Astrology and pathology of chronic pyelonephritis
Reading File
Finding Sources
Finding Sources
Searching PubMed
chronic pyelonephritis pathology
Reading File
Reading File
Reading File
Reading File
Searching Images
chronic pyelonephritis histology gross pathology
Loading Image
Searching Images
chronic pyelonephritis kidney thyroidization tubules histology
Loading Image
Loading Image
I have all the material needed for a comprehensive answer. Note: the user likely meant etiology (not "astrology") — a common typo/autocorrect. I'll address both etiology and pathology.
Etiology and Pathology of Chronic Pyelonephritis
Note: I'm interpreting "astrology" as "etiology" — the standard pairing with pathology in clinical medicine.
Definition
Chronic pyelonephritis is a clinicopathologic entity in which chronic tubulointerstitial inflammation and scarring involve the renal parenchyma along with deformity of the pelvicalyceal system, distinguishing it from other causes of chronic interstitial nephritis. Critically, it affects the calyces — a feature shared only with analgesic nephropathy, making pelvocalyceal damage a key diagnostic clue.
- Robbins & Kumar Basic Pathology, p. 548
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Etiology (Causes and Predisposing Factors)
Chronic pyelonephritis virtually never occurs in a structurally normal urinary tract. It almost always requires a predisposing anatomical or functional abnormality:
1. Vesicoureteral Reflux (VUR) — Most Common Cause
- Reflux-associated (reflux) nephropathy is the most common cause of chronic pyelonephritis.
- VUR allows bacteria to ascend to the renal pelvis and parenchyma.
- Intrarenal reflux (compound papillae at the poles) explains why scars are characteristically polar (upper and lower poles).
- Children with severe VUR are at highest risk; improving recognition and early treatment of VUR has reduced the incidence of end-stage renal disease (ESRD) from this cause.
2. Urinary Tract Obstruction
- Calculi, posterior urethral valves, ureteral strictures, prostatic hypertrophy, or pelvic masses.
- Obstruction can be unilateral (calculi, ureteral lesions) or bilateral (congenital urethral anomalies).
- Stasis promotes bacterial colonization and recurrent infection.
3. Recurrent Urinary Tract Infections (UTIs)
- Repeated episodes of ascending bacterial infection → repeated bouts of renal inflammation → progressive scarring.
- Common organisms: E. coli, Proteus, Klebsiella, Enterococcus.
- Uncomplicated UTI alone in a structurally normal tract is rarely (if ever) sufficient to cause chronic pyelonephritis or ESRD in adults.
4. Other Predisposing Conditions
| Condition | Mechanism |
|---|---|
| Nephrolithiasis | Obstruction + nidus for recurrent infection |
| Neurogenic bladder | Urinary stasis, incomplete emptying |
| Pregnancy | Ureteral dilation + immunosuppression |
| Diabetes mellitus | Impaired host defenses, papillary necrosis risk |
| Immunosuppression | Reduced ability to clear infection |
| Analgesic abuse | Papillary necrosis → structural damage |
Campbell-Walsh-Wein Urology: "In patients without underlying renal or urinary tract disease, chronic pyelonephritis secondary to UTI is a rare disease… Nonobstructive uncomplicated UTI alone was never found to be the cause of renal insufficiency."
Pathology
Gross Morphology
The hallmarks on gross examination are:
- Coarse, discrete, irregular corticomedullary scars overlying dilated, blunted, or deformed calyces
- Flattening of the papillae
- Kidneys are asymmetrically scarred (bilaterality is possible but asymmetric) — this distinguishes it from chronic glomerulonephritis, where both kidneys are diffusely and symmetrically scarred
- Scars are most numerous at the upper and lower poles, corresponding to reflux sites (compound papillae)
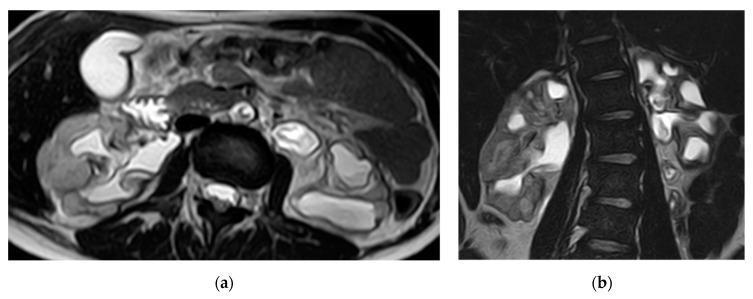
- Affected kidneys appear irregularly contracted on imaging
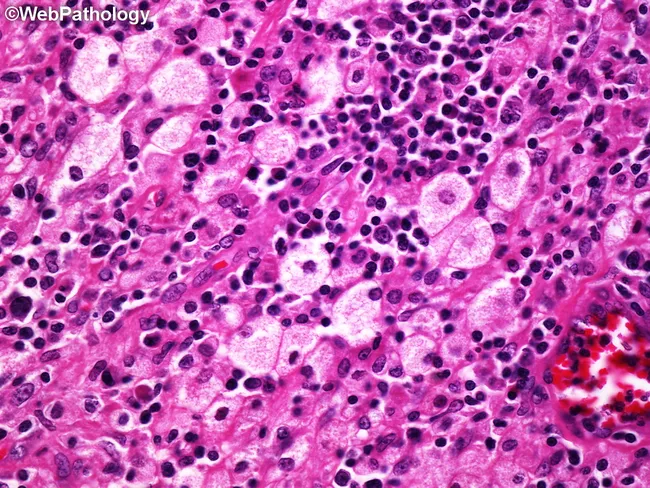
Microscopic Morphology
Changes are predominantly tubulointerstitial:
| Structure | Changes |
|---|---|
| Tubules | Atrophy in some areas; hypertrophy/dilation in others |
| "Thyroidization" | Dilated tubules with flattened epithelium filled with proteinaceous (PAS-positive) casts resembling thyroid colloid — a hallmark but not specific feature |
| Interstitium | Fibrosis + chronic inflammatory infiltrate (lymphocytes, plasma cells, occasional neutrophils) in cortex and medulla |
| Calyces | Fibrosis around calyceal epithelium + marked chronic inflammatory infiltrate |
| Glomeruli | Generally normal early; later show periglomerular fibrosis, fibrous obliteration, ischemic changes; secondary FSGS in advanced disease |
Special Form: Xanthogranulomatous Pyelonephritis (XGP)
A rare variant of chronic pyelonephritis characterized by:
- Accumulation of foamy (lipid-laden) macrophages intermingled with plasma cells, lymphocytes, PMNs, and occasional giant cells
- Associated with Proteus infections and obstruction/nephrolithiasis
- Large yellow-orange nodules that can grossly mimic renal cell carcinoma
- Requires nephrectomy in most cases
Other Infection-Related Variants
- Malakoplakia: Macrophage dysfunction with intracytoplasmic calcifications (Michaelis-Gutmann bodies)
- Megalocytic interstitial nephritis: PAS-positive granular macrophage cytoplasm
- All three associated with gram-negative infections and macrophage dysfunction
Pathogenesis Summary
Predisposing factor (VUR / obstruction / stones)
↓
Recurrent ascending bacterial infection
↓
Acute inflammatory bouts → tubular injury
↓
Interstitial fibrosis + tubular atrophy
↓
Calyceal deformity + corticomedullary scarring
↓
Loss of concentrating ability → polyuria, nocturia
↓
Secondary FSGS (in some) → proteinuria → CKD → ESRD
Clinical Correlation
| Feature | Detail |
|---|---|
| Onset | Often silent; late presentation with renal insufficiency or hypertension |
| Urine | Bacteriuria/pyuria may be present or absent (especially if obstructed or late-stage) |
| Imaging | Asymmetric contracted kidneys, cortical scars, calyceal clubbing/deformity |
| Tubular dysfunction | Loss of concentrating ability → polyuria, nocturia (hyposthenuria) |
| Proteinuria | Usually mild; development of heavy proteinuria/secondary FSGS is a poor prognostic sign |
| ESRD | Risk significantly higher when underlying VUR, obstruction, or reflux nephropathy present |
Robbins, Cotran & Kumar Pathologic Basis of Disease: "The onset of proteinuria is a poor prognostic sign since it indicates an increased likelihood of progression to ESRD."
Sources: Robbins, Cotran & Kumar — Pathologic Basis of Disease; Robbins & Kumar — Basic Pathology; Campbell-Walsh-Wein Urology; National Kidney Foundation — Primer on Kidney Diseases, 8e
This is a shared conversation. Sign in to Orris to start your own chat.