Thermoregulation and its importance in anaesthesia
Reading File
Finding Sources
Finding Sources
Searching PubMed
thermoregulation anesthesia perioperative hypothermia
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have all the information needed to write a comprehensive, well-structured answer. Let me compose it.
Thermoregulation and Its Importance in Anaesthesia
1. Normal Thermoregulation
The hypothalamus maintains core body temperature within very narrow tolerances, known as the interthreshold range. At one extreme sits the threshold for sweating and vasodilation (heat loss); at the other, the threshold for vasoconstriction and shivering (heat conservation). In healthy, awake individuals, a fraction of a degree change in core temperature is enough to trigger the appropriate response - the interthreshold range is approximately 0.2-0.4°C. Core temperature is normally 36.5-37.5°C, and is best measured by central venous blood temperature, with oesophageal, nasopharyngeal, tympanic membrane, or bladder probes serving as proxies.
Heat is generated via basal metabolic activity and muscle contraction (including shivering), and is lost through four physical mechanisms:
- Radiation (~60% of heat loss at rest) - electromagnetic emission from skin
- Convection - heat transfer to air currents
- Conduction - direct transfer to surfaces
- Evaporation - from skin and respiratory tract
2. How Anaesthesia Disrupts Thermoregulation
Both general and neuraxial anaesthetics impair thermoregulation by interfering with hypothalamic reflex responses.
General anaesthesia:
- Widens the interthreshold range (from ~0.4°C to ~4°C), meaning the body tolerates a much larger temperature swing before activating a defence response.
- Isoflurane produces a concentration-dependent decrease in the vasoconstriction threshold (~3°C decrease per 1% inhaled isoflurane).
- Shivering, the most powerful heat-generation defence, is also suppressed.
Neuraxial (spinal/epidural) anaesthesia:
- Causes vasodilation below the block level, redistributing heat from warm central compartments to cooler peripheral tissues.
- Impairs the hypothalamus's temperature perception from the anaesthetised dermatomes, leading it to underestimate the degree of heat loss - this ongoing misperception allows continued cooling even as the patient's core temperature falls.
3. The Three Phases of Perioperative Hypothermia
Unintentional perioperative hypothermia is defined as core temperature < 36°C and will occur in nearly every patient undergoing general or regional anaesthesia unless actively prevented. The pattern is characteristic:
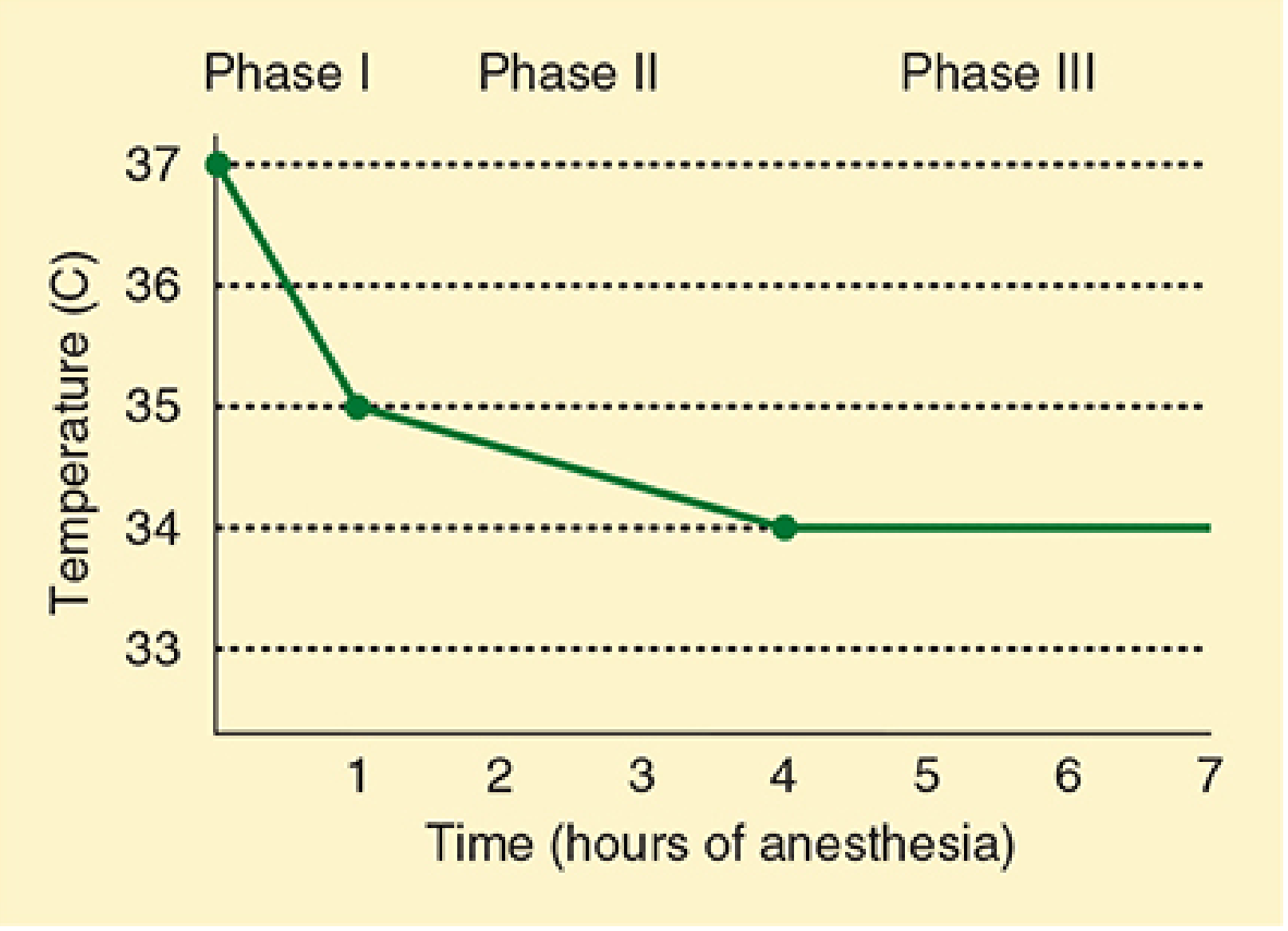
Figure: Core temperature typically falls ~2°C in the first hour (Phase I), then gradually over 3-4 hours (Phase II), before plateauing (Phase III). - Morgan & Mikhail's Clinical Anesthesiology, 7e
| Phase | Mechanism | Time course |
|---|---|---|
| Phase I - Redistribution | Heat moves from warm core (abdomen, thorax) to cooler periphery due to anaesthetic-induced vasodilation. Actual heat loss to environment is minimal. | First 1 hour; core drops ~1-2°C |
| Phase II - Continuous heat loss | Ongoing radiation, convection, conduction, and evaporation to the cold OR environment. | Hours 1-4; slow, gradual decline |
| Phase III - Steady state | Heat loss equals metabolic production. | After ~4 hours; temperature plateaus |
- Morgan & Mikhail's Clinical Anesthesiology, 7e, p.2293-2295
4. Deleterious Effects of Hypothermia
Unintended perioperative hypothermia has been associated with increased mortality and multiple adverse physiological consequences:
| System | Effect |
|---|---|
| Cardiac | Arrhythmias, ischaemia, increased peripheral vascular resistance |
| Haematological | Reversible coagulopathy (platelet dysfunction), increased transfusion requirements |
| Respiratory | Reduced oxygen delivery (left-shift of Hb-O2 curve), reduced hypoxic ventilatory drive |
| Metabolic | Delayed drug metabolism, prolonged action of muscle relaxants |
| Neurological | Altered mental status, shivering |
| Renal | Impaired renal function |
| Wound | Peripheral vasoconstriction impairs tissue oxygenation, increased surgical site infection risk, impaired wound healing |
Prevention or correction of hypothermia has been shown to decrease wound infections and increase collagen deposition in major abdominal surgery. - Barash's Clinical Anesthesia, 9e, p.550
5. Postoperative Shivering
Shivering in the PACU can arise from:
- True hypothermia (the body's attempt to restore temperature)
- Neurological after-effects of volatile agents (non-thermoregulatory shivering)
- Post-regional anaesthesia (spinal/epidural anaesthetics lower the shivering threshold)
Consequences of intense shivering:
- Increases oxygen consumption by up to fivefold
- Decreases arterial oxygen saturation
- Increases CO2 production and cardiac output
- Raises myocardial ischaemia risk
- Can occasionally cause rebound hyperthermia (38-39°C) with metabolic acidosis
Treatment:
- Best approach: maintain normothermia intraoperatively so shivering doesn't occur
- IV meperidine (pethidine) 12.5-25 mg in adults is effective pharmacological treatment
- Intubated/ventilated patients: sedation + muscle relaxant while rewarming
6. Prevention and Management of Hypothermia
Pre-operative
- Prewarming for 30 minutes with convective forced-air warming blankets before induction significantly reduces the Phase I redistribution drop by minimising the central-peripheral temperature gradient.
Intraoperative
- Forced-air warming blankets (Bair Hugger) - most effective active warming method
- Warm-water blankets on the operating table
- Heated humidification of inspired gases - reduces evaporative losses from the airway
- Warming of IV fluids - especially when large volumes are used
- Increasing OR ambient temperature - cold theatre temperature is a significant contributor
- Passive insulators (warm cotton blankets, metallic "space blankets") have limited utility unless the entire body is covered
Postoperative
- Forced-air warming device (first-line)
- Warming lights or heating blankets as alternatives
- Treat shivering (see above)
High-risk patients: extremes of age, long procedures, abdominal surgery, cold ambient OR, large-volume IV fluids, high-flow unhumidified gases.
7. Special Populations
Neonates and Infants
Infants are especially vulnerable because of:
- Large surface area : body weight ratio
- Thin skin and limited fat stores
- Dependence on non-shivering thermogenesis (brown fat metabolism) rather than shivering, particularly in the first 3 months of life
Cold stress in neonates causes increased oxygen consumption and metabolic acidosis. Anaesthetics specifically impair non-shivering thermogenesis. Warming measures include warming mattresses, incubators, plastic wraps, warm disinfectant solutions, and humidified gases. Forced hot-air blankets are most effective but overheating is a risk. - Miller's Anesthesia, 10e, p.10560
8. Malignant Hyperthermia (MH)
MH represents the most dangerous temperature emergency in anaesthesia - a pathological, uncontrolled form of hyperthermia rather than a failure of thermoregulation.
Definition: A rare (1:15,000 paediatric; 1:40,000 adult) genetic hypermetabolic muscle disorder triggered by volatile anaesthetic agents or succinylcholine.
Pathophysiology: Uncontrolled release of calcium from the sarcoplasmic reticulum in skeletal muscle -> sustained muscle contraction -> massive ATP consumption -> hypermetabolic state with excessive O2 consumption and CO2 production -> severe lactic acidosis, hyperthermia, and rhabdomyolysis.
Triggering agents:
| Volatile Agents | Depolarising Agent |
|---|---|
| Halothane, isoflurane, sevoflurane, desflurane, enflurane, methoxyflurane, ether | Succinylcholine |
Early signs: Unexplained rise in end-tidal CO2 (most sensitive early indicator - doubling/tripling of EtCO2 is a red flag), tachycardia, muscle rigidity, rising temperature. Core temperature can rise at 1°C every 5 minutes.
Late signs: Mixed metabolic and respiratory acidosis, hyperkalaemia, myoglobinuria (dark urine), DIC, acute kidney injury, cerebral oedema, hepatic failure.
Associated conditions: Central-core disease, multi-minicore myopathy, King-Denborough syndrome; Duchenne muscular dystrophy (controversial).
MH Treatment Protocol (MHAUS Protocol):
- Discontinue volatile agent and succinylcholine immediately; notify surgeon; call for help
- Dantrolene sodium 2.5 mg/kg IV as soon as possible (repeat as needed - blocks Ca²+ release from SR)
- Hyperventilate with 100% oxygen
- Sodium bicarbonate for metabolic acidosis
- Cooling measures - cold IV fluids, cold gastric/bladder lavage, cooling blankets
- Hyperkalaemia - dextrose 25-50g IV + regular insulin 10-20 units IV
- Antiarrhythmic agents if needed (after correcting K+ and pH)
- Monitor: EtCO2, electrolytes, ABG, CK (peaks 12-18h post - MH strongly suspected if CK >20,000 IU/L), myoglobin, core temperature, urine output/colour, coagulation
- MHAUS hotline (USA): 1-800-644-9737 for expert consultation 24/7
Mortality even with prompt treatment: 5-30%. Most deaths arise from delayed or absent dantrolene treatment.
- Morgan & Mikhail's Clinical Anesthesiology, 7e, p.2297-2301
9. Intentional Hypothermia / Temperature Management
Hypothermia (in the absence of shivering) reduces metabolic oxygen requirements and can be protective during cerebral or cardiac ischaemia. Targeted temperature management (TTM) is used:
- Cardiac surgery requiring cardiopulmonary bypass - deliberate cooling protects the brain and heart
- Post-cardiac arrest neuroprotection (targeted at 33-36°C per current guidelines)
- Neurosurgery for aneurysm clipping - moderate hypothermia may reduce ischaemic brain injury
10. Key Clinical Pearls
- Nearly all anaesthetised patients will become hypothermic without active warming.
- Prewarming before induction is the most effective single intervention against Phase I redistribution.
- Neuraxial anaesthesia causes hypothermia by the same redistribution mechanism as GA, compounded by impaired hypothalamic perception.
- Any unexplained rise in EtCO2 intraoperatively must raise suspicion for MH.
- Postoperative shivering multiplies O2 consumption fivefold - this is poorly tolerated by patients with cardiac or pulmonary disease.
- Prolonged hypothermia extends neuromuscular blockade and can lead to inadvertent re-curarisation after extubation.
Sources:
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Chapters 13 & 52
- Miller's Anesthesia, 10e - Chapter 72 (Paediatric section)
- Barash's Clinical Anesthesia, 9e - Chapter 82 (Wound healing/SSI)
- Sabiston Textbook of Surgery, p.1204
This is a shared conversation. Sign in to Orris to start your own chat.