Inguinal canal anatomy with tricks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Now I have everything needed for a comprehensive, trick-rich answer. Let me compile it:
Inguinal Canal Anatomy - Complete Guide with Mnemonics & Tricks
Basic Facts
- An oblique, slit-like passage in the lower anterior abdominal wall
- ~4 cm long (some sources say 4-6 cm)
- Runs downward, forward, and medially, parallel to and just above the inguinal ligament
- Goes from the deep (internal) inguinal ring → superficial (external) inguinal ring
The Two Rings
Deep (Internal) Inguinal Ring
- Opening in the transversalis fascia (actually the beginning of its tubular evagination, forming the internal spermatic fascia)
- Location: midpoint of the inguinal ligament - midway between the ASIS and the pubic symphysis (not pubic tubercle - common exam trick!)
- The inferior epigastric vessels lie just medial to it - this is the key landmark separating indirect from direct hernias
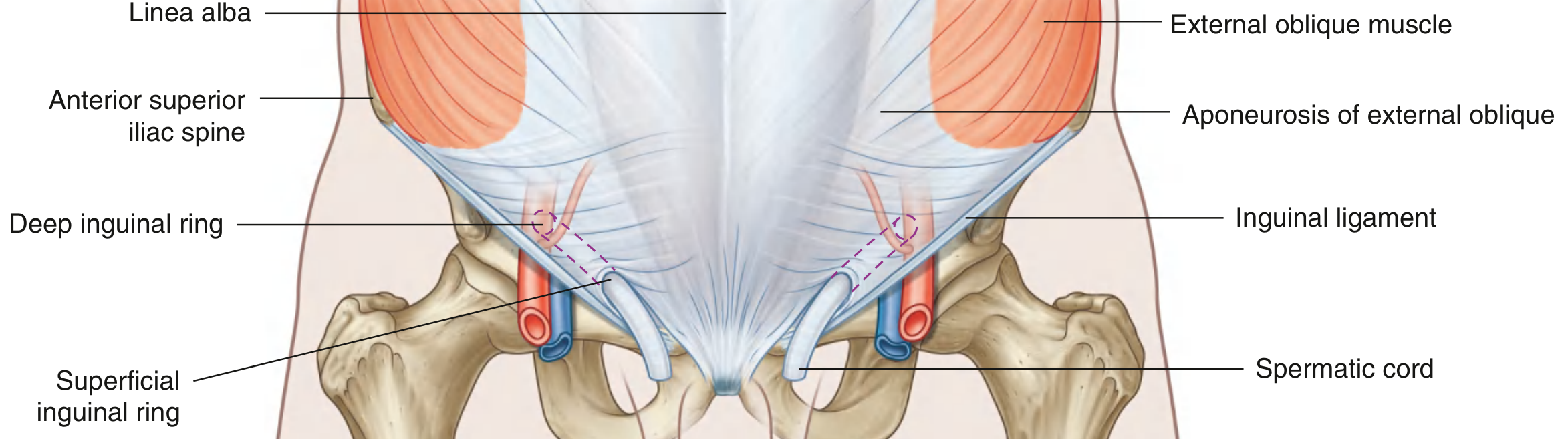
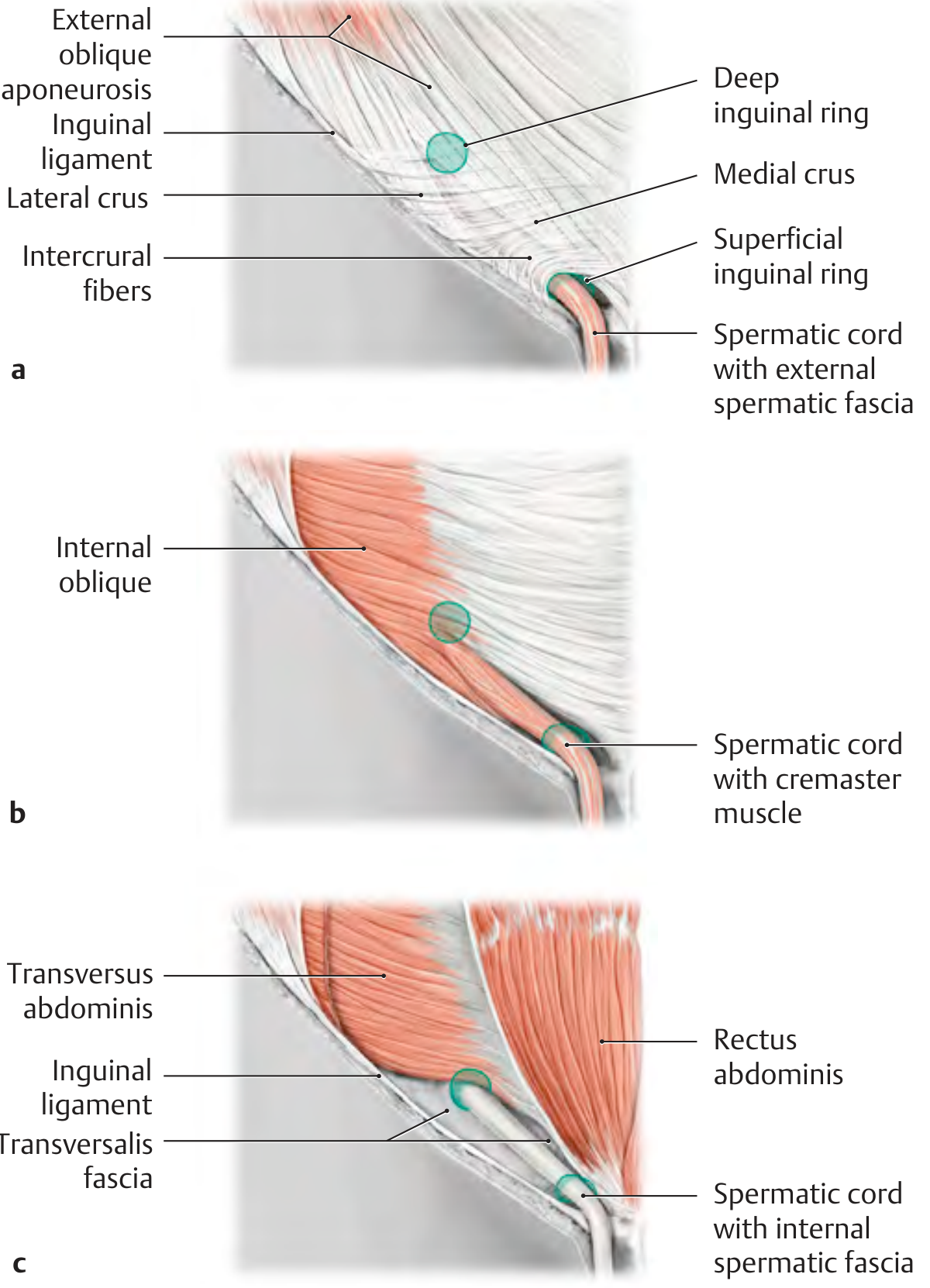
Superficial (External) Inguinal Ring
- Triangular opening in the external oblique aponeurosis
- Located just superolateral to the pubic tubercle
- Apex points superolaterally; base = pubic crest
- Medial crus attaches to pubic symphysis, lateral crus to pubic tubercle
- Intercrural fibers prevent further widening
Trick: "Deep = Defect in transversalis fascia. Superficial = Slit in external oblique aponeurosis."
The Four Walls - "MALT" Mnemonic
| Wall | Structure | Trick |
|---|---|---|
| Medial (posterior) | Transversalis fascia + peritoneum (with interfoveolar ligament medially) | "Trans-post" |
| Anterior | External oblique aponeurosis (+ internal oblique in lateral 1/3) | "External = Anterior" |
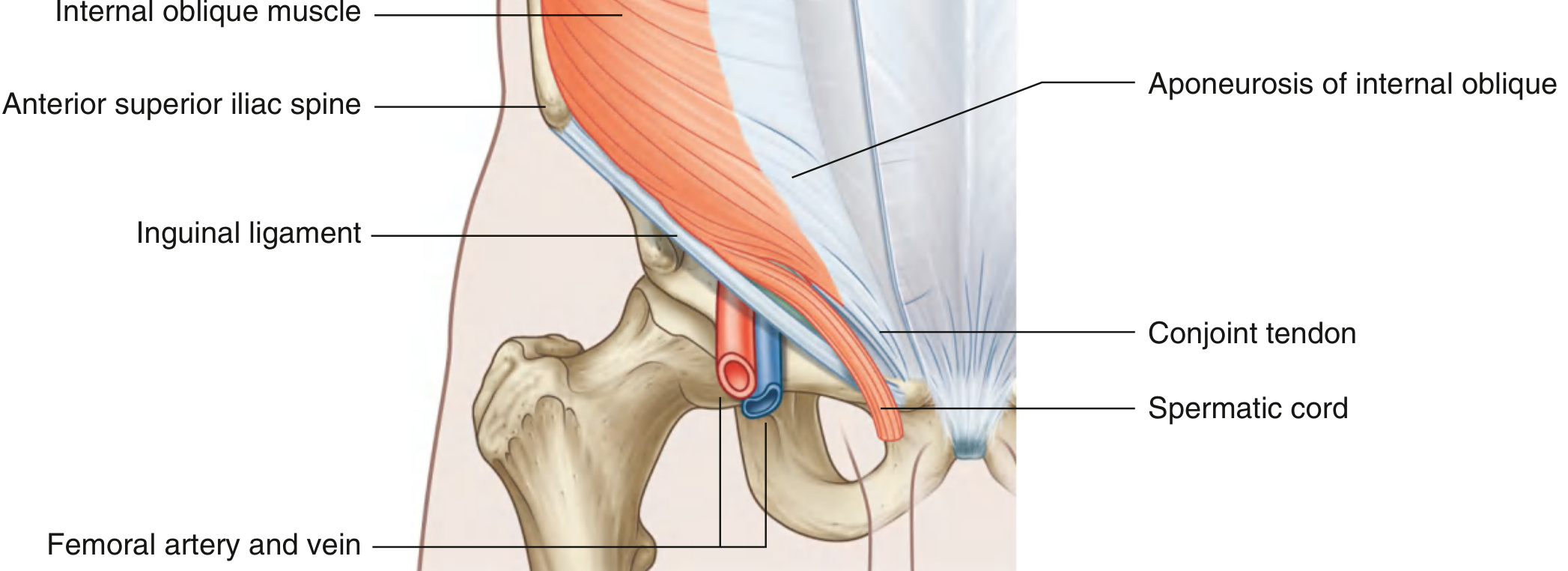
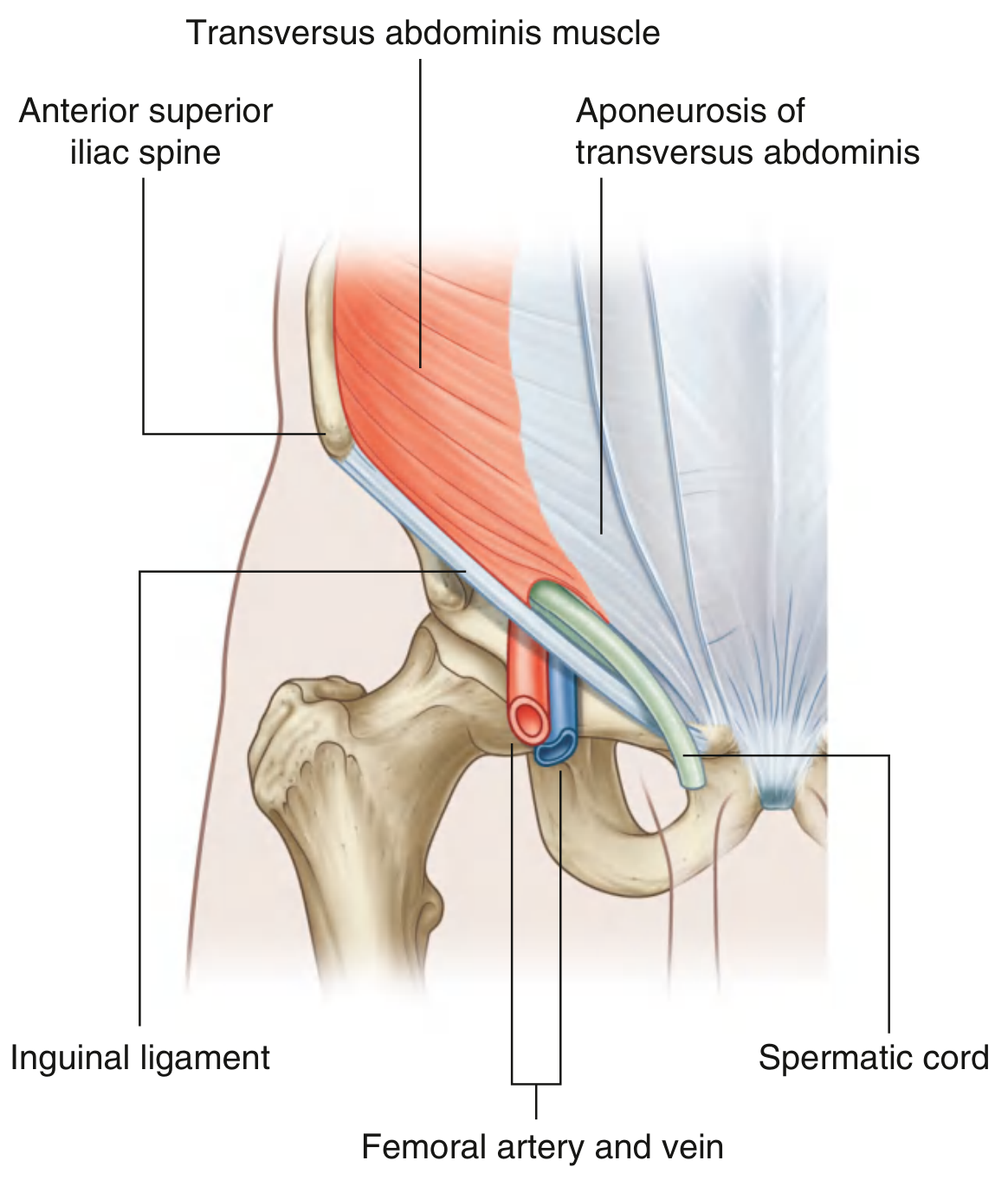
| Lateral/Roof | Arching fibers of internal oblique + transversus abdominis → conjoint tendon | "Roof arches over" |
| Trench/Floor | Medial half of the inguinal ligament (+ lacunar ligament medially) | "Floor = Poupart's gutter" |
Better Mnemonic for walls: "2 Muscles Arch Over (MALT)"
- M = Medial posterior wall = transversalis fascia
- A = Anterior wall = external oblique aponeurosis
- L = Lateral/Superior (Roof) = internal oblique + transversus
- T = Trough/Floor = inguinal ligament
Trick to remember the roof: The internal oblique and transversus abdominis arc over the deep ring laterally and descend medially to fuse as the conjoint tendon (falx inguinalis) - the roof descends to become the posterior wall medially. This is the anatomical basis of the "shutter mechanism" that closes the canal with increased abdominal pressure.
Contents - by Sex
In Males (the Spermatic Cord + extras):
The spermatic cord contains:
- Vas deferens (ductus deferens)
- Testicular artery (from aorta at L2)
- Pampiniform plexus of veins
- Cremasteric artery (from inferior epigastric)
- Artery to vas (from inferior vesical)
- Sympathetic nerve fibers + lymphatics
- 3 fascial coverings: internal spermatic fascia, cremasteric fascia, external spermatic fascia
Trick for spermatic cord coverings: "I Carry Everything" - Internal spermatic fascia (from transversalis fascia), Cremasteric fascia (from internal oblique), External spermatic fascia (from external oblique aponeurosis)
In Females:
- Round ligament of the uterus + its artery
- Genital branch of genitofemoral nerve
In BOTH Sexes:
- Ilioinguinal nerve (L1) - enters canal by piercing the internal oblique; exits through superficial ring; supplies scrotum/labia majora and medial thigh
- Lymphatics
Trick: "Ilioinguinal does NOT enter the deep ring" - it pierces internal oblique from behind and joins the canal partway through, then exits the superficial ring.
Key Nerve Relations
| Nerve | Path | Clinical Relevance |
|---|---|---|
| Ilioinguinal (L1) | Pierces internal oblique → travels in canal on top of spermatic cord → exits superficial ring | Injured in hernia repair - numbness of scrotum/labia & medial thigh |
| Iliohypogastric (L1) | Runs above the canal, pierces external oblique above superficial ring | Damaged in Pfannenstiel incision |
| Genital branch of genitofemoral (L1/L2) | Enters deep ring with spermatic cord; motor to cremaster, sensory to scrotum | Cremasteric reflex |
Hesselbach's Triangle (Site of Direct Hernias)
Three boundaries - "RIP" mnemonic:
- Rectus abdominis - medially
- Inferior epigastric vessels - laterally
- Poupart's ligament (inguinal ligament) - inferiorly

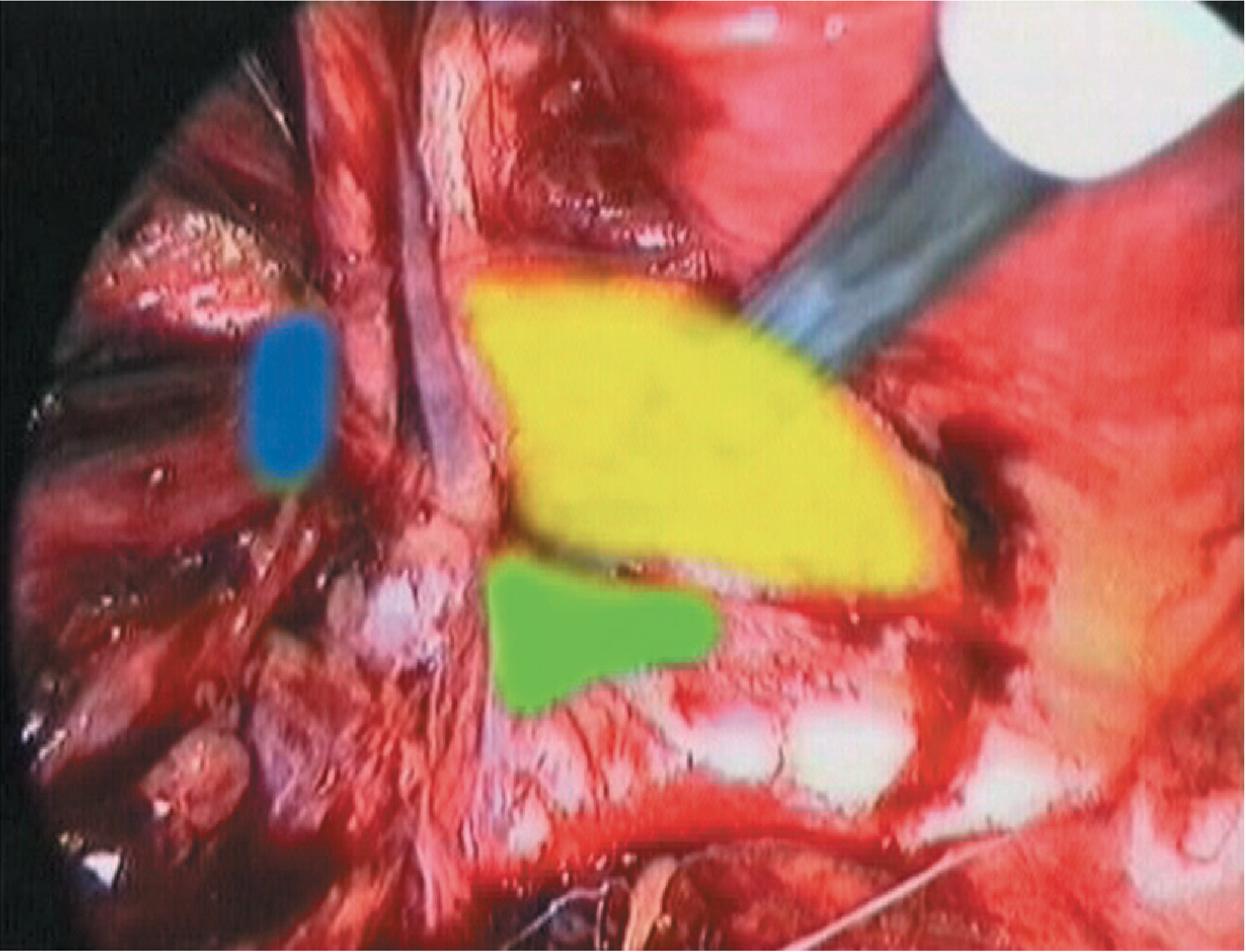
Indirect vs. Direct Hernia - The Key Distinction
| Feature | Indirect | Direct |
|---|---|---|
| Entry point | Deep (internal) ring - LATERAL to inferior epigastric vessels | Posterior wall (Hesselbach's triangle) - MEDIAL to inferior epigastric vessels |
| Mechanism | Congenital (patent processus vaginalis) or acquired | Always acquired - weakness of transversalis fascia |
| Can enter scrotum? | Yes - follows processus vaginalis | Rarely (does not traverse full canal) |
| Age | More common in young | More common in older men |
| Control with finger at deep ring | Controlled | Not controlled |
| Relationship to inferior epigastric | Lateral | Medial |
Classic trick: "Indirect = In through the deep ring = lateral = young = congenital possible. Direct = Directly through the wall = medial = old man."
The Shutter Mechanism (Functional Anatomy Trick)
When intra-abdominal pressure rises (coughing, straining):
- Internal oblique and transversus abdominis contract
- Their arching fibers descend toward the inguinal ligament (the roof comes down)
- This compresses the canal like a shutter, preventing herniation
- In females: more protective because the round ligament is smaller, keeping the rings tighter
- In males: this is why large direct hernias are predominantly male - once the shutter mechanism fails, there is no muscle protection medially
Processus Vaginalis - The Embryological Basis
- Peritoneal diverticulum that precedes testicular descent
- Testis descends retroperitoneally → through deep ring → canal → superficial ring → scrotum
- Normally obliterates after birth
- Persistence → indirect inguinal hernia (congenital) in males
- Partial persistence → hydrocele (communicating or non-communicating)
Summary Table of Walls (Quick Reference)
| Structure | |
|---|---|
| Anterior wall | External oblique aponeurosis |
| Posterior wall | Transversalis fascia (+ peritoneum) |
| Roof (superior wall) | Internal oblique + Transversus abdominis → conjoint tendon |
| Floor (inferior wall) | Medial inguinal ligament (+ lacunar ligament medially) |
| Deep ring | Transversalis fascia (midpoint of inguinal ligament; lateral to inferior epigastric vessels) |
| Superficial ring | External oblique aponeurosis (superolateral to pubic tubercle) |
Exam Tricks Summary
- Deep ring location: Midway between ASIS and pubic symphysis (not tubercle). Inferior epigastric vessels lie just medial to it.
- Indirect hernia = LATERAL to inferior epigastrics; Direct = MEDIAL (through Hesselbach's triangle).
- Ilioinguinal nerve does NOT enter the deep ring - it joins the canal partway by piercing internal oblique.
- Genital branch of genitofemoral enters the deep ring (not the ilioinguinal).
- Conjoint tendon = fused aponeurosis of internal oblique + transversus abdominis → attaches to pubic tubercle and pectineal line → forms the roof AND reinforces the posterior wall medially.
- Coverings of spermatic cord = from inner to outer: Internal spermatic fascia (transversalis) → Cremasteric fascia (internal oblique) → External spermatic fascia (external oblique).
- Females have the inguinal canal but smaller rings; genital branch of genitofemoral nerve is in the canal (not the round ligament alone).
- Direct hernias cannot reach the scrotum in the classical sense - they bulge through the posterior wall but do not follow the oblique canal course.
Sources: Gray's Anatomy for Students, p. 352-354; Bailey and Love's Short Practice of Surgery 28th Ed., p. 1087; Thieme Atlas of General Anatomy and Musculoskeletal System, p. 231
Boundaries in details
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Now I have everything for a deep-dive into the boundaries. Here it is:
Inguinal Canal - Boundaries in Detail
The Six Boundaries at a Glance
| Boundary | Primary Structure | Reinforcement |
|---|---|---|
| Anterior wall | External oblique aponeurosis (entire length) | Internal oblique muscle fibers (lateral 1/3 only) |
| Posterior wall | Transversalis fascia (entire length) | Conjoint tendon (medial 1/3 only) |
| Roof (superior wall) | Arching fibers of internal oblique + transversus abdominis | Fuse medially as the conjoint tendon |
| Floor (inferior wall) | Medial half of inguinal ligament | Lacunar ligament (medial part) |
| Deep (internal) ring | Transversalis fascia | - |
| Superficial (external) ring | External oblique aponeurosis | Intercrural fibers |
1. Anterior Wall
Primary structure: Aponeurosis of the external oblique - present along the entire length of the canal.
Reinforcement - lateral 1/3 only: The lowermost fibers of the internal oblique muscle (which originate from the lateral 2/3 of the inguinal ligament) arch over and cover the deep inguinal ring from the front. This is important because the deep ring is a potential weak point - nature adds a muscular lid on top of it.
Trick: "The anterior wall is the wall you cut through first in open hernia repair - you open the external oblique aponeurosis to enter the canal."
Trick for the reinforcement: The internal oblique covers the deep ring anteriorly (outer side), but as the spermatic cord passes through it becomes the cremasteric fascia - so the same muscle that reinforces the anterior wall contributes the middle covering of the cord.
2. Posterior Wall
Primary structure: Transversalis fascia - present along the entire length of the canal.
Reinforcement - medial 1/3 only: The conjoint tendon (inguinal falx) - formed by the fused aponeuroses of the internal oblique + transversus abdominis - inserts onto the pubic crest and pectineal line, reinforcing the posterior wall behind the superficial inguinal ring.
- The conjoint tendon sits posterior to the superficial ring, plugging the weakest medial spot
- The interfoveolar ligament (a thickening of the transversalis fascia between the two epigastric folds) contributes additional reinforcement at the mid-posterior wall
Trick for what's lateral vs. medial in the posterior wall:
- Lateral 2/3 = naked transversalis fascia only (the weak zone where indirect hernias push through)
- Medial 1/3 = transversalis fascia + conjoint tendon (reinforced, but direct hernias can still break through if weakened)
Surgical trick: In the Bassini repair, the surgeon sutures the conjoint tendon to the inguinal ligament to reinforce this posterior wall. In Lichtenstein, a mesh is placed in the preperitoneal space to reinforce it.
3. Roof (Superior Wall)
Structure: The arching fibers of the internal oblique and transversus abdominis muscles together.
- These muscles originate laterally from the inguinal ligament (and iliac crest)
- Their lower fibers arch over the spermatic cord from lateral to medial
- They fuse medially to form the conjoint tendon attaching to the pubic crest
The Shutter Mechanism: When intra-abdominal pressure rises, these muscles contract and their arching fibers descend toward the inguinal ligament (floor) - the roof comes down to meet the floor, compressing and closing the canal like a shutter valve. This is the primary defense against herniation.
Trick: "The roof and the posterior wall medially are both made by the same two muscles (IO + TA) - they arch over as the roof, then fuse and come down to reinforce the posterior wall as the conjoint tendon."
4. Floor (Inferior Wall)
Primary structure: The medial half of the inguinal ligament - this is the infolded lower free edge of the external oblique aponeurosis. It rolls inward and upward to form a concave gutter or trough on which the spermatic cord rests.
Medial reinforcement: The lacunar ligament (Gimbernat's ligament) - where the inguinal ligament turns posteriorly to attach to the pectineal line of the pubis. It fans out medially to fill the angle between the inguinal ligament and the pectineal line.
Deep (lateral) contribution: The iliopubic tract (a thickening of the transversalis fascia running parallel to and just deep to the inguinal ligament) reinforces the deep/lateral portion of the floor. This is the landmark used in laparoscopic hernia repair.
Three-zone floor breakdown from lateral to medial:
- Lateral - iliopubic tract (transversalis fascia thickening)
- Central - superior gutter surface of inguinal ligament
- Medial - lacunar ligament (Gimbernat's ligament)
Trick: The lacunar ligament is the rigid medial edge of the floor - this is why it is the tight structure that strangulates a femoral hernia (it cannot expand).
5. Deep (Internal) Inguinal Ring
Structure: An outpouching/evagination of the transversalis fascia - not merely a hole, but the start of a fascial tube that becomes the internal spermatic fascia around the cord.
Exact location:
- Midway between the ASIS and pubic symphysis (not the pubic tubercle)
- Just above the inguinal ligament
- Lateral to the inferior epigastric vessels (this is the key surgical landmark)
- 4 cm lateral to the superficial ring
Boundaries of the ring itself:
- Medially: the interfoveolar ligament (a fold of transversalis fascia containing the inferior epigastric vessels - the "lateral umbilical fold")
- Inferiorly: inguinal ligament
- Laterally: the transversalis fascia itself
Trick: "Inferior epigastric vessels are the gatekeepers - lateral to them = deep ring = indirect. Medial to them = Hesselbach's = direct."
6. Superficial (External) Inguinal Ring
Structure: A triangular defect in the aponeurosis of the external oblique muscle.
Boundaries of the triangle:
- Apex: points superolaterally; held together by intercrural fibers that bridge the two crura, preventing further widening
- Base: the pubic crest
- Medial crus: attached to the pubic symphysis
- Lateral crus: attached to the pubic tubercle
- Reflected inguinal ligament (Colles' ligament): arched fibers from the contralateral external oblique aponeurosis that reflect upward to complete the deep groove at the ring's base
Location: Just superolateral to the pubic tubercle (this helps distinguish inguinal hernia from femoral hernia, which lies inferomedial to the pubic tubercle)
Clinical trick - inguinal vs. femoral hernia by ring position:
- Inguinal hernia sac → exits above and medial to pubic tubercle
- Femoral hernia sac → exits below and lateral to pubic tubercle
The "Boundary-Asymmetry" Concept - High-Yield
The canal does NOT have uniform walls throughout its length. Each wall has a lateral and medial character:
| Wall | Lateral portion | Medial portion |
|---|---|---|
| Anterior | External oblique + internal oblique (double layer) | External oblique only |
| Posterior | Transversalis fascia only (weakest zone) | Transversalis fascia + conjoint tendon |
| Floor | Inguinal ligament + iliopubic tract | Inguinal ligament + lacunar ligament |
| Roof | Arching IO + TA muscle fibers (active, shutter) | Conjoint tendon (static reinforcement) |
Big-picture trick: Nature designed this so that lateral weakness (where the deep ring is) is defended by the anterior wall (internal oblique over the deep ring), while medial weakness (where direct hernias occur) is defended by the posterior wall (conjoint tendon). The two reinforcements are placed exactly opposite to each other, cross-protecting the canal.
Ligaments of the Floor - Often Confused
| Ligament | Also known as | What it is | Attaches |
|---|---|---|---|
| Inguinal ligament | Poupart's ligament | Folded inferior edge of external oblique aponeurosis | ASIS → pubic tubercle |
| Lacunar ligament | Gimbernat's ligament | Medial extension of inguinal ligament turning back on itself | Pubic tubercle → pectineal line |
| Pectineal ligament | Cooper's ligament | Periosteum + fascia of pectineal line | Along pectineal line of pubis |
| Iliopubic tract | - | Deep thickening of transversalis fascia parallel to inguinal ligament | ASIS → superior pubic ramus |
| Reflected inguinal ligament | Colles' ligament | Fibers from contralateral external oblique that reflect upward | Pubic symphysis → linea alba |
Exam trick: Cooper's ligament (pectineal ligament) is used as the suture anchor in the McVay repair of inguinal and femoral hernias because it is the strongest structure in the area.
Sources: Gray's Anatomy for Students, pp. 352-354; Campbell Walsh Wein Urology, p. 3230-3231; Bailey and Love's Short Practice of Surgery 28th Ed., p. 1087; Thieme Atlas of General Anatomy and Musculoskeletal System, p. 231-237
This is a shared conversation. Sign in to Orris to start your own chat.