Explain the chemotherapy
Reading File
Finding Sources
Searching the Web
chemotherapy mechanisms classes drugs cancer treatment overview
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive explanation of chemotherapy, drawn from authoritative medical textbooks.
Chemotherapy
Definition
Chemotherapy refers to drugs or medicines used to treat cancer. They may be given alone or in combination. Traditional (cytotoxic) chemotherapy targets different phases of the cell cycle and can damage normal cells as well as cancer cells.
- Sabiston Textbook of Surgery, p. 179
Core Principle: Why Cancer Cells Are Targeted
All chemotherapeutic agents exploit the fact that cancer cells divide more rapidly than most normal cells. Because they target rapidly dividing cells preferentially, normal fast-dividing tissues (bone marrow, GI mucosa, hair follicles, oral mucosa) are also susceptible - which accounts for most side effects.
- Swanson's Family Medicine Review
Indications and Contexts of Use
| Term | Meaning |
|---|---|
| Primary/definitive | When cancer is disseminated and not amenable to surgery |
| Adjuvant | After surgery/radiation, to eliminate micrometastases |
| Neoadjuvant | Before surgery, to shrink the tumor |
| Maintenance | Low-dose, to prolong remission |
- Lippincott Illustrated Reviews: Pharmacology, p. 1213
Cell Cycle and Drug Specificity
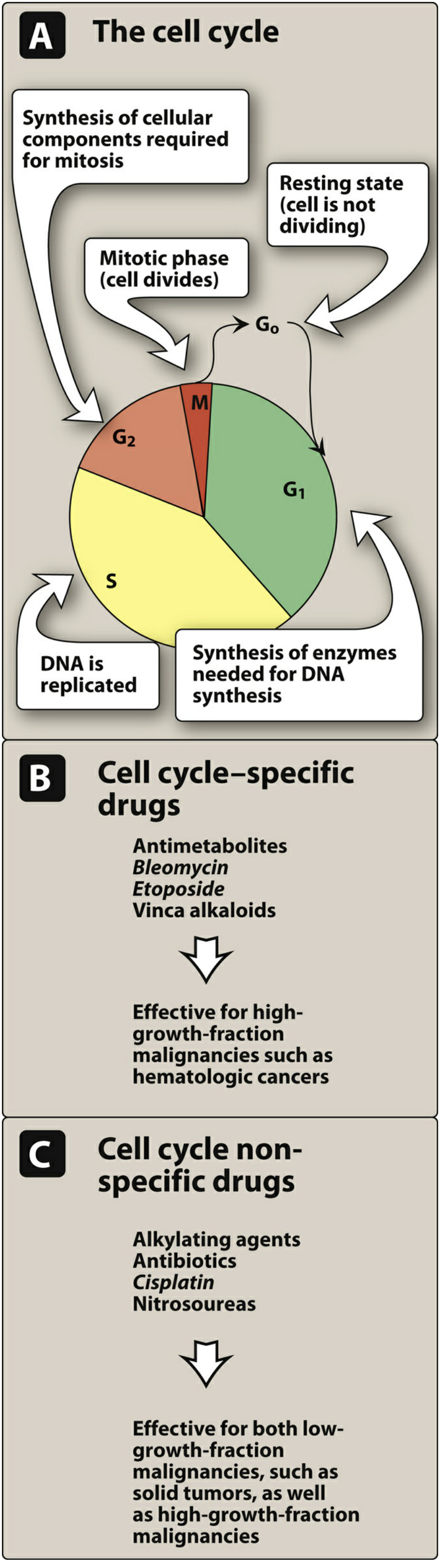
From: Lippincott Illustrated Reviews - Pharmacology
Drugs are divided based on whether they act at a specific cell cycle phase:
- Cell cycle-specific drugs (e.g., antimetabolites, bleomycin, vinca alkaloids): work only on dividing cells; best for high-growth-fraction malignancies like leukemias and lymphomas.
- Cell cycle-nonspecific drugs (e.g., alkylating agents, cisplatin, nitrosoureas): can kill both dividing and resting cells; effective against solid tumors and high-growth-fraction malignancies.
Major Classes of Chemotherapy Drugs
1. Alkylating Agents
- Mechanism: Damage DNA by cross-linking the two DNA strands, preventing the cell from reproducing. They are cell cycle-nonspecific.
- Examples: Cyclophosphamide, ifosfamide, chlorambucil, busulfan, cisplatin, carboplatin.
- Key toxicity: Ifosfamide causes hemorrhagic cystitis (prevented by mesna); cyclophosphamide causes bladder toxicity and myelosuppression.
2. Antimetabolites
- Mechanism: Structurally mimic normal building blocks of DNA/RNA. They interfere with nucleotide synthesis or are incorporated into DNA/RNA in place of normal bases, disrupting replication. They are maximally active in S phase (cell cycle-specific).
- Examples and specifics:
- Methotrexate - inhibits dihydrofolate reductase, blocking folate metabolism; reversed by leucovorin
- 5-Fluorouracil (5-FU) - inhibits thymidylate synthase; causes mucositis and hand-foot syndrome
- Capecitabine - oral prodrug of 5-FU
- 6-Mercaptopurine (6-MP) - purine analog; dose must be reduced 50-75% when given with allopurinol
- Cytarabine (Ara-C) - used in acute leukemias
- Gemcitabine - used in pancreatic and lung cancers
3. Antitumor Antibiotics (Cytotoxic Antibiotics)
- Anthracyclines (doxorubicin, daunorubicin, idarubicin):
- Intercalate into DNA and inhibit topoisomerase II, blocking DNA/RNA synthesis
- Generate free radicals that cause DNA strand breaks
- Most serious toxicity: irreversible, dose-dependent cardiotoxicity leading to left ventricular dysfunction and heart failure; monitored by LVEF; dexrazoxane can reduce this risk
- Must be given IV; extravasation causes tissue necrosis; urine may turn red
- Bleomycin:
- Forms DNA-bleomycin-Fe2+ complex that generates hydroxyl radicals, causing DNA strand breaks
- Cell cycle-specific (G2 phase)
- Used in testicular cancer and Hodgkin lymphoma
- Key toxicity: pulmonary fibrosis (irreversible)
4. Topoisomerase Inhibitors
- Mechanism: Topoisomerase enzymes normally unwind DNA for copying. These drugs trap the enzyme-DNA complex, causing lethal DNA strand breaks.
- Topoisomerase I inhibitors: Irinotecan, topotecan
- Topoisomerase II inhibitors: Etoposide, doxorubicin
- Risk of secondary malignancy (AML/ALL) with prolonged use
5. Mitotic Inhibitors / Plant Alkaloids
- Vinca alkaloids (vincristine, vinblastine): Bind tubulin and prevent polymerization of microtubules, arresting mitosis; key toxicity is peripheral neuropathy
- Taxanes (paclitaxel, docetaxel): Stabilize already-formed microtubules so they cannot depolymerize, blocking cell division
6. Targeted Therapies (Modern Chemotherapy)
Although sometimes classified separately, these are increasingly part of cancer drug regimens:
- Tyrosine kinase inhibitors (e.g., imatinib for BCR-ABL in CML; erlotinib for EGFR in lung cancer; trastuzumab for HER2 in breast cancer)
- Immune checkpoint inhibitors (e.g., pembrolizumab blocks PD-1 to unleash T-cell anti-tumor activity)
- Hormone therapy (e.g., leuprolide for prostate cancer; aromatase inhibitors for breast cancer)
Combination Chemotherapy
Using multiple agents together (with different mechanisms and non-overlapping toxicities) is more effective than monotherapy because it:
- Provides maximal cell killing within tolerated toxicity
- Covers a broader range of resistant cell lines in a heterogeneous tumor
- Delays or prevents the development of resistant cell lines
Example: R-CHOP for non-Hodgkin lymphoma = Rituximab + Cyclophosphamide + Doxorubicin + Vincristine + Prednisone
- Lippincott Illustrated Reviews: Pharmacology, p. 1214
The Log Kill Phenomenon
Chemotherapy destroys a constant fraction (not a fixed number) of cells per dose (first-order kinetics). For example, a 5-log kill reduces 10⁹ leukemic cells to 10⁴ - the patient enters remission. But since residual cells remain, repeated cycles are necessary. This is why chemotherapy is given in intermittent cycles.
Drug Resistance
- Intrinsic resistance: Some tumors (e.g., melanoma) never respond.
- Acquired resistance: Tumor cells mutate after prolonged drug exposure.
- Multidrug resistance (MDR): The most important mechanism involves overexpression of P-glycoprotein, a transmembrane pump that uses ATP to actively expel drugs from cells. It mediates cross-resistance to structurally unrelated agents including vinca alkaloids, anthracyclines, and dactinomycin.
- Minimized by: short-term intensive therapy, combination regimens.
Pharmacologic Sanctuaries
Some sites are poorly penetrated by chemotherapy:
- CNS - requires intrathecal drug administration or craniospinal irradiation (relevant in ALL)
- Testes - poor drug penetration
- Areas inside solid tumors with poor vascularization
Adverse Effects
| Adverse Effect | Details |
|---|---|
| Myelosuppression | Most common; leads to neutropenia and infection risk; managed with G-CSF (filgrastim) |
| Nausea/Vomiting | Managed with antiemetics (ondansetron, etc.) |
| Mucositis/Stomatitis | GI and oral mucosa damage |
| Alopecia | Hair loss (usually reversible) |
| Cardiotoxicity | Anthracyclines - dose-dependent, can be irreversible |
| Pulmonary fibrosis | Bleomycin |
| Hemorrhagic cystitis | Ifosfamide/cyclophosphamide - prevented by mesna |
| Peripheral neuropathy | Vinca alkaloids, platinum compounds |
| Tumor lysis syndrome | Metabolic emergency from massive cell death - causes hyperuricemia, hyperkalemia, hyperphosphatemia, hypocalcemia; classic in Burkitt lymphoma, T-cell ALL |
| Secondary malignancies | Alkylating agents and topoisomerase inhibitors can themselves cause AML years later |
Wound Healing and Surgery
Chemotherapy can impair wound healing by disrupting cell migration, extracellular matrix production, and angiogenesis. Before elective surgery, the patient's absolute neutrophil count (ANC) should recover. Patients on regimens causing profound neutropenia are poor candidates for implant placement due to infection risk. Multidisciplinary planning between the medical oncologist, resecting surgeon, and reconstructive surgeon is essential.
- Sabiston Textbook of Surgery, p. 185-201
Sources: Lippincott Illustrated Reviews: Pharmacology (16th Ed.); Sabiston Textbook of Surgery; Goodman & Gilman's Pharmacological Basis of Therapeutics; Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.