orchestrated interaction between the CNS (hypothalamus), the anterior pituitary, and the ovary. Disruption at any level results in reproductive failure. - Berek & Novak's Gynecology, p.264
Hypothalamus. The hypothalamus is a small neural structure at the base of the brain, above the optic chiasm. It is divided into three zones: periventricular, medial (cell bodies), and lateral (axons). It is not isolated - it has multiple interconnections with the limbic system (amygdala, hippocampus), thalamus, and pons, forming feedback loops. The major hypothalamic secretory products are pituitary-releasing factors:
- Gonadotropin-releasing hormone (GnRH): controls LH and FSH secretion
- Thyrotropin-releasing hormone (TRH): controls TSH
- Corticotropin-releasing hormone (CRH): controls ACTH
- Growth hormone-releasing hormone (GHRH): controls GH
- Berek & Novak's Gynecology, p.265-268
GnRH Pulsatility. GnRH is secreted in a pulsatile manner - the pulse frequency determines the relative ratio of LH to FSH secretion. Pulsatile GnRH simultaneously regulates both gonadotropins in the pituitary. Continuous (non-pulsatile) GnRH actually suppresses gonadotropin secretion - a fact exploited pharmacologically by GnRH agonists. - Berek & Novak's Gynecology, p.264
Feedback Loops. Three levels of feedback to the hypothalamus operate:
- Long feedback loop - circulating estrogens and androgens feed back onto steroid receptors in the hypothalamus
- Short feedback loop - pituitary hormones feed back directly to the hypothalamus
- Ultrashort feedback loop - hypothalamic secretions feed back onto the hypothalamus itself
- Berek & Novak's Gynecology, p.267
Anterior Pituitary. In the pituitary, FSH and LH (gonadotropins) are produced by gonadotroph cells. They act on the ovary in a defined, sequential manner to produce follicular growth, ovulation, and corpus luteum formation. - Berek & Novak's Gynecology, p.264
1.3 Oogenesis
In the developing ovaries, primordial germ cells produce oogonia by mitotic division until gestational weeks 20-24, reaching a maximum of approximately 7 million oogonia. From weeks 8-9 of gestation, some oogonia enter prophase of meiosis and become primary oocytes. This process continues until approximately 6 months after birth, at which point all oogonia have become primary oocytes. The oocytes remain in a state of suspended prophase (meiotic arrest) - the first meiotic division is not completed until ovulation, which may occur many years later.
Simultaneously, atresia progressively reduces the oocyte pool:
- Gestational week 20-24: ~7 million oogonia
- At birth: ~2 million oocytes
- At puberty: ~400,000 oocytes
- At menopause: few if any oocytes remain
Unlike males, females do not produce new oogonia; reproduction depends on a fixed, continuously declining pool of oocytes. - Costanzo Physiology 7th Ed., p.475
1.4 Folliculogenesis (Ovarian Follicular Development)
Follicular development occurs in three stages:
Stage 1 (Primordial → Primary Follicle). This stage parallels the prolonged prophase of the primary oocyte, lasting 13-50 years. The primary oocyte grows; granulosa cells proliferate and nurture the oocyte with nutrients and steroid hormones; theca interna cells develop; granulosa cells begin secreting fluid. No follicle progresses beyond this stage in prepubertal ovaries.
Stage 2 (Primary → Graafian Follicle). This stage occurs over 70-85 days and is present only during the reproductive period. During each menstrual cycle, a cohort of follicles enters this sequence. Antral fluid (containing steroid hormones, mucopolysaccharides, proteins, and FSH) accumulates centrally. Granulosa and theca cells continue to grow. At completion, the follicle is termed a Graafian follicle, 2-5 mm in diameter.
Stage 3 (Graafian → Dominant Follicle → Ovulation). This stage is most rapid, occurring 5-7 days after menses. A single Graafian follicle achieves dominance; its cohorts regress (atresia). Within 48 hours, the dominant follicle grows to 20 mm in diameter. On day 14 of a 28-day cycle, ovulation occurs: the dominant follicle ruptures, releasing the secondary oocyte into the peritoneal cavity. The oocyte enters the fallopian tube, where it begins the second meiotic division. If fertilization occurs, the second meiotic division is completed, yielding the haploid ovum with 23 chromosomes. - Costanzo Physiology 7th Ed., p.475-476
Two-cell, Two-gonadotropin Model. The theca cells, stimulated by LH, produce androgens (primarily androstenedione and testosterone). These androgens are transferred to adjacent granulosa cells, where aromatase enzymes (FSH-stimulated) convert them to estrogens - primarily estradiol (E2). This two-cell model explains why both FSH and LH are required for estrogen synthesis. - Berek & Novak's Gynecology; Tietz Lab Medicine
1.5 Corpus Luteum Formation and Function
After ovulation, the residual elements of the ruptured follicle form the corpus luteum (yellow body). It is composed primarily of granulosa cells but also theca cells, capillaries, and fibroblasts. The corpus luteum synthesizes and secretes progesterone and estrogen, which are necessary for endometrial preparation and maintenance of pregnancy.
- If fertilization does not occur: the corpus luteum degenerates into the corpus albicans (white scar tissue) over approximately 14 days; estrogen and progesterone fall; FSH rises again to begin a new cycle.
- If fertilization does occur: hCG produced by the trophoblast maintains the corpus luteum until the placenta takes over steroid synthesis (at approximately 10-12 weeks). - Costanzo Physiology 7th Ed., p.476
PART II: THE MENSTRUAL CYCLE - PHYSIOLOGY
The normal menstrual cycle lasts 21 to 35 days (average 28 days), with 2-6 days of flow and 20-60 mL average blood loss. Cycle length variability is primarily due to variability in the follicular phase; the luteal phase is relatively constant at approximately 14 days. - Berek & Novak's Gynecology, p.280
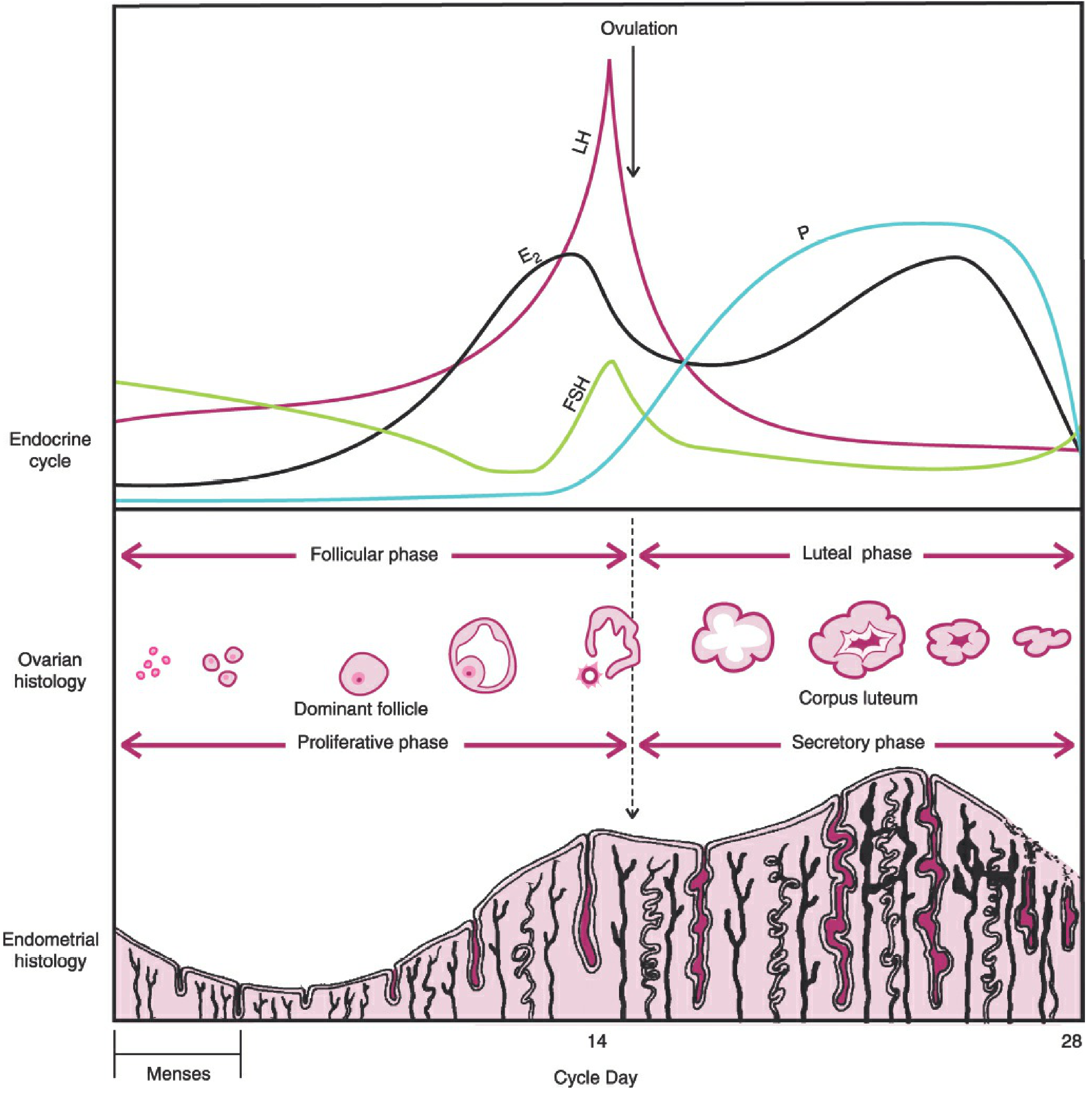
The menstrual cycle. The endocrine cycle (top) shows cyclic changes of LH, FSH, estradiol (E2), and progesterone (P) relative to ovulation. The middle panel shows ovarian histology (follicular and luteal phases). The bottom panel shows corresponding endometrial histology (proliferative and secretory phases). - Berek & Novak's Gynecology, Fig. 7-9
2.1 Phases of the Menstrual Cycle
Phase 1: Follicular Phase (Proliferative Phase) - Days 1-14
Day 1 is defined as the first day of menstrual bleeding. As the previous corpus luteum regresses, estrogen and progesterone concentrations fall. Rising FSH (from reduced inhibin/estrogen feedback) recruits a cohort of growing follicles. These follicles secrete increasing estrogen, which drives endometrial proliferation (growth of the functionalis layer, glands, stroma, and spiral arteries). Rising estrogen also causes cervical mucus to become copious, watery, elastic ("ferning" pattern on glass), creating channels that facilitate sperm passage. - Costanzo Physiology 7th Ed., p.479
As follicles grow, rising estrogen and inhibin B suppress FSH (negative feedback), ensuring only the dominant follicle - which has the most FSH receptors - continues growing while others undergo atresia.
The LH Surge and Ovulation. Late in the follicular phase, when estrogen exceeds a threshold for a sufficient duration, it switches from negative to positive feedback on the pituitary - the biphasic response. This triggers the dramatic midcycle LH surge (the proximate cause of ovulation), with ovulation occurring 24-36 hours after the surge onset. The LH surge begins 16-58 hours before ovulation in 90% of women. FSH also surges at midcycle, inducing LH receptors on granulosa cells. - Berek & Novak's Gynecology, p.281; Tietz Lab Medicine, p.2215
Phase 2: Luteal Phase (Secretory Phase) - Days 15-28
After ovulation, the corpus luteum produces increasing amounts of progesterone and estrogen. Progesterone dominates this phase, causing:
- Slowing of endometrial proliferation; decreased endometrial thickness
- Uterine glands become tortuous and accumulate glycogen vacuoles; increased mucus secretion
- Edema of the endometrial stroma
- Spiral arteries elongate and coil
- Cervical mucus thickens, becomes non-elastic and non-ferning (hostile to sperm)
- A mild thermogenic effect, raising basal body temperature by 0.2-0.5°F (0.1-0.3°C) - the basis of the basal body temperature method of fertility awareness
- Costanzo Physiology 7th Ed., p.479
Progesterone, estrogen, and inhibin A from the corpus luteum suppress gonadotropin secretion (long feedback). Progesterone peaks approximately 8 days after ovulation (days 21-23, midluteal phase). If conception does not occur, the corpus luteum involutes, hormone levels fall, endometrial ischemia occurs, and menstruation begins, resetting the cycle. - Berek & Novak's Gynecology, p.281; Tietz Lab Medicine, p.2218
2.2 Endometrial Cycling (Uterine Cycle)
The endometrium is divided into:
- Decidua functionalis (superficial two-thirds): proliferates monthly and is shed at menstruation. Consists of the stratum spongiosum (deep intermediate zone) and stratum compactum (superficial compact zone).
- Decidua basalis (deepest layer): does not undergo significant monthly cycling; serves as the source of endometrial regeneration after each menses.
The existence of endometrial stem cells (residing in bone marrow and migrating to the basalis) has been demonstrated - they provide the regenerative capacity of the endometrium. - Berek & Novak's Gynecology, p.282
The histologic changes in the endometrium - as described by Noyes, Hertig, and Rock (1950) - proceed in orderly fashion in response to cyclic hormonal production and can be used to "date" the endometrium in diagnostic biopsies.
PART III: PATHOLOGY OF THE FEMALE REPRODUCTIVE SYSTEM AND MENSTRUAL CYCLE
Disorders of menstrual physiology may lead to various pathologic states, including infertility, recurrent miscarriage, and malignancy. As stated in Berek & Novak's Gynecology: "In the normal menstrual cycle, orderly cyclic hormone production and parallel proliferation of the uterine lining prepare for implantation of the embryo. Disorders of the menstrual cycle and, likewise, disorders of menstrual physiology, may lead to various pathologic states, including infertility, recurrent miscarriage, and malignancy."
3.1 Disorders of Ovulation
Anovulation is the failure to release an oocyte and is the single most common cause of female infertility. It may be due to:
a) Polycystic Ovary Syndrome (PCOS)
PCOS is the single most common endocrine abnormality of women of reproductive age, affecting approximately 5-10% of women. It is the most common cause of anovulatory infertility. Women with PCOS present with: abnormal menses (oligomenorrhea/amenorrhea), infertility, hirsutism, acne, and obesity - all related to excess androgen. The pathophysiology involves hyperandrogenism, insulin resistance, and dysregulation of LH/FSH secretion (typically elevated LH:FSH ratio). - Textbook of Family Medicine 9e, p.1052
Recent reviews (
Joham et al., Lancet Diabetes Endocrinol, 2022, PMID: 35934017;
Stener-Victorin et al., Nat Rev Dis Primers, 2024, PMID: 38637590) confirm the genetic, neuroendocrine, and metabolic complexity of PCOS, emphasizing its heterogeneous presentation. Hormonal hallmarks include elevated androgens, dysregulated estrogen secretion, and altered gonadotropin pulsatility (
Yang & Chen, J Endocrinol, 2024, PMID: 38285626).
b) Hyperprolactinemia
Excess prolactin (due to prolactinoma, drugs - antipsychotics, antidepressants, opiates; hypothyroidism; or idiopathic) suppresses GnRH pulsatility and thus gonadotropin secretion, leading to anovulation and amenorrhea. Galactorrhea is the clinical correlate (inappropriate milk secretion). - Textbook of Family Medicine 9e, p.1052
c) Hypothalamic Causes (Hypogonadotropic Hypogonadism)
Includes Kallmann syndrome (hypothalamic insufficiency with anosmia), excessive exercise, severe weight loss (anorexia nervosa), and psychogenic stress. These impair GnRH pulse generation, leading to low FSH/LH and anovulation. - Tietz Lab Medicine, p.2763
d) Primary Ovarian Insufficiency (POI)
Previously called premature ovarian failure - defined as hypergonadotropic hypogonadism (high FSH, low estrogen) before age 40. Causes include autoimmune destruction of follicles, gonadotoxic chemotherapy, radiation, chromosomal abnormalities (Turner syndrome), and resistant ovary syndrome.
e) Luteal Phase Deficiency
Inadequate progesterone production by the corpus luteum after ovulation, resulting in inadequate endometrial preparation for implantation. It can cause infertility or early pregnancy loss.
f) Thyroid and Metabolic Disorders
Both hypothyroidism and hyperthyroidism disturb the HPO axis. Thyroid disorders alter sex hormone-binding globulin (SHBG) levels, change the metabolism of estrogens, and disrupt GnRH pulsatility. Obesity and hepatic disease also alter steroid metabolism significantly. - Tietz Lab Medicine, p.2751
3.2 Disorders of the Fallopian Tubes (Tubal Factor Pathology)
Tubal damage accounts for approximately 20% of female infertility. Mechanisms include:
Pelvic Inflammatory Disease (PID): The most common cause of tubal damage. PID results from ascending infection (most commonly
Chlamydia trachomatis and
Neisseria gonorrhoeae) causing salpingitis, peritubal adhesions, and tubal occlusion.
Chlamydia trachomatis is particularly insidious as it often causes subclinical or minimally symptomatic salpingitis (
Horner et al., J Infect Dis, 2021, PMID: 34396401). A single episode of PID confers approximately a 12-15% risk of tubal infertility; three or more episodes raise the risk to 50-75%.
Salpingitis Isthmica Nodosa (SIN): A condition where nodular thickening develops in the isthmic portion of the fallopian tube, associated with diverticulosis of the tubal epithelium, leading to obstruction and an elevated risk of ectopic pregnancy.
Endometriosis-Related Tubal Damage: Peritubal adhesions from endometriosis can distort tubal anatomy and impair oocyte pickup and transport.
3.3 Uterine Pathology
Uterine Leiomyomata (Fibroids):
Benign smooth muscle tumors of the myometrium. Submucosal fibroids distort the endometrial cavity, impairing implantation. Intramural fibroids of sufficient size may compress the endometrial cavity. Treatment is directed by location, size, and reproductive goals. - Tietz Lab Medicine, p.2784
Endometrial Adhesions (Asherman Syndrome):
Intrauterine adhesions (synechiae) typically develop after uterine surgery (especially dilation and curettage following pregnancy complications) or intrauterine infections (endometritis). They obliterate the endometrial cavity, causing amenorrhea, hypomenorrhea, and infertility by preventing implantation.
Congenital Uterine Malformations (Müllerian Anomalies):
Failure of normal development/fusion of the Müllerian ducts leads to anomalies such as unicornuate, bicornuate, septate, or arcuate uterus. These are associated with recurrent pregnancy loss and can impair implantation.
Endometritis:
Chronic endometritis (plasma cell infiltration of the endometrial stroma) disrupts the normal endometrial receptivity cycle, impairing implantation even in the absence of obvious symptoms. It is increasingly recognized as a cause of unexplained infertility and recurrent implantation failure.
3.4 Endometriosis
Endometriosis is defined as the presence of endometrial glands and stroma outside the uterine cavity, most commonly on the ovaries (endometriomas/"chocolate cysts"), peritoneum, fallopian tubes, and uterosacral ligaments. It affects an estimated 6-10% of women of reproductive age and 25-50% of infertile women.
- Sampson's Retrograde Menstruation Theory: retrograde flow of viable endometrial cells through the fallopian tubes into the peritoneal cavity, with subsequent implantation and growth. Most widely accepted.
- Coelomic Metaplasia Theory: metaplastic transformation of peritoneal mesothelium into endometrial tissue.
- Lymphovascular Dissemination Theory: spread of endometrial cells via lymphatics/blood vessels, explaining distant sites.
- Immune dysregulation, particularly impaired natural killer cell activity allowing ectopic implants to survive.
- Peritubal/periovarian adhesions impairing oocyte pickup
- Inflammatory cytokines in peritoneal fluid impairing sperm function and fertilization
- Impaired endometrial receptivity (altered integrin expression)
- Ovarian endometriomas reducing ovarian reserve (destroying surrounding follicles)
- Immune-mediated embryotoxicity
3.5 Cervical Factor Pathology
Cervical stenosis (often post-surgical), chronic cervicitis, or abnormal mucus viscosity can impair sperm transport. Antisperm antibodies in cervical mucus may immobilize or destroy sperm. - Tietz Lab Medicine, p.2777
3.6 Disorders of the Menstrual Cycle (Pathological States)
| Disorder | Definition | Mechanism |
|---|
| Amenorrhea (Primary) | Absence of menses by age 15 (with normal secondary sex characteristics) or 13 (without) | Müllerian agenesis, gonadal dysgenesis (Turner), hypothalamic failure |
| Amenorrhea (Secondary) | Cessation of menses for >3 cycles or >6 months | PCOS, hypothalamic suppression, hyperprolactinemia, POI, pregnancy |
| Oligomenorrhea | Cycles >35 days apart | PCOS, thyroid disease, weight changes |
| Menorrhagia | Heavy or prolonged menstrual bleeding | Fibroids, endometrial polyps, coagulopathy, anovulatory cycles |
| Dysmenorrhea | Painful menstruation | Primary (prostaglandin-mediated) or secondary (endometriosis, fibroids, adenomyosis) |
| Premenstrual Syndrome/PMDD | Physical and emotional symptoms in luteal phase | Progesterone/serotonin interactions |
| Dysfunctional Uterine Bleeding | Abnormal uterine bleeding without structural cause | Anovulatory cycles - unopposed estrogen causing irregular endometrial shedding |
PART IV: INFERTILITY - GENERAL OVERVIEW
4.1 Definition and Epidemiology
Infertility is defined as the failure to conceive after 12 months of regular, unprotected intercourse in women under 35 years. For women over 35 years (or with known risk factors), evaluation is recommended after 6 months. - Textbook of Family Medicine 9e, p.1051
Global prevalence: approximately 15-20% of all couples are affected by infertility at some point. The distribution of causes among infertile couples is approximately:
- Male factors: ~30-35%
- Female factors: ~30-35%
- Combined/unexplained: ~20-30%
- Textbook of Family Medicine 9e, p.1051
Female fertility is age-dependent. It peaks at ages 20-24, declines gradually until age 32, then declines steeply after age 40, and approaches zero after age 45. This decline reflects the diminishing quantity and quality of the remaining oocyte pool. - Textbook of Family Medicine 9e, p.1051
4.2 Classification of Infertility
Infertility is classified as:
- Primary infertility: the couple has never achieved a pregnancy
- Secondary infertility: the couple has previously achieved at least one pregnancy (regardless of outcome), but is currently unable to conceive
PART V: FEMALE PRIMARY INFERTILITY
5.1 Definition
Primary infertility in women refers to infertility in a woman who has never conceived. This implies that no prior fertilization capable of producing a clinically recognized pregnancy has occurred.
5.2 Causes and Categories
The causes of female primary infertility are categorized as follows, with approximate relative frequencies:
5.2.1 Ovarian/Hormonal Factors (~40% of female infertility)
This is the largest single category. Causes include:
- PCOS - most common single endocrine cause; chronic anovulation due to hyperandrogenism and disordered LH/FSH secretion
- Hypothalamic hypogonadotropic hypogonadism - Kallmann syndrome, hypothalamic amenorrhea from exercise/weight loss/stress
- Hyperprolactinemia - prolactinoma, drug-induced
- Primary Ovarian Insufficiency (POI) - autoimmune, chromosomal (Turner syndrome 45,X is a classic cause of primary amenorrhea and primary infertility), gonadotoxic therapy
- Gonadal dysgenesis - chromosomal abnormalities
- Luteal phase deficiency
- Tietz Lab Medicine, p.2748-2766; Textbook of Family Medicine, p.1051
In primary infertility specifically, congenital causes are proportionally more important:
- Müllerian agenesis (Mayer-Rokitansky-Küster-Hauser syndrome) - absence or hypoplasia of the uterus and upper vagina; ovaries present and functional. This is a leading cause of primary amenorrhea and primary infertility.
- Turner syndrome (45,X) - streak gonads replace the ovaries; high FSH/LH; primary amenorrhea; no spontaneous ovulation possible
- Congenital uterine anomalies - septate uterus most common; associated with implantation failure
5.2.2 Tubal Factors (~20% of female infertility)
Even in primary infertility, prior subclinical infection (particularly chlamydia) may have caused silent tubal damage:
- Proximal or distal tubal occlusion
- Hydrosalpinx (distal occlusion causing fluid-filled tube)
- Salpingitis isthmica nodosa
- Peritubal adhesions
5.2.3 Uterine Factors
- Congenital uterine malformations (septate, bicornuate, unicornuate uterus)
- Submucosal fibroids (uncommon as a sole cause of primary infertility but contribute)
5.2.4 Endometriosis
Endometriosis is found in 25-50% of women with unexplained infertility and is a significant cause of primary infertility due to the mechanisms described above.
5.2.5 Cervical Factors
Cervical stenosis (congenital or post-procedural), hostile cervical mucus, or antisperm antibodies.
5.2.6 Unexplained Infertility
Approximately 10-15% of infertile couples have no identifiable cause after complete evaluation.
PART VI: FEMALE SECONDARY INFERTILITY
6.1 Definition
Secondary infertility refers to the inability to conceive or carry a pregnancy to term in a woman who has previously achieved at least one pregnancy (clinical pregnancy, including ectopic, miscarriage, or live birth).
6.2 Distinguishing Features vs. Primary Infertility
Secondary infertility has a distinct epidemiological and aetiological profile:
- Acquired conditions are proportionally more important than congenital ones
- Prior obstetric or gynecological interventions (D&C, caesarean section, pelvic surgery) create specific risk factors not applicable in primary infertility
- Age-related ovarian reserve decline becomes increasingly relevant as the interval between pregnancies lengthens
- Interval infertility (time between pregnancies increasing) is common in populations where child spacing is long
6.3 Causes of Secondary Infertility
6.3.1 Acquired Tubal Factors
- PID between pregnancies - new infection causing tubal scarring
- Puerperal sepsis (post-delivery uterine infection spreading to tubes)
- Post-abortion sepsis
- Ectopic pregnancy and its surgical management (salpingectomy/salpingostomy)
6.3.2 Uterine Factors - Acquired
- Asherman Syndrome (intrauterine adhesions) - the most important uterine cause of secondary infertility; arises after uterine curettage (postpartum hemorrhage, miscarriage management, termination of pregnancy), particularly when performed in the context of infection. Synechiae prevent implantation and cause hypomenorrhea or amenorrhea.
- Endometritis - chronic subclinical endometrial infection after delivery, abortion, or instrumentation
- Submucosal fibroids acquired or growing larger since last pregnancy
- Cervical stenosis from prior procedures (LLETZ/LEEP, cone biopsy, cervical cerclage)
6.3.3 Ovarian Reserve Decline
Age-related decline in oocyte quantity and quality is a significant cause of secondary infertility, especially when the interval since the last pregnancy is 5 or more years. Serum AMH (anti-Müllerian hormone) and FSH on day 3 of the cycle are the primary markers of ovarian reserve.
Treatment guidance from Textbook of Family Medicine: "Women who have secondary infertility (pituitary) wishing to restore fertility should be referred to specialized centers for pharmacologic induction of ovulation with exogenous pulsatile GnRH and exogenous FSH and LH treatment. GnRH can be used to restore fertility when hypothalamic disease and tertiary hypogonadism are present." - p.1404
6.3.4 Endometriosis - Progressive Disease
Endometriosis may be present or worsen between pregnancies. Even if a woman conceived naturally before, progressive endometriosis can cause secondary infertility through ovarian endometrioma formation, worsening adhesions, and declining ovarian reserve.
6.3.5 Medical/Systemic Conditions
New-onset thyroid disease (hypothyroidism, hyperthyroidism), hyperprolactinemia (e.g., prolactinoma developing after first pregnancy), or other metabolic conditions (obesity, insulin resistance) arising after a previous pregnancy.
6.3.6 Male Factor (New)
The partner may have new-onset male factor infertility (a couple evaluation is always necessary even when the problem appears to be female).
PART VII: EVALUATION OF FEMALE INFERTILITY
7.1 Initial Evaluation
A full fertility workup should include history, physical examination, and targeted investigations. Physical examination focuses on:
- External genitalia and hair pattern (signs of androgen excess - hirsutism, clitoromegaly, virilization)
- Pelvic examination (masses, nodularity, tenderness suggestive of endometriosis)
- Breasts (galactorrhea - hyperprolactinemia)
- Neurological findings (anosmia - Kallmann; visual field defects - pituitary macroadenoma)
- Thyroid (enlargement, nodules)
- Body mass index
- Tietz Lab Medicine, p.2805
7.2 Investigations
| Factor | Investigation |
|---|
| Ovulatory factors | Urinary LH predictor kits (LH surge); mid-luteal serum progesterone (day 21-23; >30 ng/dL = ovulation occurred); transvaginal ultrasound; TSH, FSH, prolactin, androgens |
| Ovarian reserve | Day 3 FSH (>12 IU/L = poor response); AMH; antral follicle count on USS |
| Tubal factors | Hysterosalpingography (HSG) - first choice; laparoscopy + chromotubation if history strongly suggests tubal damage |
| Uterine factors | Transvaginal USS; sonohysterography (for submucous fibroids, polyps); hysteroscopy; MRI |
| Cervical factors | Cervical mucus evaluation |
| Peritoneal factors | Laparoscopy |
- Textbook of Family Medicine 9e, Table 35-19; Tietz Lab Medicine
Key cut-offs:
- Serum progesterone >300 ng/dL (9.5 nmol/L) in midluteal phase = ovulation confirmed
- Day 3 FSH >12 IU/L = diminished ovarian reserve; refer to reproductive endocrinologist
- Tietz Lab Medicine, p.2826; Textbook of Family Medicine 9e, p.1389
Note: basal body temperature charts, postcoital tests, and endometrial biopsies are no longer recommended as routine studies in initial evaluation. - Textbook of Family Medicine 9e, p.1406
PART VIII: TREATMENT OF FEMALE INFERTILITY
Treatment is directed toward the underlying cause:
| Cause | Treatment |
|---|
| PCOS / anovulation | Clomiphene citrate (first-line); letrozole (aromatase inhibitor, now preferred for PCOS); metformin (for insulin resistance); gonadotropin injections |
| Hyperprolactinemia | Bromocriptine or cabergoline (dopamine agonists) |
| Hypothalamic hypogonadism | Pulsatile GnRH; exogenous FSH + LH (hMG) |
| Adrenal hyperplasia | Clomiphene + glucocorticoids |
| Tubal occlusion | Tubal surgery; IVF (preferred if severe damage) |
| Endometriosis | Surgical (laparoscopic excision); IVF/ICSI for severe disease |
| Asherman syndrome | Hysteroscopic adhesiolysis |
| Uterine fibroids | Myomectomy (submucosal) |
| Diminished ovarian reserve | IVF with stimulation; oocyte donation |
- Textbook of Family Medicine 9e, p.1402
Assisted Reproductive Technology (ART)
IVF (in vitro fertilization) is the cornerstone treatment for many causes of infertility when simpler approaches fail. It involves controlled ovarian stimulation, oocyte retrieval, fertilization in the laboratory, and embryo transfer. Preimplantation genetic testing for aneuploidy (PGT-A) is used with IVF to screen embryos before transfer (
ASRM/SART Practice Guideline, Fertil Steril, 2024, PMID: 38762806). Short- and long-term outcomes of ART have been extensively reviewed (
Graham et al., Dev Med Child Neurol, 2023, PMID: 35851656).
SUMMARY TABLE: Primary vs. Secondary Female Infertility
| Feature | Primary Infertility | Secondary Infertility |
|---|
| Definition | Never conceived | Previously conceived, now unable |
| Congenital causes | More prominent (Turner, Müllerian anomalies) | Less prominent |
| Acquired causes | Less common (but PID/endometriosis relevant) | Dominant (Asherman, PID, post-surgical) |
| Ovarian reserve | Less likely to be a major factor in young women | Age-related decline important |
| Endometriosis | Can cause primary infertility | Can progress and cause secondary infertility |
| Asherman syndrome | Rare (requires prior uterine instrumentation) | Classic cause |
| Key investigations | Same evaluation framework | Same, but with added attention to uterine cavity |
| Prognosis | Depends on underlying cause | Generally better if prior normal pregnancy; depends on cause |
REFERENCES (Key Sources for This Literature Review)
- Costanzo Physiology, 7th Edition (Elsevier, ISBN 9780323793339) - Oogenesis, folliculogenesis, HPO axis, steroid hormones
- Berek & Novak's Gynecology (Lippincott Williams & Wilkins, ISBN 9781496380357) - Comprehensive menstrual cycle physiology, neuroendocrinology
- Tietz Textbook of Laboratory Medicine, 7th Edition (Elsevier, ISBN 9780323775724) - Normal menstrual cycle, hormonal variations, female infertility evaluation
- Textbook of Family Medicine, 9th Edition (Elsevier, ISBN 9780323239905) - Clinical management of female infertility, PCOS
- Joham AE, Norman RJ, Stener-Victorin E et al. Polycystic ovary syndrome. Lancet Diabetes Endocrinol. 2022;10(9):668-680. [PMID 35934017]
- Stener-Victorin E, Teede H, Norman RJ et al. Polycystic ovary syndrome. Nat Rev Dis Primers. 2024;10(1):27. [PMID 38637590]
- Bonavina G, Taylor HS. Endometriosis-associated infertility: From pathophysiology to tailored treatment. Front Endocrinol. 2022;13:1085348. [PMID 36387918]
- Lamceva J, Uljanovs R, Strumfa I. The Main Theories on the Pathogenesis of Endometriosis. Int J Mol Sci. 2023;24(4):4254. [PMID 36901685]
- Elizur SE, Mostafa J, Berkowitz E. Endometriosis and infertility: pathophysiology, treatment strategies, and reproductive outcomes. Arch Gynecol Obstet. 2025;312:1501-1515. [PMID 40689964]
- Horner PJ et al. What Can Serology Tell Us About the Burden of Infertility in Women Caused by Chlamydia? J Infect Dis. 2021. [PMID 34396401]
- ASRM/SART Practice Committees. Preimplantation genetic testing for aneuploidy: a committee opinion. Fertil Steril. 2024. [PMID 38762806]
- Graham ME, Jelin A, Hoon AH Jr. Assisted reproductive technology: Short- and long-term outcomes. Dev Med Child Neurol. 2023;65(1):46-53. [PMID 35851656]
This literature review synthesizes content from authoritative medical textbooks and current peer-reviewed literature. For thesis citation purposes, always verify page numbers in your specific edition and follow your institution's citation style (APA, Vancouver, Harvard). The framework above covers all key domains - physiology, menstrual cycle physiology and pathology, general infertility epidemiology, and primary versus secondary female infertility - at the depth appropriate for a thesis literature review chapter.