Lefort I fracure and management. 2. Kaban’s protocol. 3. Composition of cornoys solution and its use. 4. Boundaries of canine space and its contents. 5. Various extra oral approaches to the temporomandibular joint. 6. Kelsey fry’s technique. 7. Garres Osteomyelitis. 8. Genioplasty. 9. Anterior superior alveolar nerve block. 10. Ashley’s flap. Answer from oral surgery with appropriate diagram
Kaban protocol condylar fracture management steps oral surgery
Carnoy solution composition use keratocyst Kelsey Fry technique Ashley flap canine space boundaries oral surgery
Kaban protocol TMJ ankylosis 7 steps oral maxillofacial surgery
Kelsey Fry technique wiring jaw fracture Ashley flap third molar extraoral TMJ approaches preauricular retromandibular
https://ghi.ac.ug/elibrary/ebooks/Fundamentals%20of%20Oral%2…
Ashley flap design third molar surgical extraction oral surgery Ward Mostert flap
https://library.unmas.ac.id/repository/E-FKG0083.pdf
Oral Surgery - Comprehensive Notes
1. LeFort I Fracture and Management
Fracture Line Pattern
- The lower nasal septum
- Lateral walls of both maxillary sinuses
- Palatine bones
- Lower pterygoid plates
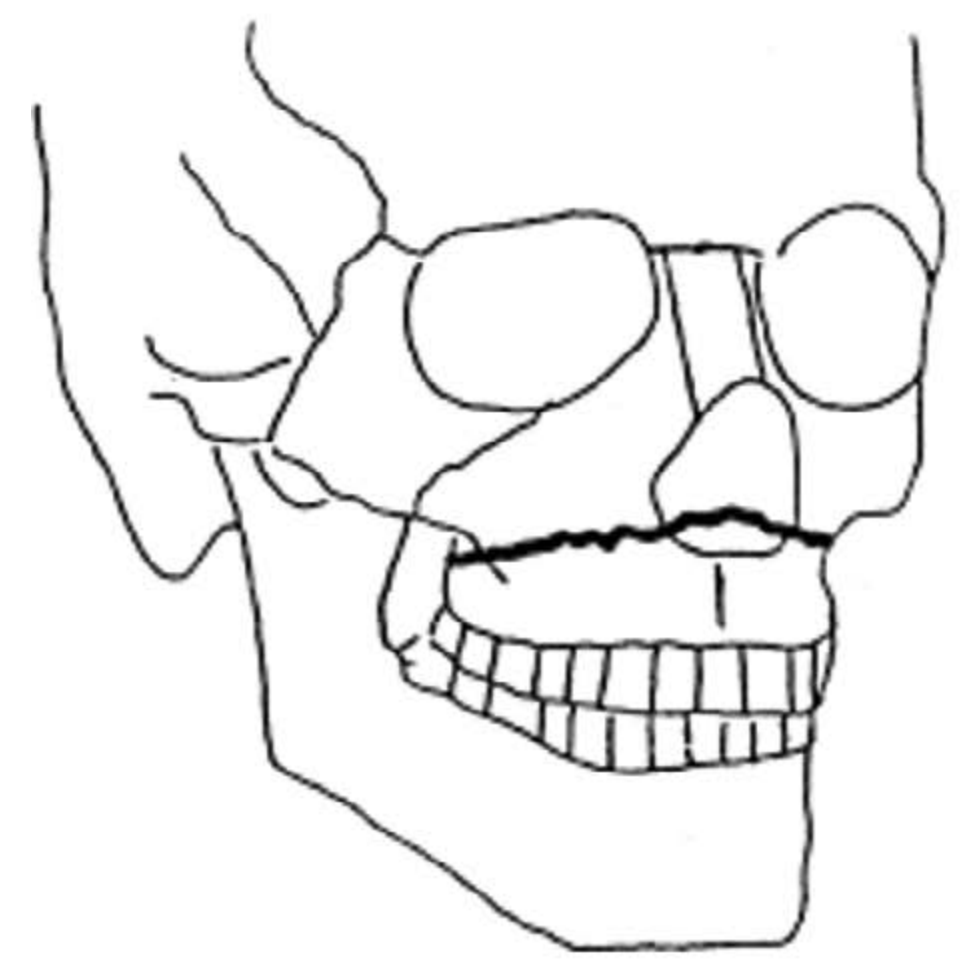
Clinical Features of LeFort I
- Dish-face deformity (not as prominent as LeFort II/III)
- "Cracked cup" resonance on percussion
- Step deformity and tenderness at zygomatico-maxillary suture line
- Abnormal mobility of entire dental arch when grasped
- Anterior open bite, Class III malocclusion
- Epistaxis, intraoral bruising (buccal sulcus ecchymosis)
- "Floating palate" - grasp the upper anterior teeth and attempt to move them
Management of LeFort I
- Airway management - nasopharyngeal airway or intubation (avoid nasotracheal in suspected skull base fractures)
- Control hemorrhage - epistaxis balloon or posterior nasal packing
- IV access, fluid resuscitation if necessary
- CT scan (axial + coronal cuts) to delineate fracture pattern
- Timing: Ideally within 5-10 days (before fibrosis); delayed if patient is unstable
- Access: Gingivobuccal (vestibular) incision from 1st molar to 1st molar bilaterally, subperiosteal dissection
- Re-establish occlusion first: Apply arch bars + intermaxillary fixation (IMF) to restore pre-injury occlusion
- Reduce the fracture: Downfracture with Rowe's disimpaction forceps, then upward repositioning
- Fixation: Titanium miniplates (2.0 mm system) at:
- Bilateral zygomatico-maxillary (ZM) buttresses
- Bilateral pyriform aperture (piriform) rims
- IMF may be released intraoperatively after plate fixation to check occlusion
- Post-op: Soft diet 4-6 weeks; physiotherapy for jaw opening
2. Kaban's Protocol (TMJ Ankylosis Management)
The 7 Steps:
| Step | Action |
|---|---|
| 1 | Aggressive surgical resection of the entire bony/fibrous ankylotic mass, creating a gap of at least 1.0-1.5 cm |
| 2 | Ipsilateral coronoidectomy - always performed to allow passive jaw opening |
| 3 | Contralateral coronoidectomy (intraoral) - performed if passive opening still <35 mm after steps 1 and 2 |
| 4 | Lining of the TMJ with temporalis fascia or native disc (if preserved), or cartilage interposition |
| 5 | Reconstruction of the ramus-condyle unit with a costochondral rib graft (pediatric patients) or total joint prosthesis (adult patients); transport distraction osteogenesis is an alternative |
| 6 | Rigid fixation of the graft/prosthesis with screws/plates |
| 7 | Early mobilization and aggressive physiotherapy starting within days postoperatively, continued for minimum 6 months |
Goals of Kaban's Protocol:
- Mouth opening >35 mm interincisal
- Lateral excursions present
- Minimal or no pain on function
- Resumption of normal diet
- Mean postoperative interincisal opening at 1 year was 37.5 mm (292% increase from preoperative mean) in the original series
Key Points:
- Failure/reankylosis is most commonly due to inadequate resection - especially insufficient medial bone removal
- 3D CT is recommended preoperatively to define extent of ankylosis
- The ankylotic mass on the medial side (displaced condylar fragment) must be completely excised
- Physiotherapy compliance is the single most important factor for sustained success
3. Carnoy's Solution - Composition and Use
Composition (per 10 mL):
| Component | Amount |
|---|---|
| Ethanol (95%) | 6 mL |
| Chloroform | 3 mL |
| Glacial acetic acid | 1 mL |
| Ferric chloride | 1 g |
Modified Carnoy's Solution (without chloroform - safer version):
- Ethanol: 6 mL
- Glacial acetic acid: 3 mL
- Ferric chloride: 1 g (chloroform omitted due to hepatotoxicity concerns)
Uses in Oral Surgery:
-
Odontogenic Keratocyst (OKC/KCOT) - Primary use:
- Applied directly to the bone cavity walls after enucleation of the cyst
- Applied for 3-5 minutes with cotton gauze
- The solution penetrates and destroys residual epithelial remnants and satellite cysts within the bone
- Significantly reduces the recurrence rate of OKC (from ~25-30% with enucleation alone to ~2-3% with Carnoy's)
-
Ameloblastoma - chemical adjunct after conservative surgery
-
General use: Chemical cauterization of aggressive odontogenic lesions after enucleation
Mechanism of Action:
- Ferric chloride precipitates proteins (acts as a protein coagulant)
- Acetic acid decalcifies bone and enhances penetration
- Ethanol denatures proteins
- The solution penetrates 1.54 mm into cancellous bone (Voorsmit's original study)
- Chloroform increases lipid solubility and tissue penetration depth
Precautions:
- Protect neurovascular structures (infraorbital nerve, mental nerve, inferior alveolar nerve) with petroleum gauze
- Do not use near the inferior alveolar canal
- Irrigate thoroughly with saline after the 3-minute application
- Chloroform-containing form is carcinogenic/hepatotoxic - modified formula preferred
4. Boundaries of the Canine Space and Contents
Boundaries:
| Boundary | Structure |
|---|---|
| Anterior | Nasal cartilage (lateral aspect) |
| Posterior | Buccal space |
| Deep (floor) | Levator anguli oris muscle + anterior surface of maxilla (canine fossa) |
| Medially | Levator labii superioris alaeque nasi |
| Laterally | Zygomaticus major muscle |
| Superiorly | Quadratus labii superioris (levator labii superioris) |
| Inferiorly | Oral mucosa + orbicularis oris |
Contents:
- Angular artery and vein (terminal branch of facial artery)
- Infraorbital nerve (exits through infraorbital foramen)
- Loose areolar connective tissue
- Levator anguli oris muscle (forms the floor)
Clinical Features of Canine Space Infection:
- Swelling in the cheek anterior to the canine fossa, lateral to the nose
- Obliteration of the nasolabial fold (pathognomonic)
- Swelling may extend into the labial sulcus
- Danger: Infection may spread via angular vein to facial vein and then to cavernous sinus (cavernous sinus thrombosis)
Drainage:
- Intraoral route: Incision in upper labial sulcus at the level of the canine apex; blunt dissection directed superiorly, avoiding the infraorbital nerve
- Extraoral route (rare): Small incision at the alar base, directed toward the canine fossa
5. Extra-oral Approaches to the Temporomandibular Joint
Classification of Approaches to the TMJ:
| Approach | Description |
|---|---|
| Preauricular (Blair, 1914) | Hockey stick incision in the preauricular region |
| Angulated vertical (Thoma, 1945) | Vertical preauricular incision |
| Al-Kayat & Bramley (1979) | Reverse question-mark / inverted question mark incision - GOLD STANDARD |
| Postauricular (Alexander, 1975) | Incision behind the ear |
| Endaural (Rongetti, 1954) | Incision within the ear canal |
| Submandibular (Risdon, 1934) | Incision 1.5-2 cm below the lower border of mandible |
| Retromandibular (Hinds & Girotti, 1967) | Incision in retromandibular region |
| Bicoronal/Hemicoronal (Pogrel, 1991) | Scalp incision for extensive access |
| Intraoral endoscopic | Minimally invasive |
Al-Kayat and Bramley (Preferred) Approach - Detail:
- Incision: Reverse question-mark shaped; begins in the temporal scalp (~3 cm above the zygomatic arch), curves downward anterior to the auricle, ending at the inferior border of the tragus
- In the temporal region, the blade is angled at 45° to protect hair follicles
- Dissection proceeds through skin, subcutaneous tissue to the superficial temporal fascia (glistening white layer)
- Superficial temporal artery and vein are preserved within the flap (only transverse facial artery is ligated)
- Above the zygomatic arch: dissection is between the superficial temporal fascia and the deep temporal fascia (this protects the temporal branch of the facial nerve)
- Below the zygomatic arch: the periosteum over the zygomatic arch is incised and elevated
- The outer capsule of the TMJ is exposed and incised
- Advantage: Best exposure, protection of the temporal and zygomatic branches of the facial nerve, excellent cosmesis
Retromandibular Approach (Hinds):
- Incision 3 cm long, 0.5 cm posterior to the posterior border of the ramus
- Passes through platysma, parotid capsule, and blunt dissection through the parotid gland
- Good for condylar fractures (subcondylar access)
6. Kelsey Fry's Technique (Lingual Split Bone Technique)
Indication:
- Impacted mandibular third molars with distal and lingual inclination
- Horizontally impacted teeth
- Young patients with elastic (pliable) bone where lingual plate is thin (<1 mm)
Principle:
Steps:
- Anesthesia: Inferior alveolar nerve block + lingual nerve block (or GA)
- Flap design: Standard incision - sulcular from the distal of the second molar, with a distal relieving incision along the external oblique ridge toward the anterior border of the ramus; a mucoperiosteal flap is elevated buccally AND lingually
- Lingual periosteum elevation: Lingual soft tissue flap is elevated carefully using a Howarth's periosteal elevator; a Bowdler-Henry retractor is placed to protect the lingual nerve
- Bone removal (minimal buccal): Only a small amount of buccal bone is removed to expose the crown
- Sectioning: Using a straight chisel (Gardner 4 mm or Chandler 5 mm) and Mead mallet, a cut is made in the distolingual bone to weaken the lingual plate
- Splitting the lingual plate: A curved chisel is placed between the tooth and the lingual plate; a mallet tap fractures the thin lingual cortex
- Luxation and delivery: The tooth is displaced lingually using an elevator (Warwick James or Coupland) and delivered through the lingual side
- Wound closure: Socket irrigated, lingual flap repositioned, sutured
Advantages:
- Minimal buccal bone removal
- Quick procedure
- Less trismus (sparing the masseter region)
Disadvantages / Complications:
- Risk of lingual nerve injury (most serious complication) - 0.2-22% temporary, 0-2% permanent
- Infection spreading to sublingual or parapharyngeal space
- Excessive hemorrhage from lingual soft tissue
- Edema near the airway
- Uncomfortable under local anesthesia (chisel and mallet)
Davis Modification (1983):
- Lingual periosteum is NOT elevated when sectioning the lingual plate
- Reduces risk of lingual nerve injury
7. Garre's Osteomyelitis
Definition:
Synonyms:
- Chronic nonsuppurative sclerosing osteomyelitis
- Chronic osteomyelitis with proliferative periostitis
- Periostitis ossificans
- Focal gross thickening of the periosteum
Etiology:
- Low-virulence infection, usually from a periapical abscess of a vital or non-vital molar (commonly mandibular first molar in children/young adults)
- Organism: Usually Streptococcus viridans (alpha-hemolytic streptococcus)
- Seen almost exclusively in children and young adults (because their periosteum is highly osteogenic and reactive)
Pathophysiology:
Clinical Features:
- Hard, non-tender (or mildly tender) bony swelling over the inferior mandibular border
- Usually unilateral, overlying a carious/pulpitis-affected molar
- Overlying skin is normal (no sinus tract)
- No trismus in early stages
- Patient is generally in good health
Radiographic Features:
- "Onion-skin" periosteal layering on the buccal/inferior surface of the mandible - pathognomonic
- "Fingerprint" or "orange-peel" appearance of periosteal new bone
- Thickened inferior cortex
- OPG and lateral oblique: laminated periosteal reaction
- CT: shows detailed layering and extent of periosteal reaction
Histopathology:
- Layers of woven/lamellar new bone separated by fibrovascular connective tissue
- Minimal inflammatory infiltrate (low-grade)
- No necrotic bone (no sequestrum)
Management:
- Eliminate the cause: Extraction of the offending tooth (carious molar) OR endodontic treatment if tooth is restorable
- Antibiotics: Penicillin V or amoxicillin for 7-10 days (to eliminate residual infection)
- The periosteal new bone involutes spontaneously over 6-12 months after removal of the causative tooth - this is a key feature
- If the lesion does not resolve: surgical decortication/removal of the exostosis
- Follow-up with OPG at 6 and 12 months to confirm resolution
8. Genioplasty
Definition:
Types of Genioplasty:
| Type | Deformity Corrected |
|---|---|
| Advancement (sliding) genioplasty | Horizontal chin deficiency (microgenia) |
| Reduction genioplasty | Chin prominence (macrogenia) |
| Vertical lengthening | Vertical chin deficiency |
| Vertical shortening | Vertical chin excess |
| Asymmetry correction | Transverse chin asymmetry |
| Alloplastic (implant) | Minor horizontal deficiency only |
Osseous Genioplasty - Surgical Technique:
- Anesthesia: General anesthesia with nasotracheal intubation; or local with sedation
- Incision: Intraoral vestibular incision in the lower lip mucosa, 5-10 mm anterior to the attached gingiva, from canine to canine; extends through mucosa, orbicularis oris muscle, and periosteum
- Subperiosteal dissection: Exposes the anterior surface of the chin; mental nerves are identified and carefully preserved bilaterally (exit at mental foramina between premolars)
- Osteotomy line: Marked with a bur at least 5 mm below the apices of the lower teeth (to avoid tooth roots) and 5 mm below the mental foramina; the cut is made with an oscillating saw or reciprocating saw
- Down-fracture: The distal chin segment is fractured downward
- Repositioning: The segment is moved anteriorly (advancement), posteriorly (reduction), superiorly (shortening), or inferiorly (lengthening) as required
- Fixation: Step plates (Synthes 2.0 mm stepping plates) or straight miniplates with screws stabilize the repositioned segment
- Wound closure: Mental muscle is re-suspended to periosteum (important to avoid witch's chin deformity); mucosa is closed with resorbable sutures
Alloplastic Implant (Alternative for Simple Horizontal Deficiency):
- Silastic/PTFE implant placed via same vestibular incision
- Subperiosteal pocket created over chin
- Implant centered on the midline using the mental symphysis landmark
- Secured with a screw or sutures
- Limitations: Fixed range of sizes, cannot correct vertical or transverse asymmetries, risk of bone resorption under implant
Complications:
- Mental nerve hypoesthesia/paresthesia (most common)
- Witch's chin deformity (mentalis muscle dehiscence)
- Relapse of position
- Implant malposition, extrusion, infection
- Asymmetric chin healing
9. Anterior Superior Alveolar Nerve Block
Anatomy:
- Maxillary central incisors
- Maxillary lateral incisors
- Maxillary canine (and associated labial gingiva/periodontium)
Indication:
- Dental procedures on maxillary central incisor, lateral incisor, and canine (on the ipsilateral side)
- Lacerations or injuries requiring anesthesia from the central incisor to the canine
Technique:
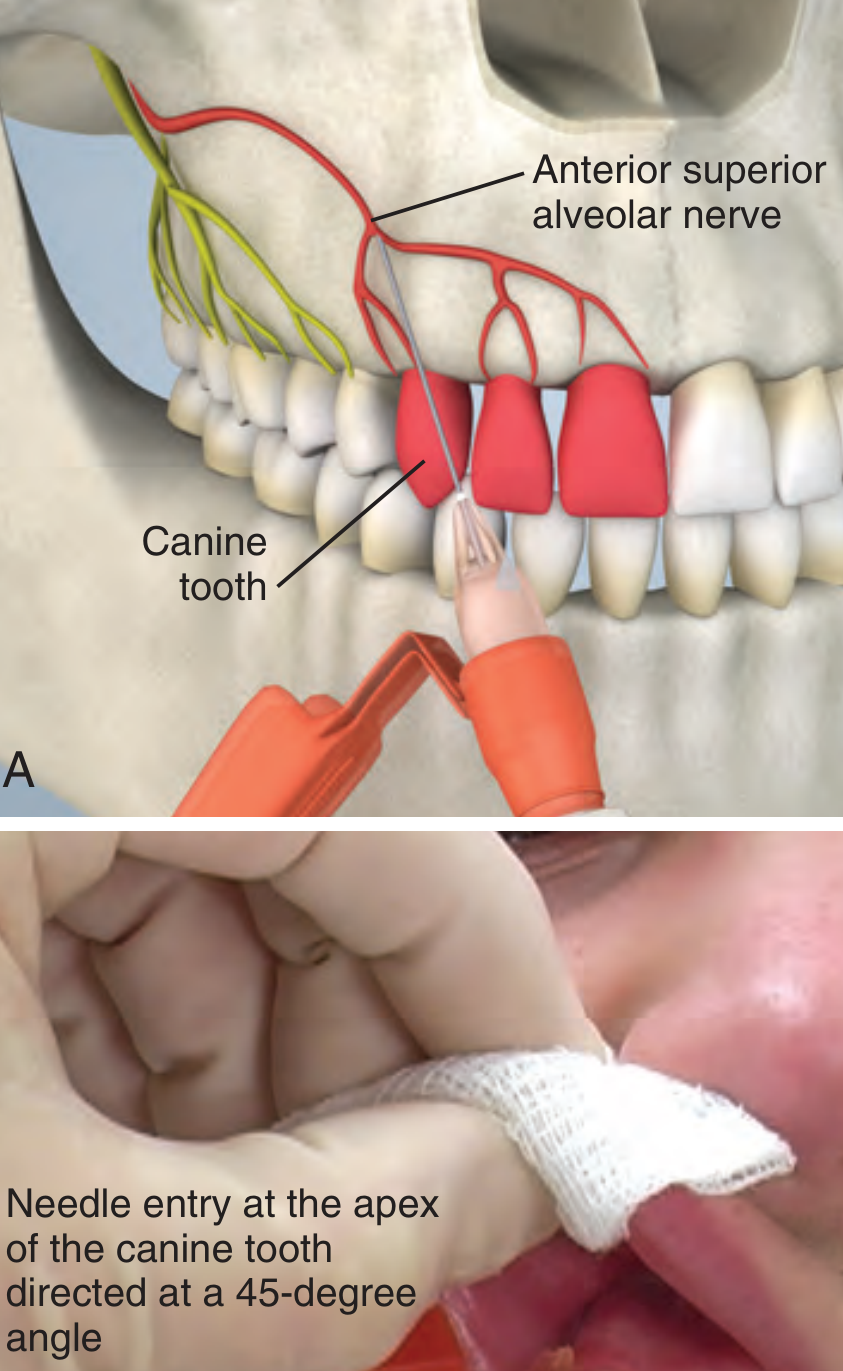
- Apply topical anesthetic (2% benzocaine gel) to the mucosa at the injection site for 1-2 minutes
- Landmark: Apex of the maxillary canine tooth; locate the height of the mucosal reflection (mucobuccal fold) at this level
- Needle insertion: Insert needle at the height of the mucosal reflection at the level of the canine apex
- Angulation: Direct the needle at a 45-degree angle toward the root apex
- Depth: 5 mm
- Aspirate (negative pressure); inject 1-2 mL of local anesthetic slowly
- Onset: 3-5 minutes
Complications:
- Inadvertent block of the infraorbital nerve (if needle is inserted too deep) - causes cheek and lower lid anesthesia
- Failure if needle is too superficial (anesthetic does not reach the nerve)
- Failure if MSAN is absent (will need supplemental infiltration)
- Hematoma (rare)
10. Ashley's Flap
Definition:
Design:
- A sulcular (envelope) incision runs around the necks of the second and first molars in the buccal sulcus
- A distal incision runs distally and slightly buccally from the distal of the second molar along the external oblique ridge (NOT directly down the anterior border of the ramus, which risks lingual nerve injury)
- An anterior vertical releasing incision is placed at the mesial of the first molar (or distal line angle of the second premolar), extending into the buccal vestibule
Key Features Distinguishing Ashley's Flap:
- The distal incision is placed along the external oblique ridge (buccal), keeping it away from the lingual nerve
- The anterior vertical relieving incision at the mesial of the first molar provides adequate retraction and access without excessive tissue tension
- The incision base is broad (wider than the free margin), ensuring good blood supply
Advantages:
- Good visualization and access to the third molar and overlying bone
- Wound closure is on sound bone (minimizes postoperative complications)
- Reduces risk of alveolar osteitis compared to envelope flap alone
- Better control of the flap margin
Comparison of Flap Designs for Lower Third Molar:
| Flap | Design | Notes |
|---|---|---|
| Envelope flap | Sulcular only; no releasing incision | Simple but limited access |
| Triangular flap | Sulcular + distal + mesial vertical release | Good access; risk of wound dehiscence |
| Ashley's (modified) | Sulcular + distal (along ext. oblique) + mesial vertical at first molar | Best combination of access and healing |
| Ward's flap | Crescent-shaped sulcular | Historical |
Closure:
- After tooth removal and socket irrigation, the flap is repositioned
- Primary closure is achieved with 3-0 silk or resorbable sutures at the releasing incision and distal to the second molar
- The sulcular component heals without sutures or with interrupted sutures at the mesial of the second molar
Quick Reference Summary Table
| Topic | Key Fact |
|---|---|
| LeFort I | Horizontal fracture above tooth apices; floating palate; managed with ORIF at ZM buttress + pyriform rim |
| Kaban's Protocol | 7 steps for TMJ ankylosis; aggressive resection + coronoidectomy + CCG + early physio |
| Carnoy's Solution | Ethanol 6 mL + Chloroform 3 mL + Glacial acetic acid 1 mL + FeCl3 1 g; used for OKC for 3 min |
| Canine Space | Between levator anguli oris and levator labii superioris alaeque nasi; contains angular vessels and infraorbital nerve |
| TMJ Approaches | Al-Kayat & Bramley (preferred); preauricular, endaural, retromandibular, submandibular |
| Kelsey Fry | Lingual split technique (1933); fractures lingual plate; risk of lingual nerve injury |
| Garre's Osteomyelitis | Periostitis ossificans; onion-skin pattern; young patients; treat by extracting causal tooth |
| Genioplasty | Horizontal osteotomy of mentum; 5 mm below apices and foramina; step plates for fixation |
| ASAN Block | At apex of canine; 45° angle; 5 mm depth; 1-2 mL; innervates incisors and canine |
| Ashley's Flap | Modified triangular flap; distal cut on external oblique ridge; mesial vertical at first molar |
II. Write Notes on: (10 x 5 = 50) 1. Alveolar osteitis. 2. Oro antral fistula. 3. War lines. 4. CSF rhinorrhea. 5. Bi-rotational Insertion technique. 6. Eutectic mixture of local anesthetic. 7. Lingual split technique. 8. Moist heat sterilization. 9. Kazanjian procedure. 10. Tic doulereaux.
war lines growth arrest lines bone radiology oral surgery oroantral fistula Rehrmann flap Kazanjian procedure vestibuloplasty
war lines growth arrest lines oral surgery maxillofacial bi-rotational insertion technique dental implant Kazanjian vestibuloplasty procedure steps
war lines Harris lines growth arrest lines mandible bone radiology significance oral surgery
bi-rotational insertion technique root canal endodontics dentistry
https://codental.uobaghdad.edu.iq/wp-content/uploads/sites/1…
Kazanjian procedure vestibuloplasty steps technique indications mandible preprosthetic surgery
https://ternadental.com/wp-content/uploads/59.-Pre-Prostheti…
Short Notes in Oral Surgery (10 × 5 Marks)
1. Alveolar Osteitis (Dry Socket)
Definition:
Synonyms: Dry socket, Localized osteitis, Fibrinolytic osteitis
Incidence: Affects approximately 3-4% of all extractions; rises to 20-30% for mandibular third molar extractions.
Etiology and Predisposing Factors:
| Factor | Mechanism |
|---|---|
| Smoking | Nicotine causes vasoconstriction, impairs clot formation; physical suction dislodges clot |
| Oral contraceptives (OCP) | Elevated estrogen increases fibrinolysis |
| Traumatic extraction | Excessive surgical trauma devitalizes bone |
| Dry socket history | 10x recurrence risk |
| Pericoronitis | Pre-existing infection activates fibrinolysis |
| Mandibular location | Dense cortical bone, poorer blood supply |
| Systemic diseases | Diabetes, immunocompromise |
Pathophysiology:
Clinical Features:
- Onset: 2nd or 3rd postoperative day (distinguishes it from normal post-extraction pain which improves by day 2)
- Severe, throbbing, deep-seated pain - often radiating to the ear, eye, and temple
- Pain is disproportionate and poorly controlled by standard analgesics
- Socket is empty of clot - bare bone visible
- Grey/yellowish necrotic debris or granulation tissue may line the socket
- Fetid odor (halitosis) due to decomposing clot/debris
- No pus, no lymphadenopathy (distinguishes from infection)
- Regional lymphadenopathy absent or minimal
Diagnosis: Clinical - based on history and examination. No investigations required.
Management:
- Irrigation: Gently irrigate the socket with warm sterile saline or chlorhexidine 0.12% to remove debris. Do NOT curette aggressively.
- Intra-socket dressing: Pack the socket with a medicated dressing:
- Alvogyl (most commonly used) - contains iodoform, eugenol, butamben, and fibrin - provides analgesic + antimicrobial effect
- Whitehead's varnish gauze (bismuth iodoform paraffin paste - BIPP)
- Change dressings every 2-3 days until symptoms resolve (usually 5-7 days)
- Analgesics: NSAIDs (ibuprofen 400 mg TDS) + paracetamol
- Antibiotics: Not routinely indicated; use only if systemic signs of infection appear (metronidazole or amoxicillin)
- Patient instruction: Avoid smoking, hot liquids; soft diet; maintain oral hygiene around the socket
- Healing: Socket heals by secondary intention over 2-4 weeks once dressings are maintained
Note: Local curettage to induce fresh bleeding (re-clotting) as described in some older texts is not recommended as it causes additional trauma.
2. Oro-Antral Fistula (OAF)
Definition:
Causes / Etiology:
- Most common: Extraction of maxillary posterior teeth (upper 6, 7 - roots near antrum)
- Implant surgery in the posterior maxilla
- Trauma/fracture involving the sinus floor
- Periapical or periodontal disease perforating the sinus floor
- Osteomyelitis, malignancy
- Radical antral surgery (Caldwell-Luc)
- Osteoradionecrosis
Clinical Features / Symptoms:
- Fluid regurgitation from mouth to nose (nose bleed or drainage when drinking)
- Positive Valsalva test: air hissing through the socket on nose-blowing
- Cheek-blowing test: fine hissing sound and air bubbles at the socket
- Post-nasal drip, unilateral nasal discharge
- Reduced sense of smell
- Halitosis, altered voice
- If chronic: recurrent sinusitis, cheek swelling, purulent discharge
Diagnosis:
- Clinical examination and Valsalva test
- OPG - loss of sinus floor bony continuity, often with opacification of the antrum
- CT scan (axial + coronal) - confirms sinus involvement, shows extent of defect
Classification by Size:
- Small: <3 mm - may heal spontaneously
- Medium: 3-5 mm - conservative or simple primary closure
- Large: >5 mm - requires flap closure
Management:
- Encourage clot formation, pack with Surgicel or BIPP
- Avoid nose-blowing, Valsalva; nasal decongestants
- Amoxicillin + metronidazole 7 days; chlorhexidine mouthwash
- Two divergent (trapezoidal) incisions made buccally from each side of the fistula
- Broad-based mucoperiosteal flap raised
- Fistula margins freshened/de-epithelialized
- Horizontal periosteal releasing incision at the base of the flap (allows advancement without tension)
- Flap advanced medially to cover the defect
- Sutured in two layers (periosteum + mucosa)
- Disadvantage: Reduces vestibular depth
- For large defects; fat pad mobilized through a buccal incision and pulled over the defect
- Re-epithelializes spontaneously over 3-4 weeks
- Palatal rotation-advancement flap: Uses greater palatine artery pedicle; rotated to cover defect - but only suitable for premolar region defects
- Palatal hinged (inversion) flap: Mucosa inverted into the fistula as a lining layer
- Caldwell-Luc antrostomy if chronic sinusitis is present (to drain and clear the sinus)
- Irrigation with warm saline via the OAF site preoperatively
3. War Lines (Growth Arrest Lines / Harris Lines)
Definition:
Historical Note:
- First documented by Harris (HA Harris, 1926-1927)
- Further studied by Park (1964)
Synonyms:
Pathophysiology:
Causes of Formation:
- Malnutrition / starvation (most classic)
- Severe systemic illness (septicaemia, high fever)
- Chemotherapy / radiation
- Wartime food deprivation (hence "War lines" in forensic/historical contexts)
- Scurvy, rickets
- Post-traumatic (growth plate injury)
Radiographic Features:
- Dense, transverse radiopaque lines perpendicular to the long axis of bone
- Seen at the metaphysis of long bones (tibia, femur, radius - most common sites)
- Parallel to the growth plate
- Multiple lines in the same bone indicate multiple episodes of arrest
- In jaw bones: may be seen in the mandibular symphysis and alveolar bone in cases of severe childhood deprivation
Histological Features:
- Non-lamellar appearance
- Complete lack of osteocyte lacunae within the line
- Presence of irregularly distributed tubular structures
- Trabeculae immediately above and below the line are normal
Significance in Oral Surgery / Forensics:
- Indicator of past childhood stress/illness/malnutrition
- Used in forensic anthropology to estimate health history of individuals
- In clinical practice: indicates that patient suffered significant systemic stress during skeletal development
- Post-traumatic Harris lines can help assess growth disturbance after physeal injuries
- In the jaw: may correlate with deficient alveolar development, affecting implant planning
Differential Diagnosis:
- Lead lines (Burton's lines) - dense bands in metaphysis due to heavy metal deposition (lead, arsenic, bismuth) - appear similar but are due to hypermineralization, not growth arrest
- Bone infarcts
- Metaphyseal chondrodysplasia
4. CSF Rhinorrhea
Definition:
Causes / Etiology:
| Category | Examples |
|---|---|
| Traumatic (most common - 80%) | Anterior skull base fracture (ethmoid, cribriform plate, sphenoid); facial fractures (LeFort II, III, NOE fractures) |
| Iatrogenic | Endoscopic sinus surgery (FESS), pituitary surgery, anterior skull base surgery; inadvertent injury to cribriform plate/LLCP |
| Spontaneous (non-traumatic) | Elevated ICP (idiopathic intracranial hypertension/BIH), meningocele/meningoencephalocele |
| Neoplastic | Erosion by malignant tumor |
| Congenital | Defects in the cribriform plate or sphenoid |
Clinical Features:
- Unilateral, watery, clear nasal discharge - typically intermittent, worse on bending forward or straining
- Post-nasal drip
- "Halo sign" or "target sign" - if CSF-contaminated blood is placed on filter paper, a clear halo forms around a central blood spot
- Salty/sweet taste (patient may describe a salty metallic taste)
- Meningism (headache, neck stiffness) - especially if complicated by meningitis
- Anosmia (olfactory nerve involvement)
Diagnosis:
- Beta-2 transferrin (Beta-2 transferrin assay): Pathognomonic for CSF - this protein is found only in CSF (and perilymph), not in nasal secretions, tears, or serum. Gold standard confirmatory test.
- Beta-trace protein (prostaglandin-D synthase): Alternative marker, high sensitivity
- Glucose: CSF glucose >30 mg/dL in nasal secretion is suggestive (but not specific - may be positive in diabetics)
- CT cisternography: Intrathecal injection of contrast + CT imaging - locates the site of leak
- HRCT skull base (coronal): Shows bony defect in the skull base/cribriform plate
- MRI (T2W/CISS): Non-invasive; shows high-signal CSF tract through the defect
- Radionuclide cisternography: Radiolabeled technetium-DTPA injected intrathecally; pledgets placed in nose to detect radioactivity
Management:
- Bed rest with head elevation (30° - reduces CSF pressure)
- Strict instructions: no nose-blowing, no Valsalva, no straining
- Lumbar drain - to reduce CSF pressure and allow spontaneous healing (drain 200-300 mL/day for 5-7 days)
- Prophylactic antibiotics (controversial - risk of meningitis vs. antibiotic resistance)
- Most traumatic CSF leaks resolve within 7-10 days
- Endoscopic endonasal repair (EER) - gold standard; plugging the defect with fat, fascia lata, mucoperichondrium (mucosal graft) using fibrin glue
- Craniotomy for large defects not amenable to endoscopic access
- Intracranial pressure management (acetazolamide, weight loss, VP shunt if IIH)
- CSF rhinorrhea may complicate LeFort II, LeFort III fractures, or NOE fractures
- Suspected if clear watery fluid flows from the nose after mid-face trauma
- Nasotracheal intubation is contraindicated if skull base fracture/CSF rhinorrhea is suspected
5. Bi-Rotational Insertion Technique (Bi-Directional Needle Rotation Technique)
Definition:
Rationale:
- Causes the needle tip to miss the intended target (reduces accuracy of nerve blocks)
- Is particularly significant during inferior alveolar nerve (IAN) blocks where needle deflection away from the mandibular foramen can reduce anesthetic success
Mechanism:
Technique:
- The Wand handpiece assembly holds the needle
- As the needle is advanced into tissue, the operator rotates the handpiece assembly alternately clockwise and counterclockwise (like a watch-winder motion)
- The alternating rotation prevents net deflection in one direction
- The computer-controlled pump simultaneously delivers the anesthetic at a controlled, slow rate (0.5 mL/min)
- The needle follows a more accurate, straighter path to the target nerve
Advantages:
- Reduced needle deflection - potentially more accurate needle placement
- The slow, controlled injection rate reduces pain on injection
- Reduced needle trauma to tissues
- Improved patient comfort
Clinical Significance:
- Particularly relevant for the inferior alveolar nerve block where needle deflection can carry the tip away from the mandibular foramen
- Studies (Kennedy et al.) comparing conventional IAN block vs. bi-directional technique in irreversible pulpitis showed no statistically significant difference in anesthetic success (50% vs. 56%)
- Still valuable for its patient-comfort aspects via the CCLAD (computer-controlled local anesthetic delivery) system
The Wand System (CompuDent):
- Computer-controlled constant rate of injection (prevents volume spikes that cause pain)
- Bi-directional rotation capability
- Use with standard dental cartridges
6. Eutectic Mixture of Local Anesthetic (EMLA)
Definition:
Composition:
| Component | Concentration |
|---|---|
| Lidocaine | 2.5% |
| Prilocaine | 2.5% |
| Emulsifying agents (macrogol glycerol hydroxystearate) | - |
| Purified water, Carbomer, Sodium hydroxide (pH ~9) | - |
Mechanism of Action:
Properties:
- Penetrates intact skin (unique among topical anesthetics)
- Requires occlusive dressing (e.g., Tegaderm) over application site
- Onset: 45-60 minutes under occlusion (60-90 minutes for thicker skin)
- Duration: 1-2 hours of anesthesia; effect persists 1-2 hours after removal
- Depth of anesthesia: up to 3-5 mm in skin
Indications (Oral/Dental and General):
- Dental: Pre-injection topical anesthesia of mucosa before needle insertion (intraoral use - onset faster on mucosa, ~15-30 minutes without occlusion)
- Venipuncture / IV catheter placement (especially pediatrics)
- Superficial skin procedures: punch biopsy, minor excisions, laser resurfacing
- Debridement of leg ulcers
- Neonatal circumcision
- Lumbar puncture, vaccination sites in children
Contraindications:
- Methemoglobinemia (prilocaine metabolite ortho-toluidine converts hemoglobin to methemoglobin) - avoid in neonates <3 months, G6PD deficiency, concurrent methemoglobin-inducing drugs
- Known allergy to amide local anesthetics
- Application to broken/inflamed skin (rapid absorption)
- Near the eyes (corneal toxicity)
Side Effects:
- Local: pallor (vasoconstriction from lidocaine), then erythema, transient blanching of skin
- Systemic (rare, at high doses): methemoglobinemia (prilocaine), CNS toxicity, cardiac effects
- Irritant reactions
7. Lingual Split Technique (Kelsey Fry's Technique)
Definition:
History:
Steps:
- LA: IAN block + lingual nerve block
- Standard flap (sulcular + distal incision along external oblique ridge)
- Elevate lingual periosteum with Howarth's elevator; protect lingual nerve with Bowdler-Henry retractor
- Minimal buccal bone removal to expose crown
- Apply Gardner chisel (4 mm) and Mead mallet to create a distolingual cut
- Fracture the lingual plate with a curved chisel
- Luxate and deliver the tooth lingually
- Irrigate and suture
Instruments Required:
- Gardner chisel (4 mm) and Chandler chisel (5 mm)
- Mead mallet (17 cm)
- Howarth's periosteal elevator
- Bowdler-Henry lingual nerve retractor
- Coupland or Warwick James elevator
Indications:
- Lingually inclined or distolingual impacted mandibular third molars
- Young patients with elastic, thin lingual plate
- Horizontal impactions
Advantages:
- Minimal buccal bone removal - faster healing, less trismus
- Less postoperative pain and swelling (masseter not disturbed)
- Quick extraction
Complications:
- Lingual nerve injury (most feared): 0.2-22% temporary; 0-2% permanent
- Sublingual space infection
- Excessive hemorrhage from lingual soft tissue
- Swelling/edema near airway
Davis Modification:
8. Moist Heat Sterilization
Definition:
Types of Moist Heat Sterilization:
- Kills vegetative bacteria, most viruses and fungi within 10 minutes
- Does NOT kill bacterial spores (endospores of Clostridium, Bacillus) at 100°C
- NOT true sterilization - only disinfection
- Used only for items that cannot withstand higher temperatures
| Parameter | Standard Cycle | Flash Cycle |
|---|---|---|
| Temperature | 121°C (250°F) | 134°C (272°F) |
| Pressure | 15 psi (1 atm gauge) | 30 psi |
| Time | 15-20 minutes | 3-4 minutes |
- Gravity displacement (downward displacement): Steam enters from top, displaces cooler air downward and out through a drain. Requires longer cycles.
- Prevacuum (pre-vacuum/high-vacuum): Air is evacuated before steam admission; allows faster penetration into porous loads. More efficient.
- Unsaturated chemical vapor (Harvey Chemiclave): Uses formaldehyde + alcohol + water vapor - less corrosive to instruments.
- Moist heat causes hydrolysis and coagulation of cellular proteins
- Disrupts hydrogen bonds in protein secondary structure
- Destroys cell membrane lipids
- Denatures nucleic acids
- Spore killing is due to protein hydrolysis at the high temperature/pressure combination
- Kills ALL microorganisms including spores, prions (partially), viruses
- Non-toxic, non-residual
- Penetrates porous materials and wrapped instruments
- Economical and rapid
- Universally validated
- Not suitable for heat-sensitive materials (rubber, plastics, some sharp instruments lose edge)
- May cause corrosion of carbon steel instruments
- Requires proper packaging and loading
- Physical: Temperature and pressure gauges, printout recorders
- Chemical indicators (Bowie-Dick test, Class 4-6 indicators): Chemical strip changes color on exposure to correct temperature - only confirms conditions were reached, not true sterility
- Biological indicators (Spore tests): Most reliable; use Geobacillus stearothermophilus spore strips for steam; run weekly. A negative culture after autoclaving confirms sterilization.
- Wrapped instruments: 121°C/15 psi/20 min (gravity) or 134°C/3 min (prevacuum)
- Wrapped textiles: 134°C/3 min (prevacuum)
- Implant instruments: prevacuum cycle preferred
- 63°C for 30 min (holder method) or 72°C for 15 sec (HTST)
- Kills most pathogens but NOT spores - NOT sterilization
- Used for heat-sensitive instruments (e.g., handpieces that can't tolerate autoclaving)
9. Kazanjian Procedure (Kazanjian Vestibuloplasty)
Definition:
Indication:
- Edentulous mandible with a shallow labial vestibule due to resorbed alveolar ridge and/or high muscle attachments (mentalis, orbicularis oris, buccinator)
- Patients requiring complete lower denture with inadequate vestibular depth for stability
- Adequate alveolar bone height present (if bone height is severely deficient, ridge augmentation is needed first)
- Sufficient healthy labial mucosa available for advancement
Classification of Vestibuloplasty Procedures:
- Kazanjian technique (1924)
- Godwin's modification (1947)
- Clark's technique
- Obwegeser's modification (1959)
- Trauner's technique
- Caldwell's technique
Steps of Kazanjian Technique:
-
Anesthesia: Inferior alveolar nerve block + mental nerve block + infiltrations; or general anesthesia
-
Incision: A horizontal incision through the mucosa is made in the labial sulcus at the junction of attached and loose (alveolar) mucosa - at the depth of the existing (shallow) sulcus - from canine to canine (or across the full anterior mandible as needed)
-
Mucosal flap elevation: The incised mucosa is elevated superiorly as a pedicle flap (maintaining its attachment to the lip), exposing the periosteum of the labial bone surface and the underlying mentalis muscle attachments
-
Muscle detachment: The mentalis muscle (and orbicularis oris fibers) is stripped/detached from the periosteum by sharp dissection, releasing the tissue that was tethering the sulcus high
-
Suturing the mucosal flap: The superior edge of the mucosal flap (which remains attached to the inner lip) is sutured downward to the periosteum at the new, lower (deeper) vestibular depth
- This positions the mucosal flap to line the deeper vestibule
- The flap covers the upper part of the denuded periosteum
-
Raw bone periosteum exposed: The lower portion of the exposed periosteum (below the sutured flap) is left bare, to heal by secondary epithelialization (granulation tissue → epithelialization from adjacent mucosa)
-
Stent/Splint placement: A preformed acrylic surgical stent (made from the patient's existing denture or a study cast) is placed over the raw surface and held in position with circumandibular wires or sutures
- The stent maintains the new vestibular depth during healing
- Prevents contraction of the healing wound
-
Post-operative care: Stent kept for 3-4 weeks; new denture fabricated after complete healing (4-6 weeks)
Advantages:
- Deepens the vestibule effectively
- Uses existing mucosa (no donor site needed)
- Relatively simple technique
- Good retention of vestibular depth long-term
Disadvantages:
- Secondary epithelialization leaves a less resilient surface (compared to Clark's mucosal graft technique)
- The raw periosteal surface is painful postoperatively
- Risk of scar contraction and relapse of vestibular depth
- Does NOT address lingual/floor of mouth depth
Differences from Clark's Technique:
| Kazanjian | Clark's | |
|---|---|---|
| Type | Secondary epithelialization | Mucosal graft |
| Raw surface | Left to granulate | Covered with free mucosal graft from palate |
| Tissue quality | Less resilient | More resilient (keratinized graft) |
| Donor site | None | Palatal donor site |
10. Tic Douloureux (Trigeminal Neuralgia)
Definition:
Epidemiology:
- Incidence: ~4-5 per 100,000 per year
- More common in females (slight female predominance)
- Usually affects persons over 50 years (rare in young adults)
- Usually unilateral; bilateral in ~3%
- Most commonly affects V2 (maxillary) and V3 (mandibular) divisions; V1 involvement is rare
Classification:
| Type | Description |
|---|---|
| Classic (Type 1 TN) | Due to vascular compression of the trigeminal root entry zone (superior cerebellar artery most common) |
| Secondary TN | Due to identifiable structural cause: multiple sclerosis, tumor (acoustic neuroma, meningioma), AVM |
| Idiopathic TN | No vascular compression or structural cause on imaging |
Etiopathogenesis:
- Vascular compression theory (most accepted): Pulsatile compression of the trigeminal nerve root by an aberrant blood vessel (usually superior cerebellar artery) causes focal demyelination. This leads to ephaptic transmission (cross-activation between adjacent demyelinated axons) and a hypersensitive, hyperexcitable population of trigeminal neurons.
- Ignition hypothesis (Devor): Nerve injury induces physiologically linked hyperexcitable neurons; discharge of any one neuron rapidly spreads to activate the entire population, causing the sudden synchronous paroxysmal discharge characteristic of TN.
Clinical Features (White and Sweet Diagnostic Criteria):
- Pain character: Paroxysmal, lancinating, electric shock-like, stabbing, or burning
- Duration: Very brief - each attack lasts fractions of a second to 2 minutes
- Location: Strictly confined to the distribution of one or two branches of the trigeminal nerve (V2 and V3 most common)
- Unilateral: Always unilateral during an attack
- Trigger factors (essential feature): Light touch to specific trigger zones causes an attack:
- Trigger zones: nasolabial fold, corner of mouth, chin, cheek, gingiva
- Triggers: gentle touch, talking, chewing, brushing teeth, washing face, shaving, cold wind
- Refractory period: After an attack, a brief refractory period during which triggers do not elicit pain
- No neurological deficit: Sensory and motor function of the trigeminal nerve are normal between attacks (if deficit present, consider secondary TN)
- Pain-free intervals: Patients are completely pain-free between attacks; remissions can last months to years
Differential Diagnosis:
- Dental pain (toothache, pulpitis) - ruled out by dental examination
- Atypical facial pain/persistent idiopathic facial pain
- Cluster headache / SUNCT syndrome
- Glossopharyngeal neuralgia (pain in throat/ear, triggered by swallowing)
- Postherpetic neuralgia (follows herpes zoster rash)
- Temporomandibular disorder
Investigations:
- MRI brain with gadolinium (3T, FIESTA/CISS sequence): To identify vascular compression at the root entry zone (Meckel's cave level) and to exclude secondary causes (MS plaques, tumors)
Management:
| Drug | Dose | Mechanism |
|---|---|---|
| Carbamazepine (1st line) | 200-1200 mg/day in divided doses | Sodium channel blocker; reduces ectopic discharge |
| Oxcarbazepine (preferred if side effects) | 300-1800 mg/day | Sodium channel blocker (fewer drug interactions) |
| Baclofen | 40-80 mg/day | GABA-B agonist; adjunct |
| Lamotrigine | 200-400 mg/day | Sodium channel blocker; adjunct |
| Pregabalin/Gabapentin | Variable | Calcium channel modulator |
- Percutaneous retrogasserian glycerol rhizolysis - glycerol injected into Meckel's cave
- Percutaneous balloon compression - balloon compresses the ganglion
- Percutaneous radiofrequency thermocoagulation (RFT) - heat selectively destroys pain fibers (A-delta, C fibers) while sparing touch (A-beta)
- Posterior craniotomy (retromastoid approach)
- Identify the offending vessel compressing CN V
- Place a Teflon (PTFE) felt pad between the vessel and the nerve
- Relieves compression; non-destructive - preserves sensation
- Long-term success: 70-80% pain-free at 10 years
- Preferred in younger patients with classic TN due to vascular compression
- Oral surgeons and dentists are often the first to see TN patients
- Many patients undergo unnecessary dental extractions thinking the pain is dental
- Recognition of TN is critical to avoid irreversible dental treatment
- Oral surgeons may perform peripheral nerve blocks (infraorbital/inferior alveolar nerve) or peripheral neurectomy as temporizing measures
Quick Summary Table
| Topic | Key Mnemonic/Core Point |
|---|---|
| Alveolar Osteitis | Day 2-3 post-extraction; fibrinolysis; bare bone; Alvogyl dressing; NOT primarily infective |
| OAF | Epithelialized OAC; Valsalva test; Rehrmann buccal flap for closure |
| War Lines | Harris/Park lines; transverse metaphyseal densities; growth arrest due to malnutrition/illness |
| CSF Rhinorrhea | Beta-2 transferrin = gold standard test; LLCP most vulnerable; lumbar drain for conservative Mx |
| Bi-rotational Technique | Alternating CW/CCW needle rotation; reduces needle deflection; Hochman & Friedman; Wand system |
| EMLA | Lidocaine 2.5% + Prilocaine 2.5%; eutectic = lower melting point; penetrates intact skin; 60-min onset |
| Lingual Split | Kelsey Fry 1933; fracture lingual plate; deliver tooth lingually; risk = lingual nerve injury |
| Moist Heat Sterilization | Autoclave 121°C/15psi/20min; biological indicator = Geobacillus stearothermophilus; kills spores |
| Kazanjian Procedure | 1924; labial vestibuloplasty; mucosal flap + periosteal suturing + stent; secondary epithelialization |
| Tic Douloureux | TN; paroxysmal lancinating pain V2/V3; triggers; Carbamazepine 1st line; MVD gold standard surgery |
Pell and Gregory classification of 2. Posterior superior Alveolar nerve block. 3. Tracheostomy. 4. Marsupialisation. 5. TNM classification. 6. Gilley’s temporal approach. 7. Pre anaesthetic medication. 8. Dry socket. 9. Pleomorphic adenoma. 10. Ludwig’s Angina.
Pell Gregory classification impacted mandibular third molar oral surgery Winter classification
marsupialization cyst jaw technique steps indications advantages preanaesthetic medication drugs uses Ludwig angina management tracheostomy oral surgery
Gillies temporal approach zygomatic fracture technique steps instruments elevator oral maxillofacial surgery
preanaesthetic medication drugs atropine midazolam morphine oral surgery general anesthesia indications doses
TNM classification oral cavity head neck cancer 8th edition staging T1 T2 T3 T4 N0 N1
Oral Surgery Short Notes (10 × 5 Marks)
1. Pell and Gregory Classification of Impacted Mandibular Third Molar
Part A - Relationship to the Ramus and Second Molar (Class I, II, III)
| Class | Description |
|---|---|
| Class I | Sufficient space exists between the anterior border of the ramus and the distal surface of the second molar to accommodate the full mesiodistal diameter of the third molar crown. The tooth can erupt |
| Class II | The space between the anterior border of the ramus and the distal surface of the second molar is less than the mesiodistal diameter of the third molar crown. Half of the crown is covered by the ramus |
| Class III | The entire third molar or most of it is within the ramus of the mandible. Very little to no space anterior to the ramus |
Part B - Depth of Impaction Relative to Second Molar (Position A, B, C)
| Position | Description |
|---|---|
| Position A | The occlusal plane of the third molar is at the same level as the occlusal plane of the second molar |
| Position B | The occlusal plane of the third molar is between the occlusal plane of the second molar and the cemento-enamel junction (cervical line) of the second molar |
| Position C | The occlusal plane of the third molar is below the cervical line (CEJ) of the second molar - deeply embedded in bone |
Combined Classification:
Surgical Difficulty:
- Class I, A = Easiest
- Class III, C = Most difficult (maximum bone removal required)
Winter's Classification (Angulation - complementary system):
| Type | Angle | Difficulty |
|---|---|---|
| Vertical | 10° to -10° | Moderate |
| Mesioangular | 11° to 79° | Most common; moderate |
| Horizontal | 80° to 100° | Difficult |
| Distoangular | -11° to -79° | Most difficult |
| Buccolingual | Lateral tilt | Rare; difficult |
| Inverted | Upside down | Very rare |
2. Posterior Superior Alveolar Nerve Block (PSAN Block)
Nerve Blocked:
Indications:
- Extraction of maxillary second and third molars
- Pulp therapy, restorations of upper second and third molars
- Periodontal procedures in the maxillary molar region
- When multiple upper molar teeth require treatment simultaneously
Anatomy:
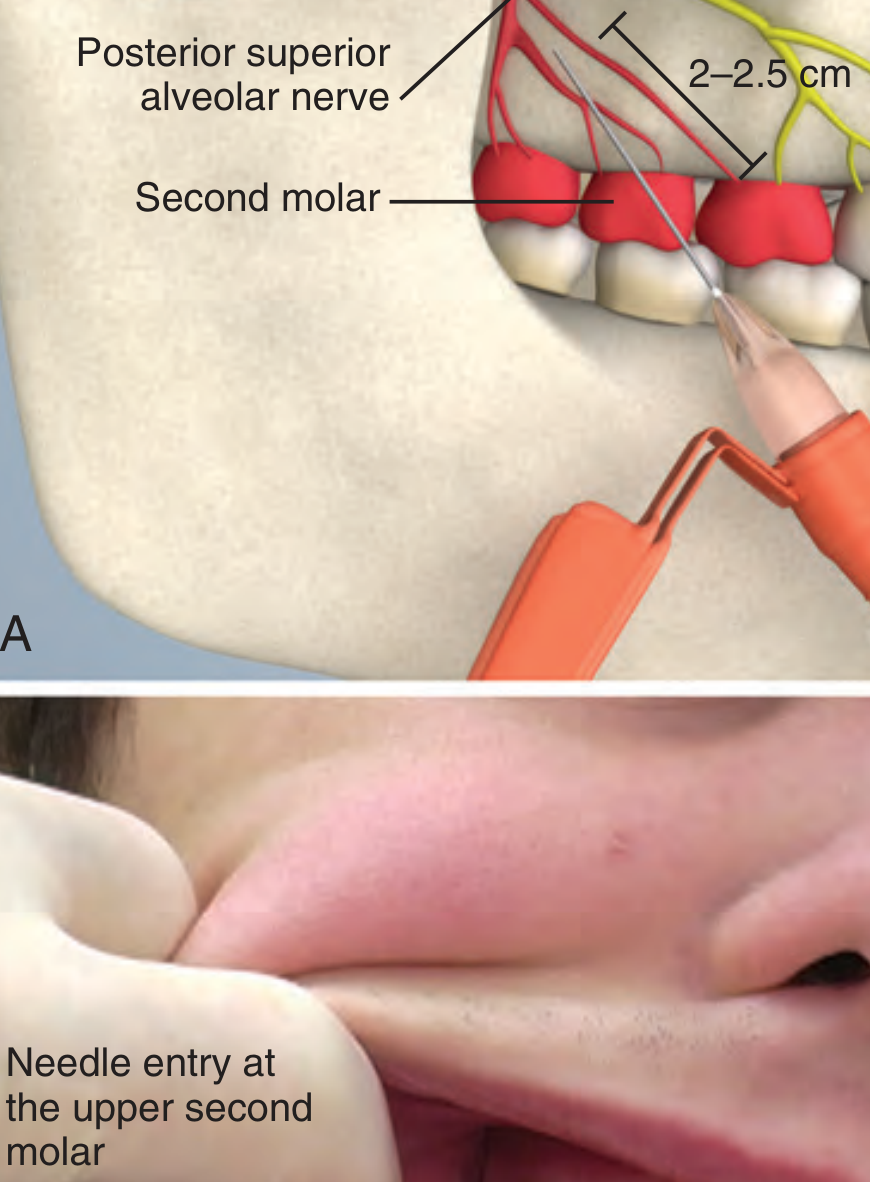
Technique:
- Apply topical anesthetic to the mucosa distal to the upper second molar
- Landmark: Mucobuccal fold above the maxillary second molar
- Needle insertion point: At the height of the mucobuccal fold at the level of the upper second molar (distal aspect)
- Direction: Upward (superiorly) + inward (medially) + backward (posteriorly) toward the maxillary tuberosity at approximately 45° to the occlusal plane
- Depth: 15-25 mm (no more than 25 mm to avoid the pterygoid plexus)
- Volume: Aspirate first; inject 1.5-2 mL slowly over 30-60 seconds
- Onset: 3-5 minutes
Complications:
- Hematoma (most common) - needle pierces pterygoid venous plexus → painful, rapidly expanding hematoma in the infratemporal fossa; prevents further surgery; apply pressure, cold packs
- Diplopia and features resembling Horner syndrome (ptosis, enophthalmos, miosis) - anesthetic spreads to orbital nerves; transient
- Trochlear nerve (CN IV) palsy - rare, transient
- Inadequate anesthesia if the MSAN is present and innervates part of the first molar
- Infection (rare, if sterile technique not maintained)
3. Tracheostomy
Definition:
Indications:
- Acute upper airway obstruction (Ludwig's angina, severe facial trauma, angioedema, burns, foreign body)
- Massive maxillofacial trauma
- When cricothyrotomy is not feasible
- Prolonged mechanical ventilation (>7-10 days)
- Major oral/oropharyngeal/laryngeal surgery (to secure airway and prevent aspiration)
- Bilateral vocal cord palsy
- Obstructive sleep apnea (severe, unresponsive to CPAP)
- Neuromuscular disorders impairing airway protection
- LeFort III fractures with severe mid-face disruption
- Bilateral mandibular fractures with floor-of-mouth hemorrhage
- Ludwig's angina with impending airway compromise
- Radical neck dissection + laryngectomy
- Mandibulotomy for tumor access
Types:
- Standard (open) surgical tracheostomy - in operating theatre under GA
- Percutaneous dilational tracheostomy (PDT) - bedside under bronchoscopic guidance (ICU patients)
- Emergency cricothyrotomy - through cricothyroid membrane (not true tracheostomy; temporary)
Surgical Technique (Standard):
- Position: Patient supine, neck extended (shoulder roll)
- Anesthesia: GA with endotracheal intubation (or local with sedation in emergency)
- Incision: Horizontal skin crease incision 2 cm below the cricoid, OR vertical midline incision 2-3 cm long
- Dissection: Midline dissection through platysma; strap muscles retracted laterally; thyroid isthmus identified and either retracted superiorly or divided and ligated
- Tracheal identification: Confirmed by palpation of tracheal rings; cricoid cartilage identified superiorly
- Tracheal incision: Between the 2nd and 4th tracheal rings (never above the 1st ring - to avoid subglottic stenosis)
- Options: vertical incision, H-shaped incision, Bjork flap (inferiorly based flap of tracheal wall sutured to skin for easy tube re-insertion)
- Tube insertion: Endotracheal tube cuff deflated; tracheostomy tube (cuffed PVC) inserted; cuff inflated; tube secured with tapes
- Wound closure: Loose skin closure around the tube; dressing applied
Complications:
4. Marsupialization
Definition:
Principle:
Indications:
- Large cysts where enucleation would risk fracture of the mandible
- Cysts close to vital structures (inferior alveolar nerve, roots of adjacent vital teeth, antrum floor) where enucleation would cause damage
- Dentigerous cysts - marsupialization can allow the impacted tooth to erupt (particularly in children)
- Odontogenic keratocyst (OKC) - as a first stage to reduce size before enucleation
- Elderly or medically compromised patients in whom extensive surgery is not tolerated (less invasive)
- Infected cysts (drainage required prior to definitive surgery)
Contraindications:
- When histological diagnosis of the entire lesion is needed (enucleation preferred)
- Suspected malignant transformation
- When cyst is small and easily enucleated
Steps (Intraoral approach):
- Anesthesia: Local or general anesthesia
- Incision: A circular or elliptical window of mucosa and bone overlying the most accessible/thinned part of the cyst is excised - the window should be at least 2-3 cm to prevent premature closure
- Cyst wall biopsy: A sample of the cyst wall is sent for histopathology (to exclude malignancy or confirm cyst type)
- Curettage: The infected or necrotic debris is removed; cavity irrigated with saline
- Suturing: The remaining cyst lining is sutured circumferentially to the surrounding oral mucosa using resorbable sutures - creating a continuous epithelial lining from the oral cavity into the cyst (the "pouch")
- Plug/Obturator: A surgical obturator or gauze pack is placed to maintain the opening and prevent premature closure; patient instructed to irrigate with chlorhexidine daily
- Follow-up: OPGs taken at regular intervals (every 3-6 months) to assess reduction in cyst size; when reduced, definitive enucleation may be performed (Waldron's technique = marsupialization followed by enucleation)
Advantages:
- Simple, less traumatic procedure
- Reduces risk of damage to vital structures
- Preserves adjacent teeth vitality and function
- Can allow impacted tooth eruption (dentigerous cyst)
- Reduces cyst size prior to definitive surgery
Disadvantages:
- Prolonged treatment time (months to years)
- Residual cyst lining may undergo transformation (especially OKC)
- Requires patient compliance for irrigation
- Incomplete histopathological assessment
5. TNM Classification (Oral Cavity Cancer)
Key Change in 8th Edition:
T Classification - Primary Tumor (Oral Cavity):
| Stage | Criteria |
|---|---|
| Tx | Primary tumor cannot be assessed |
| Tis | Carcinoma in situ |
| T1 | Tumor ≤2 cm AND DOI ≤5 mm |
| T2 | Tumor ≤2 cm with DOI >5 mm and ≤10 mm, OR tumor >2 cm but ≤4 cm with DOI ≤10 mm |
| T3 | Tumor >4 cm, OR any tumor with DOI >10 mm |
| T4a | Moderately advanced: tumor invades adjacent structures - cortical bone of mandible/maxilla, maxillary sinus, or skin of face |
| T4b | Very advanced: tumor invades masticator space, pterygoid plates, skull base, or encases the internal carotid artery |
Note: Superficial erosion of bone or tooth socket by a gingival tumor alone does NOT qualify as T4.
N Classification - Regional Lymph Nodes (Clinical cN):
| Stage | Criteria |
|---|---|
| N0 | No regional lymph node metastasis |
| N1 | Single ipsilateral lymph node ≤3 cm, ENE negative |
| N2a | Single ipsilateral node >3 cm but ≤6 cm, ENE negative |
| N2b | Multiple ipsilateral nodes, none >6 cm, ENE negative |
| N2c | Bilateral or contralateral nodes, none >6 cm, ENE negative |
| N3a | Any node >6 cm, ENE negative |
| N3b | Any node(s), clinically overt ENE positive |
M Classification:
| Stage | Criteria |
|---|---|
| M0 | No distant metastasis |
| M1 | Distant metastasis present |
Prognostic Stage Groups (Oral Cavity):
| Stage | T | N | M |
|---|---|---|---|
| Stage 0 | Tis | N0 | M0 |
| Stage I | T1 | N0 | M0 |
| Stage II | T2 | N0 | M0 |
| Stage III | T3 | N0 | M0 |
| Stage III | T1,2,3 | N1 | M0 |
| Stage IVA | T4a | N0,1 | M0 |
| Stage IVA | T1,2,3,4a | N2 | M0 |
| Stage IVB | T4b | Any N | M0 |
| Stage IVB | Any T | N3 | M0 |
| Stage IVC | Any T | Any N | M1 |
6. Gillies Temporal Approach
Definition:
Indications:
- Isolated, depressed zygomatic arch fracture causing:
- Facial deformity (flattening of the lateral midface)
- Mandibular hypomobility/trismus (coronoid process impingement beneath the depressed arch)
- Mildly to moderately displaced zygomatic complex fractures (arch component)
Anatomical Basis:
Instruments:
- Freer elevator (for initial dissection)
- Rowe zygomatic elevator (primary reduction instrument - a flat, broad-bladed instrument)
- Bristow elevator (alternative)
- Boise elevator
Steps:
- Anesthesia: GA (preferred) or local with sedation
- Marking: Temporal hairline marked; arch palpated and marked externally
- Incision: A 2 cm horizontal incision within the temporal hairline, approximately 2.5-3 cm above the zygomatic arch (well above the arch to avoid the temporal branch of the facial nerve)
- Dissection layers: Incised through:
- Skin
- Subcutaneous tissue
- Superficial temporal fascia (temporoparietal fascia)
- Deep temporal fascia - opened to enter the correct plane
- Tunnel creation: A Freer elevator is inserted in the plane between the deep temporal fascia and the temporalis muscle and advanced downward using a back-and-forth motion until the tip is medial (deep) to the depressed arch
- Elevation: The Rowe zygomatic elevator (or Bristow elevator) is substituted and positioned just deep to the most depressed part of the arch; an outward (lateral) force is applied to elevate the fracture
- The opposite hand palpates the arch externally throughout to monitor reduction
- Care: Do NOT use the parietal temporal bone as a fulcrum (parietal skull fracture risk)
- Confirmation: Restoration of normal arch contour; resolution of trismus; facial symmetry restored
- Wound closure: Deep temporal fascia approximated; skin closed in layers
Advantages:
- No visible external scar (scar hidden within hairline)
- Protects the temporal branch of the facial nerve
- Quick, effective for isolated arch fractures
Disadvantages:
- Risk of alopecia (hair follicle injury at incision site)
- Cannot be used if arch is comminuted (needs open fixation)
- Cannot directly visualize reduction
Alternatives:
- Intraoral (Keen) approach: Upper buccal sulcus incision (no scar, avoids facial nerve risk)
- Hemicoronal approach: For comminuted/complex arch fractures requiring plating
7. Pre-anaesthetic Medication
Definition:
Goals of Premedication:
- Anxiolysis and sedation - reduce preoperative anxiety
- Amnesia - prevent recall of unpleasant perioperative events
- Analgesia - pre-emptive pain control
- Anti-sialagogue - reduce secretions (important in oral/airway surgery)
- Antiemetic - prevent postoperative nausea and vomiting (PONV)
- Antacid - reduce aspiration risk (prophylaxis against Mendelson's syndrome)
- Facilitate smooth induction - reduce induction dose of anaesthetic agents
- Prevent autonomic reflexes - prevent vagal stimulation, bradycardia
Classification of Premedication Drugs:
A. Anticholinergics (Anti-sialagogues):
| Drug | Dose | Route | Effect |
|---|---|---|---|
| Atropine | 0.6 mg (adult) / 0.02 mg/kg | IM/IV | Anti-sialagogue, prevents bradycardia, bronchodilator |
| Glycopyrrolate | 0.2-0.4 mg | IM/IV | Better anti-sialagogue, does not cross BBB (less CNS effects), no tachycardia |
| Scopolamine (Hyoscine) | 0.4 mg | IM | Anti-sialagogue + sedation + antiemetic + amnesia |
B. Sedatives/Anxiolytics:
| Drug | Dose | Route | Effect |
|---|---|---|---|
| Midazolam | 0.07-0.1 mg/kg IM; 0.5 mg/kg oral | IM/IV/oral | Anxiolysis, amnesia, sedation (short-acting benzodiazepine); MOST COMMONLY USED |
| Diazepam | 5-10 mg | Oral night before + morning | Anxiolysis, sedation |
| Lorazepam | 2-4 mg | Oral | Longer-acting anxiolysis, amnesia |
C. Opioid Analgesics (Narcotic Premedication):
| Drug | Dose | Route | Effect |
|---|---|---|---|
| Morphine | 0.1-0.15 mg/kg | IM | Analgesia, sedation; reduce induction agent dose |
| Pethidine (meperidine) | 1-1.5 mg/kg | IM | Analgesia, less emesis than morphine |
| Fentanyl | 1-2 mcg/kg | IV | Short-acting, powerful analgesia |
D. Antiemetics:
| Drug | Dose | Effect |
|---|---|---|
| Ondansetron (5-HT3 antagonist) | 4-8 mg IV | Antiemetic; first-line |
| Metoclopramide | 10 mg IV | Prokinetic + antiemetic |
| Promethazine | 25 mg IM | Antiemetic + sedation |
| Dexamethasone | 4-8 mg IV | Reduces PONV + postoperative edema |
E. H2 Blockers/Antacids (Aspiration prophylaxis):
| Drug | Dose | Effect |
|---|---|---|
| Ranitidine | 150 mg oral night before | Reduces gastric acid volume and pH |
| Sodium citrate (clear antacid) | 30 mL oral | Immediately neutralizes gastric acid |
| Omeprazole | 40 mg | Proton pump inhibitor; used in high-risk patients |
F. Others:
- NSAIDs (ibuprofen, diclofenac, parecoxib) - pre-emptive analgesia
- Paracetamol - adjunct analgesia
- Beta-blockers - for cardiac patients (continue existing medications)
- Clonidine (α2 agonist) - reduces intraoperative anesthetic requirements, reduces PONV
Typical Premedication Protocol for Oral Surgery (GA):
| Time | Drug |
|---|---|
| Night before | Oral diazepam 5 mg (anxious patients) + ranitidine 150 mg |
| 2 hours before | Sodium citrate 30 mL oral (if emergency/full stomach) |
| 45-60 min before | IM midazolam 0.07 mg/kg + IM glycopyrrolate 0.2 mg |
| In induction room | IV ondansetron 4 mg + IV dexamethasone 8 mg |
8. Dry Socket (Alveolar Osteitis)
Definition:
Incidence: 3-4% of all extractions; 20-30% for mandibular third molar extractions
Predisposing Factors:
- Smoking (most important modifiable risk factor)
- Difficult/traumatic extraction
- Female sex + oral contraceptive pill use
- Pre-existing pericoronitis or periodontal infection
- Mandibular location (denser bone, poorer vascular supply)
- Poor oral hygiene
- Systemic: diabetes, immunosuppression
Pathogenesis:
Clinical Features:
- Onset: Day 2-3 post-extraction (diagnostic hallmark - normal post-extraction pain peaks and then recurs/worsens by day 2-3)
- Severe, throbbing, deep-seated pain radiating to the ear, temple, and eye
- Bare, grey/yellowish bone in the socket
- Fetid odor
- Minimal systemic signs (no fever, no lymphadenopathy)
- Pain poorly controlled by standard analgesics
Management:
| Step | Action |
|---|---|
| 1 | Gently irrigate socket with warm saline or 0.12% chlorhexidine |
| 2 | Dry socket dressing: Alvogyl (iodoform/eugenol/butamben) or BIPP gauze, changed every 2-3 days |
| 3 | Oral analgesics: NSAIDs (ibuprofen 400 mg TDS) + paracetamol |
| 4 | Patient instructions: no smoking, soft diet, gentle oral hygiene |
| 5 | Antibiotics only if systemic signs of infection develop |
| 6 | Monitor: healing by secondary intention over 2-4 weeks |
9. Pleomorphic Adenoma
Definition:
Epidemiology:
- Most common salivary gland tumor overall (~60% of all salivary gland tumors)
- 60-80% of parotid gland tumors are pleomorphic adenoma
- Peak incidence: 4th-6th decade
- Slight female predominance
- Most common site: Superficial lobe of the parotid gland (80%); also submandibular, minor salivary glands (palate most common intraoral site)
Etiopathogenesis:
- Origin: Myoepithelial cells or ductal reserve (stem) cells
- Associated chromosomal rearrangements: overexpression of PLAG1 transcription factor (t(3;8) translocation) and HMGA2 gene mutations
- Radiation exposure increases risk
Gross Pathology:
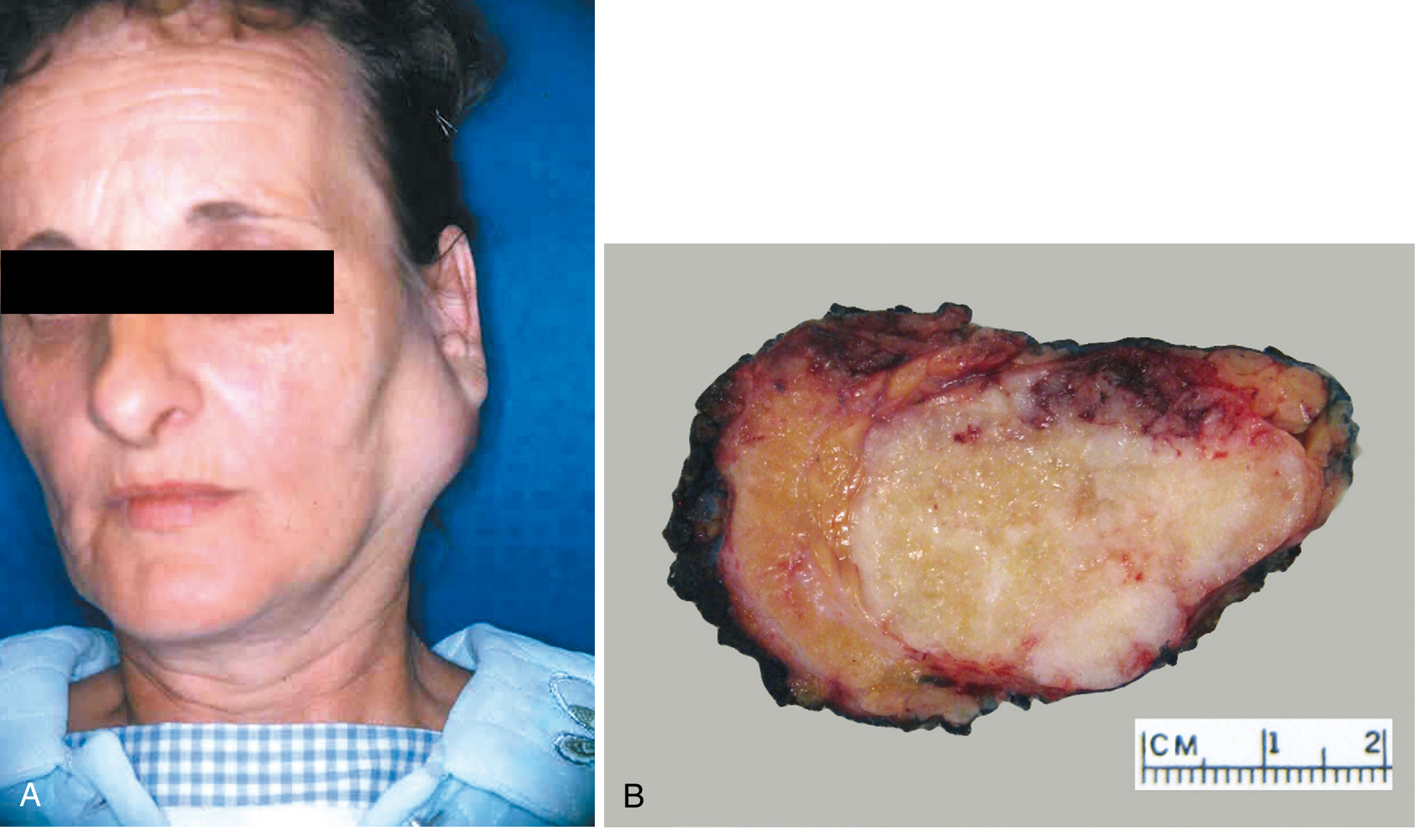
- Well-circumscribed, bosselated (lobulated) mass
- Usually <6 cm
- Cut surface: Gray-white with areas of myxoid (blue) and cartilaginous (chondroid) tissue
- Capsule: Present but incomplete especially in palatal tumors - capsular protrusions extend into surrounding gland → recurrence if enucleated
Histopathology (Morphology):
- Epithelial/ductal elements: Cuboidal/columnar cells forming ducts, tubules, cysts
- Myoepithelial elements: Small angular cells with dark nuclei; may form sheets, strands
- Mesenchymal/stromal elements: Chondromyxoid matrix - mucoid, hyaline, cartilaginous tissue; rarely bone
- No mitoses, no nuclear atypia in benign tumors
- No true nuclear pleomorphism (the name "pleomorphic" refers to histomorphic diversity, not nuclear pleomorphism)
Clinical Features:
- Painless, slow-growing, firm, mobile mass in the parotid region (pre- or infraauricular)
- Present for months to years before diagnosis
- Smooth or lobulated surface
- No skin fixation, no facial nerve palsy (if present, suspect malignancy)
- Usually unilateral
Investigations:
- FNAC (Fine needle aspiration cytology): First-line investigation; accuracy ~85-95%; confirms benign nature prior to surgery
- MRI: Gold standard imaging; well-defined, heterogeneous, T2-hyperintense mass
- Ultrasound: Useful for superficial parotid; guides FNAC
Management:
- Superficial parotidectomy (removal of the superficial lobe with facial nerve preservation) - treatment of choice for parotid pleomorphic adenoma
- Wide local excision with a cuff of normal tissue for other sites (submandibular, minor glands)
- NOT enucleation - recurrence rate after enucleation approaches 25% due to capsular irregularity and tumor protrusions
Complications of Surgery:
- Facial nerve palsy (temporary or permanent) - key risk in parotidectomy
- Frey's syndrome (auriculotemporal nerve syndrome) - gustatory sweating; occurs in 30-50%; due to aberrant reinnervation of sweat glands by secretomotor fibers
- Hematoma, wound infection, sialocele, salivary fistula
Malignant Transformation:
- ~2-4% of pleomorphic adenomas undergo malignant transformation if untreated for >15 years → Carcinoma ex pleomorphic adenoma
- Risk increases with long duration and recurrence
- Recurrence rate after superficial parotidectomy: ~4%
10. Ludwig's Angina
Definition:
Etiology:
- Odontogenic origin (85-90%): Most commonly periapical infection of mandibular second or third molar (apices below the mylohyoid line → spread to submandibular space)
- Other sources: salivary gland calculi/sialadenitis, mandibular fractures, oral lacerations, floor of mouth trauma
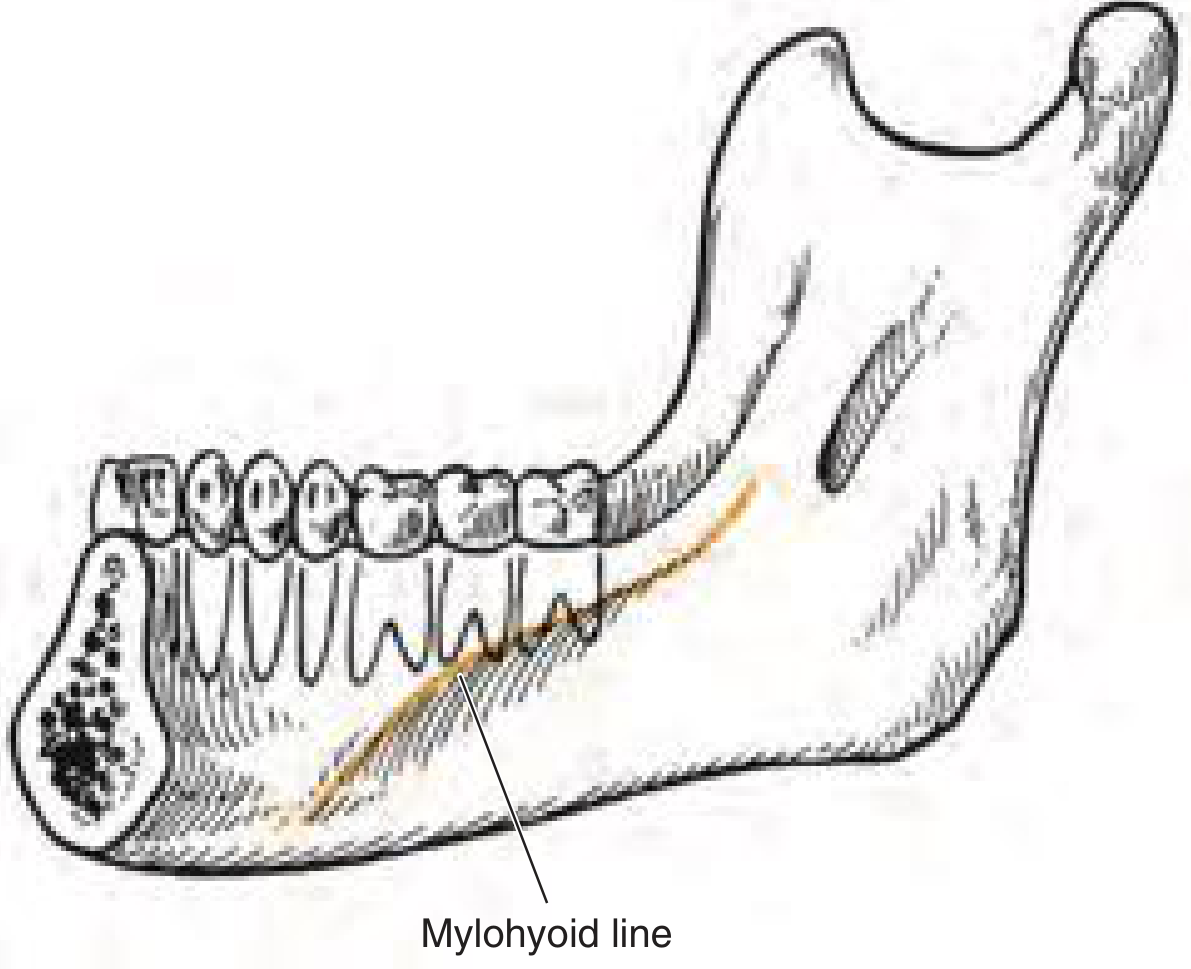
- Premolars + 1st molar apices → ABOVE mylohyoid → sublingual space
- 2nd + 3rd molar apices → BELOW mylohyoid → submandibular space
Causative Organisms:
- Polymicrobial (mixed): alpha-hemolytic streptococci (Streptococcus viridans) + anaerobes (Fusobacterium, Peptostreptococcus, Bacteroides)
- Streptococcus anginosus (S. milleri group) produces enzymes that facilitate fascial plane spread
Pathophysiology:
Clinical Features:
| Feature | Description |
|---|---|
| Brawny induration | Pathognomonic: hard, "woody," non-pitting edema of the floor of mouth and submandibular region |
| Bilateral submandibular swelling | "Bull neck" appearance; tense, tender swelling bilateral to the hyoid |
| Tongue elevation | Tongue displaced superiorly/posteriorly; may obstruct the airway |
| Trismus | Limited mouth opening |
| Dysphagia/Odynophagia | Difficulty/pain on swallowing |
| Drooling | Cannot swallow secretions |
| Dysphonia | "Hot potato" muffled voice |
| Dyspnea/Stridor | Impending airway obstruction (EMERGENCY) |
| Systemic signs | Fever, tachycardia, tachypnea; sepsis may develop |
Investigations:
- CT scan with contrast (axial + coronal): Delineates extent of infection, identifies abscess collections, evaluates airway - but patient may not tolerate lying supine
- Blood: CBC (leukocytosis), CRP, ESR elevated; blood cultures if septic
- OPG/dental X-rays: Identify causative tooth
- Chest X-ray: Exclude pneumonia/mediastinitis
Management:
Priority 1: AIRWAY MANAGEMENT (most critical)
| Airway option | When used |
|---|---|
| Awake fiberoptic nasotracheal intubation | Method of choice in early/moderate stages while airway still visible |
| Blind nasotracheal intubation | Not recommended |
| Elective tracheostomy | When intubation anticipated to be difficult or prolonged ventilation expected |
| Emergency cricothyrotomy | Last resort when cannot intubate or oxygenate |
Priority 2: IV ANTIBIOTICS (high-dose, broad-spectrum)
- First-line: Penicillin G (or amoxicillin-clavulanate) + Metronidazole (or clindamycin)
- Alternatives: Piperacillin-tazobactam; carbapenems (meropenem) in severe/resistant cases
- Continue for 10-14 days; switch to oral once improving
Priority 3: SURGICAL DRAINAGE
- Indicated when:
- CT shows discrete abscess collection
- Fluctuance on examination
- No clinical improvement after 24-48 hours of antibiotics
- Extraoral approach (preferred): Bilateral neck incisions through skin, platysma, investing fascia; blunt finger/clamp dissection through all three spaces; drains placed
- Submandibular incision placed 2 cm below and parallel to lower border of mandible
- Intraoral approach: Rarely adequate alone; used adjunctively
- Tooth extraction: Causative tooth extracted once infection controlled (or during drainage if feasible)
Priority 4: SUPPORTIVE CARE
- Steroids: Dexamethasone IV (to reduce edema and facilitate extubation)
- IV fluids, nutritional support (NG tube feeding if prolonged)
- ICU admission for monitoring
Complications / Spread of Infection:
- Descending necrotizing mediastinitis (most feared): Spread via retropharyngeal space (71%) or carotid sheath (21%) → thorax; 40% mortality even with treatment
- Parapharyngeal abscess
- Retropharyngeal abscess
- Lemierre syndrome (septic thrombophlebitis of internal jugular vein)
- Cavernous sinus thrombosis
- Aspiration pneumonia
- Septicemia and multi-organ failure
- Asphyxia
Prognosis:
- Mortality in pre-antibiotic era: 50-60%
- With modern antibiotics + early surgical intervention: Mortality <5%
- Death most commonly from airway obstruction and mediastinitis
Quick Reference Summary
| Topic | Single Key Fact |
|---|---|
| Pell & Gregory | Class (I/II/III) = ramus space; Position (A/B/C) = depth of impaction |
| PSAN Block | Needle upward + inward + backward at upper 2nd molar; 15-25 mm; risk = pterygoid plexus hematoma |
| Tracheostomy | Between 2nd-4th tracheal rings; never above 1st ring; Bjork flap for safety |
| Marsupialization | Partsch I; window + suture lining to oral mucosa; reduces cyst by eliminating osmotic pressure |
| TNM (8th Ed.) | DOI (depth of invasion) added to oral cavity T staging; ENE added to N staging |
| Gillies Approach | Temporal hairline incision; plane between deep temporal fascia and muscle; Rowe elevator |
| Premedication | Anticholinergic + benzodiazepine + opioid + antiemetic + antacid combination |
| Dry Socket | Day 2-3; bare bone; fibrinolysis; Alvogyl dressing; NOT primary infection |
| Pleomorphic Adenoma | Most common salivary tumor; chondromyxoid stroma; superficial parotidectomy; Frey's syndrome |
| Ludwig's Angina | Bilateral 3-space cellulitis; brawny induration; airway = #1 priority; IV Pen + Metro + drainage |
Antibiotic prophylaxis for infective endocarditis. 2. Marsupialization. 3. TNM classification. 4. Methods of fixation of jaw fractures. 5. Etiology, clinical features and management of Pterygomandibular space infection. 6. Composition of local anesthesia. 7. Hyperbaric oxygen therapy. 8. Oral manifestations of HIV. 9. Bilateral Sagittal Split Osteotomy. 10. What are the types of Biopsy? Add a note on FNAC. Give 5 mark answer
antibiotic prophylaxis infective endocarditis dental 2021 AHA guidelines amoxicillin high risk conditions
bilateral sagittal split osteotomy BSSO Obwegeser Dal Pont steps procedure indications oral surgery FNAC biopsy types oral surgery
pterygomandibular space infection etiology clinical features management drainage oral surgery composition dental local anesthetic cartridge
types of biopsy oral surgery incisional excisional punch trephine FNAC technique cytology
methods fixation jaw fractures IMF arch bars miniplate ORIF transosseous wiring oral surgery hyperbaric oxygen therapy mechanism indications HBO dental
Oral Surgery - Short Notes (10 × 5 Marks)
1. Antibiotic Prophylaxis for Infective Endocarditis
Background:
Cardiac Conditions Requiring Prophylaxis (HIGH-RISK only):
- Prosthetic cardiac valve (mechanical or bioprosthetic)
- Previous infective endocarditis
- Congenital heart disease (CHD) - only:
- Unrepaired cyanotic CHD (including palliative shunts/conduits)
- Completely repaired CHD with prosthetic material (within the first 6 months post-repair)
- Repaired CHD with residual defects at or adjacent to a prosthetic patch
- Cardiac transplant recipients who develop cardiac valvulopathy
NOT indicated for: Mitral valve prolapse, bicuspid aortic valve, rheumatic heart disease, acquired valvular dysfunction, CABG, VSD/ASD (repaired without residual shunt), hypertrophic cardiomyopathy
Dental Procedures Requiring Prophylaxis (in HIGH-RISK patients):
- Extractions, surgical procedures
- Scaling, root planing, subgingival curettage
- Endodontic (root canal) procedures - beyond the apex
- Replantation of avulsed teeth
- Placement of orthodontic bands (NOT brackets)
Procedures NOT Requiring Prophylaxis (even in high-risk patients):
- Dental radiographs
- Local anesthetic injections through non-infected tissue
- Adjustment of orthodontic appliances
- Placement of removable prostheses
- Shedding of deciduous teeth
- Bleeding from trauma to lips/mucosa (incidental)
- GI, GU procedures (GI/GU prophylaxis not recommended by 2021 AHA)
Antibiotic Regimens (AHA 2007/2021):
| Situation | Drug | Dose (Adult) | Timing |
|---|---|---|---|
| Standard - oral | Amoxicillin | 2 g oral | 30-60 min before |
| Unable to take oral | Ampicillin 2 g OR Cefazolin/Ceftriaxone 1 g | IM/IV | 30-60 min before |
| Penicillin allergy - oral | Cephalexin 2 g, OR Azithromycin/Clarithromycin 500 mg, OR Doxycycline 100 mg | oral | 30-60 min before |
| Pen allergy - cannot take oral | Cefazolin 1 g OR Ceftriaxone 1 g | IM/IV | 30-60 min before |
Note (2021 update): Clindamycin is no longer recommended as an alternative (risk of C. difficile infection exceeds benefit). If patient is already on amoxicillin for other reasons, use an antibiotic from a different class (e.g., azithromycin).
Pediatric Doses:
- Amoxicillin: 50 mg/kg oral
- Azithromycin: 15 mg/kg oral (max 500 mg)
2. Marsupialization
Definition:
Indications:
- Large cysts where enucleation risks mandibular fracture
- Proximity to vital structures (IAN, vital teeth roots, antrum floor)
- Dentigerous cysts - allows eruption of associated impacted tooth (especially in children)
- OKC (keratocyst) - to reduce size before definitive enucleation
- Elderly/medically compromised patients (less invasive)
- Infected cysts requiring drainage
Steps:
- Local/general anesthesia
- Excise a wide window of bone and cyst lining (≥2 cm) over the most accessible part - send specimen for histopathology
- Remove necrotic contents; irrigate with saline
- Suture the cyst lining circumferentially to the surrounding oral mucosa using resorbable sutures - creating a continuous epithelial-lined pouch
- Place an obturator/pack to maintain the window during healing
- Patient instructed to irrigate with chlorhexidine daily
- Serial OPGs at 3-6 month intervals to monitor regression
Advantages:
- Simple, less trauma
- Preserves vital structures and adjacent teeth
- Can allow tooth eruption
- Reduces size prior to definitive surgery (Waldron's technique = marsupialization + delayed enucleation)
Disadvantages:
- Prolonged treatment; needs patient compliance
- Incomplete histological assessment of entire lining
- Risk of residual lining transformation (especially OKC)
3. TNM Classification
AJCC/UICC 8th Edition (2018) - Oral Cavity Cancer
T Classification:
| T1 | ≤2 cm AND DOI ≤5 mm |
| T2 | ≤2 cm with DOI >5-10 mm, OR >2-4 cm with DOI ≤10 mm |
| T3 | >4 cm, OR any tumor with DOI >10 mm |
| T4a | Invades cortical bone, maxillary sinus, or skin of face (moderately advanced) |
| T4b | Invades masticator space, pterygoid plates, skull base, or encases ICA (very advanced) |
N Classification (Clinical):
| N0 | No regional node metastasis |
| N1 | Single ipsilateral node ≤3 cm, ENE(-) |
| N2a/b/c | Single ipsilateral >3 cm or multiple ipsilateral or contralateral, none >6 cm, ENE(-) |
| N3a | Any node >6 cm, ENE(-) |
| N3b | Any node with clinically overt ENE(+) |
M Classification:
- M0: No distant metastasis | M1: Distant metastasis
Stage Groups:
| Stage | T, N, M |
|---|---|
| I | T1, N0, M0 |
| II | T2, N0, M0 |
| III | T3, N0 or T1-3, N1, M0 |
| IVA | T4a or N2 (any T) |
| IVB | T4b or N3 (any T) |
| IVC | Any T, Any N, M1 |
4. Methods of Fixation of Jaw Fractures
A. Closed Reduction Methods (Conservative)
| Method | Description |
|---|---|
| Direct Interdental Wiring (Gilmer's wiring) | Wire looped around pairs of opposing teeth and twisted together bilaterally; simple but limited |
| Eyelet wiring (Ivy loop) | Prefabricated loops wired to individual teeth; loops are then connected by intermaxillary wires |
| Erich's Arch Bar | Most commonly used; malleable stainless steel bar with hooks wired to all teeth; hooks allow rubber bands or wires for IMF; versatile |
| Cap splints | Cast metal caps cemented over multiple teeth; used in children or when few teeth remain |
| Gunning splints | Modified complete dentures; used for edentulous mandible; held by circumandibular and piriform rim wires |
| IMF screws | Self-tapping titanium screws placed into alveolar bone between tooth roots; quick, comfortable alternative to arch bars |
- Non-displaced favorable fractures
- Condylar fractures (most)
- Greenstick fractures in children
- Grossly comminuted fractures (where ORIF impractical)
- Epilepsy (seizure risk - airway compromise)
- Psychiatric/uncooperative patients
- Pulmonary/respiratory compromise
- Alcoholism/vomiting tendency
- GI disorders with vomiting risk
B. Open Reduction and Internal Fixation (ORIF)
- Wires passed through drill holes in bone fragments and twisted together
- Non-rigid; requires supplementary IMF
- Used as adjunct, especially at inferior border
- Figure-of-8 wiring for added strength
- Standard of care for most displaced mandibular fractures
- 2.0 mm titanium miniplates with monocortical screws placed at the "tension zone" (superior border / Champy's lines of osteosynthesis)
- Champy's ideal lines of osteosynthesis (1978): Defined tension trajectories where a single miniplate provides adequate fixation - above the mental foramen, below the tooth roots, along the external oblique ridge for angle fractures
- Rigid fixation allows early mobilization without IMF
- For severely comminuted fractures, pathological fractures, infected/avascular bone
- Load-bearing fixation; may be used without bone contact
- Single large screw perpendicular to fracture compresses fragments together
- Used for parasymphysis, body fractures; excellent for oblique/long fractures
- Percutaneous pins inserted into bone fragments and held by external connecting bars
- Used for infected, comminuted fractures or when intraoral access not possible
- Wire passes under the mandible through the skin and holds a Gunning splint or denture in place
- For complex mid-face fractures; allows traction and suspension from a halo frame attached to the skull
5. Pterygomandibular Space Infection
Definition:
Anatomy / Boundaries:
| Boundary | Structure |
|---|---|
| Lateral | Medial surface of the mandibular ramus |
| Medial | Lateral surface of the medial pterygoid muscle |
| Anterior | Pterygomandibular raphe (joining buccinator + superior pharyngeal constrictor) |
| Posterior | Deep part of the parotid gland |
| Superior | Lateral pterygoid muscle |
Contents:
- Inferior alveolar nerve and artery/vein
- Lingual nerve
- Long buccal nerve
- Nerve to mylohyoid
- Sphenomandibular ligament
- Loose areolar connective tissue
Etiology (Sources of Infection):
- Mandibular third molar - pericoronitis, periapical abscess (most common)
- Needle-track infection from contaminated IAN block injection
- Infected fracture of the mandibular angle
- Spread from adjacent spaces (superficial temporal, infratemporal)
- Second molar periapical infection
Clinical Features:
| Feature | Detail |
|---|---|
| Trismus | Hallmark - severe limitation of mouth opening; due to medial pterygoid spasm |
| No/minimal extraoral swelling | Key diagnostic feature: "trismus without swelling" |
| Intraoral swelling | Swelling near the anterior tonsillar pillar; medial displacement of the soft palate |
| Dysphagia | Pain on swallowing; deviation of uvula to the opposite side |
| Pain | Deep-seated pain in the retromolar area, radiating to the ear |
| Fever and malaise | Systemic signs of infection |
Pathognomonic: Severe trismus with NO or minimal extraoral facial swelling
Investigations:
- OPG: Identify causative tooth (periapical pathology, partially erupted third molar)
- CT scan with contrast: Delineates extent, shows hypodense (pus-filled) collection within the pterygomandibular space
- CBC: Leukocytosis, elevated CRP
Management:
- IV amoxicillin-clavulanate 1.2 g TDS + metronidazole 500 mg TDS
- Alternatives: Penicillin + metronidazole; clindamycin if penicillin allergy
- Intraoral approach (preferred): Vertical incision medial and parallel to the pterygomandibular raphe (lateral to the raphe, medial to the mandibular ramus); blunt dissection with haemostat directed posteriorly and medially into the space; drain placed
- Extraoral (submandibular) approach: 2 cm below the lower border of the mandible; indicated if intraoral access inadequate or if combined with submandibular drainage
- Extraction of the causative tooth (third molar) once acute inflammation subsides, OR during drainage if accessible
- Drainage of abscess is the priority; tooth removal at same sitting if possible
- Analgesics (NSAIDs + paracetamol), hydration, soft diet
- Warm saline rinses; chlorhexidine mouthwash
- Spread to parapharyngeal, retropharyngeal, infratemporal spaces
- Ludwig's angina (if bilateral spread)
- Descending necrotizing mediastinitis
- Airway compromise
6. Composition of Local Anesthesia (Dental Cartridge)
Standard Composition of a 1.8 mL Dental Cartridge (e.g., 2% Lidocaine with 1:100,000 Epinephrine):
| Component | Concentration | Role |
|---|---|---|
| Local anesthetic agent (e.g., Lidocaine) | 2% (20 mg/mL; 36 mg/cartridge) | Primary anesthetic - blocks voltage-gated Na+ channels, prevents nerve depolarization |
| Vasoconstrictor (e.g., Epinephrine/Adrenaline) | 1:100,000 (10 mcg/mL; 18 mcg/cartridge) | Reduces blood flow → prolongs duration, reduces systemic absorption (improves depth of anesthesia), reduces bleeding |
| Antioxidant/Reducing agent (Sodium metabisulfite / Sodium bisulfite) | 0.5 mg/mL | Prevents oxidation of epinephrine (preserves vasoconstrictor efficacy) |
| Preservative (Methylparaben) | ≤1 mg/mL | Prevents microbial growth (bacteriostatic) - NOTE: excluded from single-use cartridges |
| Tonicity agent (Sodium chloride) | Variable | Adjusts osmolarity of solution to near physiological (isotonic ~280 mOsm/L) |
| Vehicle (Sterile water for injection) | q.s. | Solvent/diluent |
| pH adjustment (Sodium hydroxide) | Trace | Adjusts pH to ~4.5-6.0 (acidic pH stabilizes epinephrine and methylparaben) |
Other Common Dental Local Anesthetics and Their Concentrations:
| Agent | Concentration | Vasoconstrictor | Notes |
|---|---|---|---|
| Lidocaine | 2% | 1:100,000 or 1:80,000 epinephrine | Most widely used; amide class |
| Articaine | 4% | 1:100,000 or 1:200,000 epinephrine | Superior bone penetration; unique - contains both ester and amide groups |
| Mepivacaine | 2% (with vasoconstrictor) or 3% (plain) | Levonordefrin OR plain | Longer duration plain; useful in CV disease |
| Bupivacaine | 0.5% | 1:200,000 epinephrine | Longest duration (6-8 hrs); excellent for post-op pain control |
| Prilocaine | 4% | 1:200,000 epinephrine OR plain | Lowest systemic toxicity of amides; risk of methemoglobinemia |
Mechanism of Action:
- Un-ionized (free base) form crosses the nerve membrane
- Inside the nerve (lower pH), the drug re-ionizes to the cationic form
- The cationic form blocks the voltage-gated Na+ channel from the intracellular side
- Result: No depolarization → no impulse conduction → anesthesia
Maximum Safe Doses (Adult):
- Lidocaine with epinephrine: 7 mg/kg (maximum 500 mg)
- Lidocaine without epinephrine: 4.5 mg/kg (maximum 300 mg)
- Articaine with epinephrine: 7 mg/kg
7. Hyperbaric Oxygen Therapy (HBO)
Definition:
Physiological Basis:
- At 1 ATA (sea level), oxygen in plasma = ~0.3 mL/dL (most O2 carried by hemoglobin)
- At 2.4 ATA with 100% O2: plasma-dissolved O2 rises to ~5-6 mL/dL - sufficient to sustain tissues without hemoglobin
- This supersaturates hypoxic/necrotic tissues with oxygen, which is essential for:
- Collagen synthesis by fibroblasts (requires O2)
- Angiogenesis (promotes VEGF and new vessel formation)
- Bactericidal activity (restores oxidative burst in leukocytes; directly toxic to anaerobes)
- Reduction of tissue edema (vasoconstriction from hyperoxygenation)
- Enhancement of antibiotic activity (especially aminoglycosides)
- Osteogenesis (stimulates osteoblast activity)
Indications (Tintinalli's Table 21-2):
- Arterial gas embolism
- Carbon monoxide poisoning
- Decompression sickness
- Clostridial myonecrosis (gas gangrene)
- Necrotizing soft tissue infections
- Osteoradionecrosis (ORN) - Most important dental indication; HBO promotes angiogenesis in irradiated avascular bone; standard protocol: 20 pre-op + 10 post-op sessions (Marx protocol)
- Refractory chronic osteomyelitis of the jaws
- Medication-related osteonecrosis of the jaw (MRONJ) - adjunctive
- Compromised wound healing in irradiated tissue (e.g., pre/post dental implant surgery in irradiated jaws)
- Soft tissue radionecrosis
- Compromised flaps and grafts - improves viability
Standard Protocol:
- Pressure: 2.0-2.5 ATA (most commonly 2.4 ATA)
- Duration per session: 90-120 minutes
- Frequency: Once daily, 5 days/week
- Total sessions (ORN): 30 sessions (20 pre-op + 10 post-op) = Marx protocol
Complications of HBO:
- Barotrauma - ear (most common; tympanic membrane rupture), sinus, lung (pneumothorax)
- Oxygen toxicity: CNS (seizures with >3 ATA); pulmonary (>24 hrs continuous exposure)
- Claustrophobia (mono-place chambers)
- Fire risk (pure O2 environment - strict no-spark protocols)
- Myopia (reversible after cessation)
- Air embolism (rare)
Contraindications:
- Absolute: Untreated pneumothorax, concurrent bleomycin/cisplatin therapy (pulmonary toxicity), optic neuritis
- Relative: Pregnancy, emphysema, seizure disorder, congenital spherocytosis, claustrophobia
8. Oral Manifestations of HIV
Classification (EEC Classification - European Economic Community):
- Oral candidiasis (most common - 90% of HIV patients)
- Hairy leukoplakia
- HIV-associated periodontal disease
- Kaposi's sarcoma
- Non-Hodgkin's lymphoma
- Atypical ulcerations, thrombocytopenic purpura, salivary gland disease, viral infections (HSV, VZV, CMV, HPV)
- Bacterial infections, melanotic hyperpigmentation, drug reactions
Detailed Notes on Major Manifestations:
- Most common and often the first oral sign of immunosuppression
- CD4 count indicator: oral candidiasis signals CD4 <200 cells/μL; heralds transition to AIDS
- Types:
- Pseudomembranous (thrush): White, curd-like plaques; wipe off to leave red base; tongue, palate, buccal mucosa
- Erythematous (atrophic): Red, flat patches; often on dorsal tongue (loss of filiform papillae) and palate
- Hyperplastic: White patches that do NOT wipe off; pre-malignant potential
- Angular cheilitis (perleche): Erythema and fissuring at commissures
- Treatment: Fluconazole 100-200 mg/day; topical clotrimazole/nystatin for mild cases
- Pathognomonic of HIV (extremely specific)
- Caused by Epstein-Barr virus (EBV) reactivation
- Appearance: Corrugated (hairy), white lesion on the lateral borders of the tongue (bilateral); cannot be wiped off
- Does not transform to malignancy
- Indicates CD4 <300 cells/μL; marker of disease progression
- Treatment: Usually none required; resolves with HAART; acyclovir if symptomatic
- Most common AIDS-related malignancy
- Caused by Human Herpesvirus-8 (HHV-8)
- Oral lesions in 30% of KS patients; often the first manifestation
- Appearance: Flat or raised, reddish-blue to purple or brownish macules/nodules; hard palate (most common oral site), gingiva, tongue
- May ulcerate; causes pain, bleeding, secondary infection
- Linear gingival erythema (LGE): A band of erythema along the gingival margin extending ≥3 mm; not related to plaque levels; often with spontaneous bleeding
- Necrotizing ulcerative periodontitis (NUP): Rapid destruction of periodontal tissues; severe pain, bone loss, exposed necrotic bone; distinct from classic periodontitis
- Necrotizing stomatitis: Extension of necrosis beyond the periodontium to involve soft tissue and bone; very painful
- Severe, atypical, large, deep, and persistent aphthae occur in HIV (major aphthae/herpetiform pattern)
- Multiple ulcers, slow healing, recurrent
- Cause unknown; possibly immunological dysregulation
- Treatment: Topical/systemic corticosteroids; thalidomide in severe cases
- Most common lymphoma in HIV; diffuse large B-cell or Burkitt's lymphoma
- Oral manifestation: rapidly growing, ulcerated mass; most common on the palate and posterior gingiva
- Parotid enlargement (bilateral): Due to lymphoepithelial cysts or lymphocytic infiltration; associated with CD8+ lymphocyte infiltration
- Xerostomia: Common; due to salivary gland involvement + antiretroviral drug side effects
- Warts (squamous papilloma, condyloma acuminatum), focal epithelial hyperplasia (Heck's disease)
- Increased risk of HPV-related oral squamous cell carcinoma
- Cytomegalovirus co-infection (present in 90% of HIV cases) causes large, persistent, painful ulcerations
9. Bilateral Sagittal Split Osteotomy (BSSO)
Definition:
Indications:
- Mandibular prognathism (Class III skeletal - setback)
- Mandibular retrognathia (Class II skeletal - advancement)
- Facial asymmetry (rotation/asymmetric movement of mandible)
- Vertical excess/deficiency of the mandible
- Obstructive sleep apnea (mandibular advancement)
- Combined with LeFort I for bimaxillary surgery
Preoperative Requirements:
- Pre-surgical orthodontics (arch leveling, decompensation of dental compensations)
- Orthognathic model surgery and splint fabrication
- Removal of mandibular third molars at least 6-9 months before BSSO (to allow bone consolidation)
Surgical Technique (Dal Pont/Epker modification):
-
Anesthesia: General anesthesia via nasotracheal intubation
-
Incision: Anterior border of the ramus, extending into the buccal sulcus at the level of the first molar (bilateral)
-
Subperiosteal dissection: Medial and lateral surfaces of the ramus and body exposed
-
Medial cut (horizontal osteotomy):
- Sagittal saw or reciprocating saw is used
- A horizontal cut is made on the medial surface of the ramus, just above the mandibular foramen (above the lingula), extending posteriorly to the posterior border of the ramus
- Depth: through the medial cortex only (to avoid IAN injury)
-
Lateral cut (vertical osteotomy - Dal Pont modification):
- A vertical cut along the lateral surface of the mandibular body, extending from the second molar region to the inferior border, placed distal to the second molar tooth root
-
Connecting cut (inferior border):
- A connecting horizontal cut along the inferior border between the medial and lateral cuts
-
Splitting:
- Smith spreaders and Tessier osteotomes are carefully placed in the osteotomy lines
- The mandible is split sagittally along the medullary bone, separating the mandible into:
- Proximal segments (condyle + ramus - remain in the fossa)
- Distal/mobile segment (tooth-bearing body + chin - moved to desired position)
- The inferior alveolar nerve must be identified and protected within the distal segment
-
Repositioning:
- The distal segment is moved to the planned position (advancement, setback, or asymmetric movement)
- IMF established with the surgical occlusal splint to set the final occlusion
-
Fixation:
- Proximal and distal segments held together with 3 × 2.0 mm bicortical screws (inverted-L or linear arrangement) placed through the lateral cortex
- OR with a miniplate + monocortical screws
-
Wound closure: Resorbable sutures; IMF released; occlusion checked
Complications:
| Type | Complication |
|---|---|
| Intraoperative | Bad split (unfavorable fracture), IAN injury during splitting, hemorrhage (pterygoid plexus), condylar sag |
| Early postoperative | Swelling, trismus, IAN paresthesia, infection, plate exposure |
| Late | Relapse (most common long-term complication), TMJ dysfunction, permanent neurosensory deficit (IAN), skeletal relapse, condylar resorption |
Advantages over other mandibular osteotomies:
- Allows movement in all 3 planes (sagittal, vertical, transverse)
- Large bony contact area → good healing
- Intraoral approach (no visible scar)
- Rigid fixation allows early mobilization (no prolonged IMF)
10. Types of Biopsy with Note on FNAC
Definition:
Types of Biopsy:
- Only a representative portion of the lesion is removed (along with a small margin of normal tissue at the junction)
- Indicated when the lesion is large (>1 cm), or when complete removal would cause unacceptable morbidity, or when diagnosis is needed before definitive treatment
- Does NOT serve as treatment
- Most common type in oral surgery for large suspicious lesions
- The entire lesion is removed with a clear margin of normal tissue
- Serves as both diagnostic and therapeutic procedure
- Indicated for small lesions (≤1 cm) that appear benign
- Contraindicated for large lesions (incomplete removal risk) or suspected malignancy requiring margins planning
- A circular punch instrument (3-6 mm) is used to cut a cylindrical core of tissue
- Used for flat mucosal lesions, vesiculobullous diseases (pemphigus, pemphigoid), gingival biopsies
- Quick, minimal equipment required
- A hollow cylindrical drill (trephine) removes a core of bone or dense tissue
- Used for bony lesions (central jaw lesions) inaccessible to scalpel
- Provides histological core for diagnosis
- A stiff brush collects superficial cells from a lesion (OralCDx system)
- Transepithelial technique; samples full thickness of epithelium
- Screening tool; positive results must be confirmed with scalpel biopsy
- Fluid or tissue aspirated through a needle from a lesion
- Used to determine whether a lesion is cystic (aspiration of straw-colored fluid confirms cyst) or vascular (blood aspirated → suggests vascular lesion; NEVER excise without considering vascularity)
Note on FNAC (Fine Needle Aspiration Cytology):
- Salivary gland masses (parotid, submandibular)
- Cervical lymph node enlargement
- Soft tissue swellings of the face and neck
- Thyroid nodules
- Deep-seated lesions (infratemporal space, parapharyngeal)
- Pre-operative assessment of suspected malignancy before definitive surgery
- Lesion palpated and stabilized with non-dominant hand; skin cleaned with alcohol
- 22-25G needle attached to 10-20 mL syringe (with or without Cameco syringe holder)
- Needle inserted into the lesion; strong suction applied by withdrawing the plunger
- Needle moved back and forth within the lesion (jabbing motion) to dislodge cells
- Suction released before withdrawing the needle (to prevent aspiration of material into the syringe barrel)
- Needle removed; contents expelled on glass slides
- Air-dried smears: Stained with Giemsa/May-Grünwald (for hematological-type lesions)
- Wet-fixed smears: Fixed in 95% ethanol, stained with Papanicolaou (PAP) stain (for epithelial lesions)
- Smears examined by cytopathologist
- Minimally invasive; no general anesthesia required
- Quick result (same day or 24 hours)
- Low cost; repeatable
- No risk of tumor seeding along needle track (with fine needle)
- Excellent for cystic lesions and lymph nodes
- Guides further management
- Provides cytological diagnosis only (NO tissue architecture)
- Cannot distinguish carcinoma in situ from invasive carcinoma
- Cannot grade tumors reliably
- False negative rate 5-10% (depends on technique and cellularity)
- Sampling errors; inadequate specimens possible
- Cannot distinguish follicular adenoma from follicular carcinoma of thyroid
- Sensitivity ~85-90%, Specificity ~95%
- Confirms benign nature of pleomorphic adenoma prior to parotidectomy
- Identifies malignant features (atypia, necrosis, pleomorphism) suggesting carcinoma
Quick Summary Table
| Topic | Core Concept |
|---|---|
| IE Prophylaxis | Only for prosthetic valve, previous IE, cyanotic CHD, cardiac transplant + valvulopathy; Amoxicillin 2 g 1 hr before |
| Marsupialization | Partsch I; window + suture to oral mucosa; eliminates osmotic pressure; OPG monitoring |
| TNM 8th | DOI added to T staging; ENE added to N staging; T1 = ≤2 cm + DOI ≤5 mm |
| Jaw Fracture Fixation | IMF (arch bars, eyelet, cap splints) + ORIF (miniplate/Champy lines, transosseous wiring, lag screws) |
| Pterygomandibular Space | Trismus WITHOUT swelling; mandibular third molar cause; drain via vertical incision parallel to raphe |
| LA Composition | LA agent + vasoconstrictor + sodium metabisulfite + NaCl + water + pH adjuster |
| HBO | 100% O2 at 2-2.8 ATA; key for osteoradionecrosis (Marx: 20+10 sessions); angiogenesis + bactericidal |
| HIV Oral | Candidiasis (most common), hairy leukoplakia (EBV), KS (HHV-8), NUP, lymphoma, aphthae |
| BSSO | Trauner-Obwegeser 1955; sagittal split of ramus; IAN risk; 3 bicortical screws; prognathism/retrognathia |
| Biopsy/FNAC | Incisional/Excisional/Punch/Trephine/Brush; FNAC = cytology only; no tissue architecture; 22-25G needle |
Cardio pulmonary resuscitation. 2. Classification of suture materials. 3. Indications and surgical steps in alveoloplasty. 4. Caldwell luc procedure. 5. Management of primary haemorrhage during extraction of teeth. 6. Local and Systemic actions of Lidocaine. 7. WAR lines and it’s implications. 8. MARX protocol in the treatment of osteoradionecrosis (ORN). 9. Surgical options for prognathic mandible. 10. Plunging Ranula.
CPR AHA 2020 guidelines BLS steps compression rate ratio defibrillation oral surgery emergency Marx protocol osteoradionecrosis 20 sessions steps
Caldwell Luc operation steps indications complications antrostomy maxillary sinus oral surgery alveoloplasty types Dean Rowe simple conservative indications
WAR lines Harris lines growth arrest lines implications oral surgery suture material classification absorbable nonabsorbable synthetic natural examples
primary hemorrhage during tooth extraction management local hemostasis pressure pack gelatin sponge bone wax suture alveoloplasty types Dean simple Obwegeser
Marx protocol osteoradionecrosis HBOT 20 pre-operative 10 post-operative sessions surgical staging classification treatment 2004
Oral Surgery - Short Notes (10 × 5 Marks)
1. Cardiopulmonary Resuscitation (CPR)
Definition:
Chain of Survival (AHA 2020 - 6 Links):
- Recognition and activation of emergency response system
- Immediate high-quality CPR
- Rapid defibrillation
- Advanced resuscitation (drugs, airway)
- Post-cardiac arrest care
- Recovery (NEW - added in 2020 guidelines)
Sequence Change (AHA 2010 onwards): C-A-B (not A-B-C)
BASIC LIFE SUPPORT (BLS) - Step-by-Step:
- Ensure scene is safe; put on gloves
- Tap shoulders, shout "Are you okay?"
- No response + no normal breathing (gasping does NOT count as breathing)
- Simultaneously: Check pulse (carotid) - no longer than 10 seconds
- Call emergency services (or send someone); get AED
| Parameter | Standard |
|---|---|
| Position | Lower half of sternum; heel of hand |
| Depth | 5-6 cm (2-2.4 inches) for adults |
| Rate | 100-120 compressions/minute |
| Recoil | Allow full chest recoil after each compression |
| Interruptions | Minimize; no pause >10 seconds |
- Head-tilt chin-lift (no cervical spine injury suspected)
- Jaw thrust (if cervical spine injury suspected)
- Each breath: 1 second; watch for chest rise
- Ratio: 30 compressions : 2 breaths (single rescuer, all ages; 15:2 for children with 2 rescuers)
- Compression-only CPR acceptable if rescuer unable/unwilling to give breaths (hands-only CPR)
- Apply AED as soon as available
- Analyze rhythm; if shockable (VF/pulseless VT): deliver shock and immediately resume CPR
- Non-shockable (PEA/asystole): continue CPR, give epinephrine
ADVANCED CARDIAC LIFE SUPPORT (ACLS):
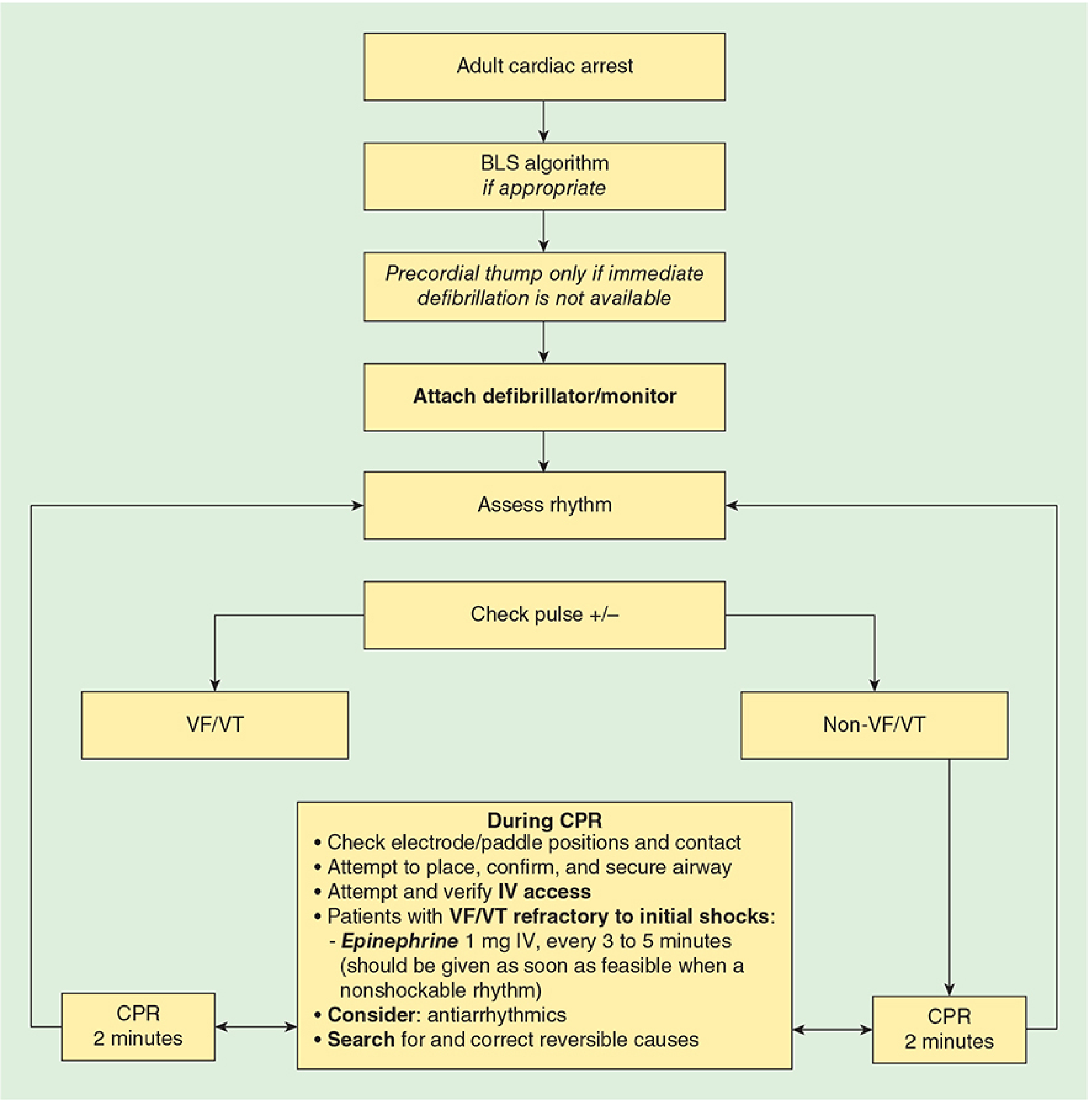
- Defibrillate immediately (biphasic: 120-200 J; monophasic: 360 J)
- After each shock: resume CPR immediately for 2 minutes before re-checking rhythm
- Epinephrine 1 mg IV every 3-5 min (after first/second shock)
- Amiodarone 300 mg IV bolus (shock-resistant VF/VT); or Lidocaine 1-1.5 mg/kg
- Continue CPR 2 min cycles
- Epinephrine 1 mg IV/IO ASAP, every 3-5 min
- Treat reversible causes
Reversible Causes - The "5 Hs and 5 Ts":
| 5 Hs | 5 Ts |
|---|---|
| Hypovolemia | Tension pneumothorax |
| Hypoxia | Tamponade (cardiac) |
| Hydrogen ion (acidosis) | Toxins |
| Hypo/Hyperkalemia | Thrombosis (coronary) |
| Hypothermia | Thrombosis (pulmonary) |
CPR in Dental Office:
- Patient reclined in dental chair is in the ideal CPR position
- Chair should be placed flat/horizontal; hard back support beneath patient
- Bite block removed; dentures removed
- Emergency kit must include: epinephrine, atropine, nitroglycerine, glucose, diphenhydramine, bronchodilator, oxygen
- Call for ambulance immediately
End Points of CPR:
- Return of Spontaneous Circulation (ROSC) - target
- EtCO2 <10 mmHg after 20 min in intubated patient = poor prognosis
- No PETco2 cutoff should be used in non-intubated patients to stop efforts
2. Classification of Suture Materials
Definition:
Classification:
A. By Absorbability (most important classification)
| Type | Material | Absorption Time | Notes |
|---|---|---|---|
| Plain catgut | Collagen from sheep submucosal intestine or bovine serosa | 7-10 days tensile strength lost; 70 days absorption | Most commonly used in oral surgery; causes significant tissue reaction |
| Chromic catgut | Catgut treated with chromic acid salts | 21-28 days tensile; 90 days absorption | Delayed absorption; less tissue reaction than plain; gold standard for intraoral closure |
| Polyglycolic acid (PGA) - Dexon | Synthetic polymer | 2-3 weeks tensile; 60-90 days | Less tissue reaction; braided |
| Polyglactin 910 - Vicryl | Polyglactin (glycolide + lactide) | 3-4 weeks tensile; 56-70 days | Most widely used synthetic absorbable; less reaction; braided |
| Poliglecaprone - Monocryl | Monofilament synthetic | 1-3 weeks; full absorption 90-120 days | Very low tissue reaction; smooth passage through tissue |
| Polydioxanone (PDS) | Monofilament synthetic | 4-6 weeks; 180 days absorption | Longest among absorbable; used for deeper tissues needing prolonged support |
| Material | Type | Notes |
|---|---|---|
| Silk | Natural, braided | Most commonly used non-absorbable in oral surgery; excellent handling; BUT significant tissue reaction; technically non-absorbable but degrades over years |
| Nylon (Ethilon) | Synthetic, monofilament/braided | Very low tissue reaction; poor knot security; monofilament form |
| Polypropylene (Prolene) | Synthetic monofilament | Lowest tissue reaction; used in vascular surgery; poor knot security |
| Polyester (Ethibond/Mersilene) | Synthetic, braided | Strong; good knot security; used in cardiac and tendon surgery |
| PTFE (Gore-Tex) | Synthetic monofilament | Inert; used in vascular and periodontal surgery |
| Stainless steel | Metallic monofilament | Maximum strength; used in sternal closure, orthopedic |
| Cotton/Linen | Natural, braided | Rarely used; significant reaction |
B. By Structure
| Type | Description | Advantages | Disadvantages |
|---|---|---|---|
| Monofilament | Single-strand | Low friction; less bacterial harbor; smooth passage | Poor handling; poor knot security; memory |
| Multifilament (braided) | Multiple intertwined strands | Good handling; good knot security | Higher capillarity (bacteria harbor); "wicking" effect |
| Pseudomonofilament | Braided core with smooth outer coating (e.g., coated Vicryl) | Good handling + lower capillarity | Intermediate |
C. By Origin (Raw Material)
| Natural | Synthetic |
|---|---|
| Catgut (collagen), silk, cotton, linen, stainless steel | Nylon, prolene, polyester, PGA, Vicryl, Monocryl, PDS, PTFE |
| More tissue reaction; less predictable | Less reaction; predictable absorption |
D. By Gauge (Size)
- Expressed as zeros: larger numbers = finer suture
- 0 (thickest) → 1-0 → 2-0 → 3-0 → 4-0 → 5-0 → 6-0 (finest)
- Intraoral oral surgery typically uses 3-0 or 4-0
- Skin closure: 4-0 or 5-0
- Vascular: 5-0 to 7-0
Ideal Suture Properties (mnemonic: STERILIZE):
- Strong (adequate tensile strength)
- Tissue reactive: minimal
- Easy to handle
- Resorbable (when appropriate)
- Infection resistant
- Low cost
- Inert (no allergic/toxic reaction)
- Zero memory/kink
- Easy knot security
Sutures in Oral Surgery Context:
- Silk 3-0: Traditional choice; good handling but causes granuloma; remove by day 7
- Chromic catgut 3-0: Best for intraoral closure; avoids need for suture removal
- Vicryl 3-0/4-0: Preferred modern choice; less reaction than catgut
- Nylon 4-0: For skin (extraoral) closure; remove at 5-7 days
3. Indications and Surgical Steps in Alveoloplasty
Definition:
Indications:
- Irregular alveolar ridge after multiple extractions - sharp bony spicules or undercuts
- Prominent mylohyoid ridge causing pain under denture
- Tori - mandibular torus or palatal torus interfering with denture seating
- Exostoses of the alveolar ridge
- Undercuts that prevent insertion/removal of dentures
- High labial frenum attachment - occasionally combined with frenectomy
- Genial tubercles - enlarged, interfering with lower complete denture
- Sharp alveolar crests after extraction
Types of Alveoloplasty:
- Performed at the time of extraction
- Small amounts of bone are removed/smoothed using bone file or rongeur
- No separate surgical procedure; flap may not be raised
- Minimal bone loss; suitable for single-tooth irregularities
- Indicated when significant vertical height reduction is also needed (reducing thick alveolar ridges)
- Removes the interseptal bone (crestal bone between tooth sockets)
- Brings the labial/buccal cortex inward to a more favorable ridge position
- Reduces ridge height while maintaining its width and base
- Specifically reduces a prominent or pendulous maxillary tuberosity
- Provides adequate interarch space for denture construction
- Bilateral protuberances of cortical bone on lingual surface of mandible (premolar region)
- Mucoperiosteal flap raised; bur/osteotome used to excise the torus; flap replaced
Surgical Steps for Simple Alveoloplasty (Most Common Exam Answer):
- Local anesthetic infiltration (buccal + lingual/palatal infiltration) OR regional block
- Crestal incision along the alveolar ridge
- Full-thickness mucoperiosteal flap elevated using a periosteal elevator, exposing the alveolar bone
- Irregular bony spicules and sharp edges identified
- Rongeur forceps used to nibble away excess bone
- Bone file used to smooth sharp edges and irregular surfaces
- Round bur (with adequate irrigation) used for precise reduction
- The goal is a smooth, rounded ridge without undercuts
- Thorough saline irrigation of the socket/wound to remove all bone chips and debris
- Palpate the ridge with a gloved finger
- Check for any remaining sharp edges or spicules
- Flap repositioned and sutured with interrupted or horizontal mattress sutures (chromic catgut 3-0 or Vicryl 3-0)
- Adequate flap tension-free closure essential
- Pressure pack placed
- Analgesics, antibiotics (if indicated)
- Review at 1 week for suture removal (if non-resorbable sutures used)
- Denture construction advised after 3-4 months (complete healing and resorption)
Complications:
- Excessive bone removal → thin, knife-edge ridge (opposite of intent)
- Nerve injury (mental nerve, IAN)
- Flap necrosis if flap design inadequate
- Dry socket / delayed healing
- Inadequate healing → poor prosthetic outcome
4. Caldwell-Luc Procedure (Radical Antrostomy)
Definition:
Indications:
- Removal of displaced root/tooth fragments from the maxillary antrum
- Removal of foreign bodies from the sinus
- Chronic maxillary sinusitis - removal of diseased sinus lining (antral membrane/polyps)
- Cysts and benign tumors within the maxillary sinus
- Closure of oroantral fistula via buccal advancement flap (Rehrmann flap)
- Blowout fracture of the orbital floor - for reduction of herniated orbital contents
- Removal of impacted maxillary canine or third molar when located within the sinus
- Management of antral hemorrhage (packing the sinus)
- Antral biopsy for suspected malignancy
- As an approach for pterygomaxillary space surgery
Surgical Steps:
- GA (preferred) OR LA with infraorbital block + posterior superior alveolar block + anterior superior alveolar block
- Nasal decongestant packs placed
- Vestibular incision (sublabial incision): Horizontal incision made in the mucobuccal fold from the canine region to the 2nd molar region, approximately 5 mm above the mucogingival junction
- Extends from the canine to the zygomatic buttress region
- Full-thickness mucoperiosteal flap elevated upward toward the infraorbital rim
- The infraorbital nerve (exits at infraorbital foramen, ~1 cm below the orbital rim at the level of the second premolar) must be identified and protected throughout
- A window is created in the anterolateral wall of the maxillary sinus in the canine fossa (above the root apices of the premolars)
- Initial entry with a bone gouge or round bur
- Window enlarged with rongeur forceps to approximately 2 × 3 cm
- The sinus mucosa (Schneiderian membrane) is visualized
- The sinus is explored under direct vision
- Diseased mucosa/polyps removed with curettes and rongeurs
- Root fragments/foreign bodies retrieved using suction, forceps, or with fibre-optic light probe assistance
- All loose material irrigated out
- A dependent drainage opening (inferior meatal antrostomy) may be created through the medial wall of the sinus into the inferior nasal meatus
- This is done to provide postoperative drainage and ventilation of the sinus
- A nasal antral window is created using a curved hemostat or trocar, connecting sinus to the nasal cavity
- Iodoform gauze pack placed to achieve hemostasis; removed via nasal antrostomy window 48-72 hrs later
- Mucoperiosteal flap returned to original position
- Closed with interrupted resorbable sutures (Vicryl or chromic catgut 3-0)
Post-operative Care:
- Prophylactic antibiotics (amoxicillin 500 mg TDS × 5 days)
- Nasal decongestants to facilitate drainage
- Patient instructed to avoid nose-blowing for 2 weeks
- No drinking through straws (creates negative pressure)
Complications:
| Intraoperative | Postoperative |
|---|---|
| Infraorbital nerve injury (paresthesia/anesthesia of cheek, upper lip) | Chronic sinusitis |
| Damage to tooth roots | Oroantral fistula |
| Entry into nasal cavity | Facial swelling/numbness (premaxillary fibrosis) |
| Excessive hemorrhage | Recurrent polyps |
| Orbital injury (if flap too aggressive superiorly) | Epiphora (lacrimal duct injury if nasal antrostomy too anterior) |
5. Management of Primary Hemorrhage During Extraction
Definition:
Causes of Primary Hemorrhage:
- Acute infection at the extraction site (hyperemia)
- Damage to larger vessels (greater palatine artery, mental artery, lingual artery)
- Fractured alveolar bone with torn periosteum
- Tearing of soft tissue flap
- Failure of blood clot formation (socket not compressed)
- Highly vascular granuloma or cyst in the socket
- Bleeding from cancellous bone (venous ooze)
- Anticoagulant therapy (warfarin, heparin, DOACs)
- Antiplatelet drugs (aspirin, clopidogrel)
- Haemophilia A or B (Factor VIII/IX deficiency)
- Von Willebrand disease
- Thrombocytopenia (ITP, chemotherapy)
- Liver disease (reduced clotting factor synthesis)
- Chronic renal failure
- Hereditary clotting disorders
Management:
Step 1 - Immediate Pressure:
- Ask patient to bite firmly on a moist gauze pack for 20-30 minutes
- This is the first and most important step - tamponade controls most extraoral bleeding
Step 2 - Examine and Identify Source:
- Aspirate blood from socket using suction
- Good light source; identify the bleeding point:
- Soft tissue bleeding (mucosal tears, gingival edges)
- Bone bleeding (cancellous bleeding from socket walls/base)
- Arterial bleeding (bright red, pulsatile)
Step 3 - Local Hemostatic Measures:
- Suturing: Place interrupted or figure-of-8 sutures across the socket; compress the gingival edges together
- Direct pressure with epinephrine-soaked gauze (1:1,000)
- Electrocautery - for visible bleeders
- Figure-of-8 suture over the socket - the most effective measure for intra-alveolar bleeding
- Resorbable hemostatic agents packed into the socket:
- Gelatin sponge (Gelfoam) - absorbs and acts as scaffold for clot
- Oxidized regenerated cellulose (Surgicel) - bactericidal; accelerates clotting
- Collagen sponge - activates platelet aggregation
- Calcium sulfate
- Bone wax - pressed into bleeding cancellous bone/marrow spaces (mechanical tamponade)
- Topical thrombin solution applied directly
- Tranexamic acid (antifibrinolytic) - soaked into gauze as local pack, OR as mouthwash
Step 4 - Further Measures (if above fail):
- Zinc oxide-eugenol pack (Alvogyl-type) placed in socket
- Electrosurgery - for arterial bleeders
- Ligation of named vessels (rare; for great palatine artery, lingual artery bleeding)
- Tamponade with iodoform gauze
Step 5 - Systemic Measures:
- Identify and reverse coagulopathy:
- Warfarin toxicity: Vitamin K, Fresh Frozen Plasma (FFP)
- Haemophilia A: Factor VIII concentrate
- Von Willebrand disease: Desmopressin (DDAVP) + Factor VIII
- Thrombocytopenia: Platelet transfusion (if <50,000/µL)
- IV access + fluid resuscitation if significant blood loss
Step 6 - Patient Instructions (Post-operative):
- Bite on gauze for 30 min
- Avoid rinsing for 24 hours
- Avoid hot liquids, alcohol, smoking for 48 hours
- Avoid nose-blowing and strenuous activity
- Soft diet
- Return if bleeding resumes
6. Local and Systemic Actions of Lidocaine
Lidocaine (Lignocaine):
LOCAL ACTIONS (as Local Anesthetic):
Mechanism:
- Lidocaine is a weak base (pKa = 7.9). At physiological pH, it exists in both ionized (BH+) and unionized (B) forms.
- The unionized (lipid-soluble) form crosses the nerve cell membrane via lipid bilayer diffusion
- Inside the axon (lower pH), re-ionization occurs to the cationic form (BH+)
- The cationic form binds to the intracellular aspect of voltage-gated Na+ channels, blocking them
- With Na+ channels blocked, the membrane cannot depolarize → no action potential generated → nerve impulse blocked
Order of Blockade (smallest to largest fibers first):
- Pain (C fibers + Aδ) → Temperature → Touch → Pressure → Proprioception → Motor (Aα largest - last)
- Clinically: analgesia before anesthesia before motor block
Local Effects on Nerve:
- Produces reversible conduction blockade
- No structural damage to nerve at therapeutic concentrations
- Onset: 2-5 min (fast for lidocaine; pKa close to physiological pH)
- Duration: 60-90 min (plain); 2-3 hours (with epinephrine 1:100,000)
- Vasoconstrictor (epinephrine) added to: prolong duration, reduce peak plasma levels, improve depth, reduce bleeding
SYSTEMIC ACTIONS:
A. Cardiovascular System Actions:
- Class IB antiarrhythmic: Blocks fast Na+ channels in cardiac myocytes
- Reduces automaticity (decreases spontaneous depolarization rate in His-Purkinje system)
- Shortens action potential duration and effective refractory period
- Used IV for: Ventricular tachycardia, ventricular fibrillation (when amiodarone is not available), ectopic ventricular beats
- No significant effect on normal myocardium at therapeutic doses
- Vasodilation: Peripheral vasodilation → hypotension
- Myocardial depression: Reduced contractility → reduced cardiac output
- Bradycardia → Heart block → Asystole
- Ventricular fibrillation (paradoxically, at very high doses)
- AV block
B. Central Nervous System Actions:
- Circumoral and tongue numbness and tingling (first sign)
- Light-headedness, dizziness
- Tinnitus, blurred vision
- Slurred speech, metallic taste
- Restlessness, anxiety
- Muscle twitching
- Seizures (excitatory CNS effects - first major toxic sign)
- CNS depression
- Unconsciousness
- Respiratory depression → Respiratory arrest
- Coma → Death (if untreated)
C. Other Systemic Actions:
- Respiratory: Bronchodilator effect at low doses (used to suppress cough reflex before intubation); respiratory depression at toxic doses
- Neuromuscular junction: Minimal effect at clinical doses; slight blockade at toxic doses
- Anticonvulsant: At subthreshold IV doses, has anticonvulsant property; paradoxically causes seizures at toxic levels
Maximum Safe Dose:
- With epinephrine: 7 mg/kg (max 500 mg in adult)
- Without epinephrine: 4.5 mg/kg (max 300 mg in adult)
Signs of Lidocaine Toxicity (In Order of Appearance):
- Circumoral numbness/tingling
- Metallic taste
- Tinnitus
- Visual disturbances
- Dizziness, confusion
- Muscle twitching
- Seizures (CNS excitation)
- CNS depression, respiratory arrest
- Cardiovascular collapse
Management of Toxicity:
- Stop injection; call for help
- ABC management
- Seizures: IV benzodiazepine (diazepam or midazolam)
- Cardiovascular collapse: IV Intralipid (lipid emulsion) 20% - binds and neutralizes lipid-soluble local anesthetic
- Supportive: oxygen, IV fluids, vasopressors if needed
7. WAR Lines and Their Implications
Background:
Discovery:
Formation:
Site of Occurrence:
- Metaphyses of long bones - distal radius, proximal tibia, distal femur (most common sites in radiology)
- Inferior border of the mandible (in the condylar region and body of the mandible)
- Maxillary sinus walls
Appearance on Radiograph:
- Dense transverse lines running perpendicular to the long axis of the bone
- Located at the metaphysis (in long bones) - the zone of previous growth plate activity
- Multiple lines may be present (one for each arrest episode)
- May appear single or multiple
Causes of WAR Lines:
- Systemic illness - typhoid, rickets, scurvy, tuberculosis
- Malnutrition - protein-energy malnutrition, vitamin deficiency
- Chemotherapy or radiation therapy
- Heavy metal poisoning - lead, bismuth
- Metabolic disorders - hypothyroidism, hypoparathyroidism
- Severe physiological stress - major trauma, surgery
- Normal growth spurts - can leave minor lines
Implications in Oral/Maxillofacial Surgery:
- Number, spacing, and location of WAR lines in the mandible and long bones can help estimate age at time of illness and current age
- Provides evidence of growth history and medical history from skeletal remains
- WAR lines in the condylar region may be mistaken for fracture lines on OPG - important differential diagnosis (WAR lines are smooth, regular, bilateral; fractures are irregular, sharp-edged, often unilateral)
- In orthognathic surgical planning, WAR lines in the condyle region indicate previous episodes of growth arrest, suggesting asymmetric or disturbed condylar growth
- May explain facial asymmetry or mandibular deformities
- Their presence indicates the patient had a significant systemic illness during growth years
- Number of lines = number of episodes of growth arrest
- Distance from the epiphysis correlates with age at occurrence
- When seen on a panoramic radiograph in the condylar process region, they represent past systemic stress events
- May indicate a growth period vulnerable to long-term effects of illness
- In lead poisoning, very dense WAR-like lines (lead lines/bismuth lines) appear at metaphyses - these indicate heavy metal deposition at zones of active bone formation
Differential Diagnosis of WAR Lines:
| Feature | WAR Lines | Fracture |
|---|---|---|
| Orientation | Horizontal (perpendicular to axis) | Oblique/irregular |
| Edges | Smooth, regular | Irregular, step |
| Bilateral | Usually bilateral | Usually unilateral |
| Location | Metaphysis | Any site of trauma |
| Continuity | Continuous across bone | Discontinuous |
8. Marx Protocol in Treatment of Osteoradionecrosis (ORN)
Osteoradionecrosis (ORN):
Pathophysiology (Marx, 1983):
- Hypoxia - reduced oxygen tension
- Hypovascularity - radiation-induced obliterative endarteritis
- Hypocellularity - loss of fibroblasts and osteoblasts
Risk Factors for ORN:
- Radiation dose >60 Gy
- Poor oral hygiene before/after radiotherapy
- Tooth extraction post-radiation (most common precipitant)
- Adjacent tumour location
- Mandible involvement (denser, less vascular than maxilla)
- Nutritional deficiency, smoking, alcohol
Marx Classification (Staging):
| Stage | Description |
|---|---|
| Stage I | Exposed bone; responds to HBO + minor debridement; ORN confined to alveolar process |
| Stage II | Stage I that fails to respond; requires more extensive sequestrectomy/debridement with primary closure |
| Stage III | Full-thickness involvement; involvement up to or through inferior border; may have pathological fracture, oro-cutaneous fistula; requires resection |
| Stage III-R | Stage III lesion after resection and bone graft reconstruction |
MARX PROTOCOL (HBO-Based Treatment):
- 100% oxygen at 2.4 ATA (atmospheres absolute)
- 90 minutes per session
- Once daily, 5 days/week
PROTOCOL FOR PREVENTION (Before Dental Procedures in Irradiated Jaw):
- Used BEFORE dental extractions or implant placement in irradiated jaws
- 20 sessions of HBO pre-operatively
- Procedure performed
- 10 sessions of HBO post-operatively
- Rationale: Pre-op HBO reverses vascular changes and restores vascular density to 75-85% of normal after 18-23 treatments
PROTOCOL FOR ESTABLISHED ORN TREATMENT:
- 30 sessions of HBO
- Reassess wound:
- If improved → 10 more HBO sessions (total 40) → conservative bony debridement → heal by secondary intention
- If no improvement → advance to Stage II
- 30 sessions of HBO
- Transoral sequestrectomy/debridement with primary mucosal closure
- Reassess wound:
- If heals → 10 more HBO sessions (total 40) → complete
- If dehisces → advance to Stage III
- 30 sessions of HBO
- Resection of mandible (marginal resection for superior border ORN; continuity resection/segmental resection for through-and-through ORN)
- Immediate or delayed bone graft reconstruction (autogenous iliac crest; or vascularized fibula free flap)
- 10 sessions of HBO post-operatively (Stage III-R = 30 pre + 10 post)
- After 10 weeks: 20 more sessions in preparation for bone graft
| Indication | Pre-op HBO | Surgery | Post-op HBO |
|---|---|---|---|
| Prevention (extraction in irradiated jaw) | 20 sessions | Procedure | 10 sessions |
| Stage I ORN | 30 sessions | Minor debridement | 10 sessions |
| Stage II ORN | 30 sessions | Sequestrectomy | 10 sessions |
| Stage III ORN | 30 sessions | Resection | 10 sessions + 20 pre-graft |
Mechanism of HBO in ORN Treatment:
- Drives angiogenesis (VEGF stimulation) - restores blood supply to ischemic bone
- Stimulates fibroblast proliferation - restores collagen synthesis
- Stimulates osteoblast activity - new bone formation
- Bactericidal - restores leukocyte oxidative killing ability (requires O2 for superoxide production)
- Reduces tissue edema via hyperoxic vasoconstriction
- Enhances antibiotic efficacy (aminoglycosides)
Limitations/Controversies:
- Expensive and not universally available
- Some evidence (e.g., DAHANCA-21 trial) questions superiority over surgery alone
- Time-consuming (30-40 daily sessions = 6-8 weeks)
- Contraindicated if untreated pneumothorax; bleomycin use
9. Surgical Options for Prognathic Mandible
Definition:
Assessment:
- Cephalometric analysis: ANB < 0° (negative); SNB > 80°; mandibular plane angle
- Clinical: Reverse overjet, concave facial profile, retrusive mid-face
- Pre-surgical orthodontic treatment mandatory to decompensate dental compensations
Surgical Options:
A. Intraoral Procedures
- Sagittal splitting of the mandibular ramus bilaterally
- Proximal segment (condyle + ramus) remains in glenoid fossa; distal segment (tooth-bearing) set back
- Fixation: 3 × bicortical positional screws per side OR miniplate
- Allows movement in all 3 planes; large bony contact → good healing
- Disadvantage: Risk of IAN injury (5-30% neurosensory disturbance)
- Vertical cut through the ramus from sigmoid notch to the inferior border, just posterior to the IAN foramen
- Proximal segment overlaps with distal segment (or separated) → mandibular setback
- Advantage: IAN NOT at risk (cut is posterior to IAN)
- Disadvantage: Requires post-op IMF (6 weeks); no rigid fixation possible from intraoral approach; less versatile (setback only; cannot advance)
- Surgical removal of a segment of bone from the body of the mandible (posterior to the mental foramen)
- Mandible shortened and closed on itself
- Now rarely used; leaves external scar if extraoral approach; risk to IAN and inferior border continuity
B. Extraoral Procedures
- Same cut as IVRO but through submandibular (Risdon) incision
- Direct visualization and rigid fixation possible
- Leaves a scar; rarely used if intraoral approach feasible
- Cut through the ramus obliquely from the sigmoid notch to posterior border of ramus
- Avoids the IAN entirely
- Extraoral approach; setback achievable
- Reserved for cases where prognathism is due to condylar hyperplasia (active growth)
- Removes the excess-growing condylar head
- Must confirm active condylar growth by bone scintigraphy before proceeding
- Condylectomy stops the growth disturbance
C. Genioplasty (Adjunctive):
- Sliding genioplasty adjusts chin position independently
- Used as an adjunct when chin protrusion remains after mandibular setback, OR when genioplasty alone can address a minor prognathism
- Not a standalone option for skeletal prognathism
D. Distraction Osteogenesis:
- Not typically used for prognathism correction; used for hypoplasia/advancement
- Exception: calvarial/midface distraction in syndromes
Comparison Table - BSSO vs IVRO:
| Feature | BSSO | IVRO |
|---|---|---|
| IAN risk | Yes (moderate) | Minimal |
| Movement | All 3 planes | Setback mainly |
| Fixation | Rigid (screws) | IMF required |
| Stability | Better (rigid fixation) | Fair (after IMF removal) |
| Occlusal control | Immediate | Post-IMF |
| Hospital stay | Shorter | Longer |
Pre-surgical Orthodontics:
- Mandatory before orthognathic surgery
- Decompensate dental compensations (Class III patients often have proclined lower incisors + retroclined upper incisors; orthodontics worsens the appearance temporarily by decompensating)
- Coordinate upper and lower arches on model surgery
- Total pre-surgical orthodontics: 12-18 months
10. Plunging Ranula
Definition:
- Simple ranula: Confined to the floor of the mouth (above the mylohyoid muscle); blue, translucent, dome-shaped swelling in the anterior floor of mouth
- Plunging (cervical) ranula: Mucous extravasate that penetrates through the mylohyoid muscle (through a natural dehiscence in the posterior mylohyoid or around the posterior free edge of the mylohyoid) and extends into the neck (submandibular region or further)
Pathogenesis:
- A natural dehiscence/defect in the posterior mylohyoid muscle (the most common mechanism)
- Around the posterior free edge of the mylohyoid
- Results in a dumbbell-shaped bilobed pseudocyst with an oral component (floor of mouth) and a cervical component (submandibular/submental)
Note: Plunging ranulas are pseudocysts (no true epithelial lining); they are lined by compressed connective tissue and granulation tissue.
Clinical Features:
- Bluish, translucent, fluctuant swelling in the floor of mouth (often small or absent in plunging ranula - may have resolved as contents herniated into neck)
- Lateral to the midline (sublingual gland is lateral)
- May push tongue superiorly and posteriorly → dysphagia, dysphonia
- Soft, non-tender, fluctuant swelling in the submandibular triangle (most common) or submental region
- May extend to the parapharyngeal space, retropharyngeal space, or even the mediastinum (rarely)
- Swelling may increase with meals (due to increased salivary secretion)
- Transilluminates if large enough
Investigations:
- Clinical examination (bimanual palpation confirms communication)
- MRI (investigation of choice): Best for delineating extent; shows dumbbell configuration; T2-bright signal (mucoid content); no enhancement of walls (differentiates from abscess)
- Ultrasound: Anechoic, homogeneous; identifies relationship to mylohyoid
- CT scan with contrast: For complex cases; identifies sinus/fistula
- FNA/Aspiration: Aspiration of viscous, straw-colored/clear fluid rich in amylase and salivary proteins - confirms diagnosis; NOT therapeutic
- Sialography: Not recommended (risks rupture and inflammation)
Differential Diagnosis:
| Diagnosis | Distinguishing Features |
|---|---|
| Cystic hygroma | Multicystic; more common in children; transilluminates |
| Thyroglossal cyst | Midline; moves with swallowing and tongue protrusion |
| Branchial cyst | Lateral neck; along anterior border of SCM |
| Submandibular sialadenitis | Painful; associated with meals; calculus may be seen |
| Lipoma | Non-fluctuant; dough-like; no FOM component |
| Lymphangioma | Multicystic; children |
Treatment:
- Simple aspiration: temporary relief; high recurrence rate (~100%)
- Sclerotherapy with OK-432 (Picibanil) or bleomycin: Injected into the pseudocyst; causes fibrosis and obliteration; good results reported especially in Japan; avoids surgery in simple cases
- Marsupialization: Only for simple ranulas; NOT recommended for plunging ranulas (very high recurrence rate >70%)
- Intraoral approach: Incision in the floor of the mouth over the sublingual region
- The ipsilateral sublingual gland is completely excised (source of mucus)
- The ranula fluid is simultaneously drained through the same intraoral incision
- The cervical component collapses and resolves on its own after source removal
- Recurrence rate: <5%
- Must identify and protect Wharton's duct (submandibular duct) throughout
- Intraoral sublingual gland excision + separate submandibular (Risdon) incision to drain the cervical pseudocyst
- Cervical drain placed; pressure dressing applied
- Used for:
- Large pseudocysts that cannot be fully drained intraorally
- Revision/recurrent cases
- Complete excision of pseudocyst wall not necessary (pseudocyst wall collapses after drainage)
Recurrence:
- Marsupialization alone: 60-90% recurrence
- Drainage without sublingual gland removal: ~50% recurrence
- Sublingual gland excision (intraoral): <5% recurrence
Complications of Surgery:
- Injury to Wharton's duct (submandibular duct) → submandibular sialadenitis, obstruction
- Injury to lingual nerve → altered taste, numbness of tongue
- Injury to hypoglossal nerve (extraoral approach)
- Wound infection, haematoma
- Recurrence (if gland not completely removed)
Quick Summary Table
| Topic | Key Exam Points |
|---|---|
| CPR | C-A-B sequence (2010); 30:2 ratio; depth 5-6 cm; rate 100-120/min; AHA 2020 added "Recovery" as 6th link in chain of survival |
| Sutures | Absorbable (catgut, Vicryl) vs Non-absorbable (silk, nylon); Natural vs Synthetic; Monofilament vs Multifilament |
| Alveoloplasty | Reshape ridge for dentures; Simple (Dean) vs Radical (intraseptal); flap - rongeur - file - closure |
| Caldwell-Luc | Canine fossa window; protect infraorbital nerve; root removal, chronic sinusitis, OAF closure |
| Primary Hemorrhage | Pressure pack first; figure-of-8 suture; hemostatic agents (Gelfoam, Surgicel); identify systemic cause |
| Lidocaine Actions | Local: Na+ channel block; order C → Aδ → motor; Systemic: CNS excitation then depression; antiarrhythmic (Class IB) |
| WAR Lines | Growth arrest lines at metaphysis; Harris 1933; bilateral transverse dense lines; forensic age estimation; DD from fracture |
| Marx Protocol | ORN = 3H (hypoxia/hypovascularity/hypocellularity); Prevention = 20+10; Treatment = 30+10 HBO sessions per stage; Stage I/II/III |
| Prognathic Mandible | BSSO (gold standard, all planes, IAN risk); IVRO (no IAN risk, setback only, needs IMF); Condylectomy (condylar hyperplasia) |
| Plunging Ranula | Sublingual gland; herniates through mylohyoid; MRI = investigation of choice; Rx = intraoral sublingual gland excision (<5% recurrence) |
1. Emergency drugs used in dental practice. 2. Carnoy’s solution. 3. Clinical features and surgical management of chronic osteomyelitis of the jaw. 4. Basic life support. 5. Landmarks and technique of Inferior alveolar block. 6. Partsch 2 procedure. 7. Genioplasty. 8. Local hemostatic agents. 9. Universal infection control precautions. 10. Anterior maxillary segmental osteotomy (AMO).
emergency drugs dental practice epinephrine nitroglycerin hydrocortisone glucagon doses indications kit
chronic osteomyelitis jaw clinical features sequestrum involucrum saucerization sequestrectomy management oral surgery Partsch 2 enucleation cyst procedure steps
anterior maxillary segmental osteotomy Wassmund Wunderer technique indications steps prognathism open bite genioplasty sliding horizontal osteotomy steps chin surgery
inferior alveolar nerve block technique landmarks pterygomandibular triangle coronoid notch insertion point depth 20-25mm aspiration oral surgery universal infection control precautions dental
Partsch II procedure cyst enucleation primary closure steps oral surgery local hemostatic agents bone wax gelatin sponge tranexamic acid thrombin fibrin sealant mechanism
Oral Surgery - Short Notes (10 × 5 Marks)
1. Emergency Drugs Used in Dental Practice
Essential (Mandatory) Emergency Drugs:
| Drug | Indication | Route/Dose (Adult) |
|---|---|---|
| Oxygen (100%) | Almost every emergency - hypoxia, syncope, angina, asthma, anaphylaxis | Inhalation via mask; 6-10 L/min |
| Epinephrine (Adrenaline) 1:1000 | Anaphylaxis (drug of choice); severe bronchospasm unresponsive to salbutamol | IM (anterolateral thigh/deltoid) 0.3-0.5 mg (0.3-0.5 mL); auto-injector (EpiPen) preferred |
| Nitroglycerin (Glyceryl trinitrate) | Angina pectoris (coronary artery spasm) | Sublingual tablet (0.4 mg) or spray; repeat every 3-5 min × 3 doses max |
| Aspirin | Suspected acute myocardial infarction (antiplatelet) | 300 mg chewed (soluble/dispersible) |
| Salbutamol (Albuterol) | Bronchospasm/acute asthma | MDI inhaler: 2 puffs; repeat as needed |
| Diphenhydramine (antihistamine - H1 blocker) | Mild-moderate allergic reactions (urticaria, angioedema) | 50 mg IM/IV OR 25 mg oral |
| Glucagon | Severe hypoglycaemia (patient unconscious; cannot take oral glucose) | 1 mg IM/subcutaneous; onset 10-15 min |
| Oral Glucose (glucose gel/tablets/fruit juice) | Conscious patient with hypoglycaemia | 15-20 g oral |
| Midazolam (oromucosal solution) | Prolonged seizures/status epilepticus | 10 mg buccal (oromucosal); or 5 mg IM |
Secondary (Supplementary) Emergency Drugs:
| Drug | Indication | Route/Dose |
|---|---|---|
| Hydrocortisone sodium succinate | Adrenal crisis; second-line in severe anaphylaxis (prevents biphasic reaction) | 100 mg IV/IM |
| Atropine | Bradycardia (symptomatic); vasovagal syncope with bradycardia | 0.5-1 mg IV |
| Naloxone (Narcan) | Opioid overdose (respiratory depression) | 0.4-2 mg IV/IM; repeat every 2-3 min |
| Flumazenil | Benzodiazepine overdose/reversal | 0.2 mg IV over 15 sec; repeat if needed |
| Diazepam/Lorazepam | Status epilepticus | 5-10 mg IV slow; 2-4 mg IM |
Emergency Drug Use by Condition:
- Epinephrine 0.3-0.5 mg IM (1st line, immediate)
- High-flow O2
- Diphenhydramine 50 mg IM/IV (H1 blocker)
- Hydrocortisone 100 mg IV (prevents late phase)
- Salbutamol inhaler (if bronchospasm persists)
- Call ambulance; IV fluids
- Nitroglycerin 0.4 mg sublingual every 5 min (max 3 doses)
- O2
- Aspirin 300 mg chewed
- If persists >15 min → presumed MI → call 999/911
- Salbutamol 2 puffs MDI (patient's own or emergency kit)
- O2
- If no response → epinephrine 0.3 mg IM
- Hydrocortisone 100 mg IV (reduces inflammation)
- Conscious: 15-20 g oral glucose; repeat in 15 min if no improvement
- Unconscious: Glucagon 1 mg IM; do NOT give anything orally; IV dextrose 50% if IV access available
- Position: Supine with legs elevated (Trendelenburg)
- O2
- Atropine only if persistent bradycardia and hypotension
- Protect from injury; clear airway
- Time the seizure
- If >5 min → Midazolam 10 mg buccal/oromucosal (or Diazepam 10 mg rectal)
- O2 post-seizure
Emergency Equipment (must accompany drugs):
- Automated External Defibrillator (AED)
- Bag-Valve-Mask (BVM) for positive pressure ventilation
- Oropharyngeal airways (sizes 0-4)
- Oxygen cylinder with mask and regulator
- IV access kit + IV fluids
- Pulse oximeter
- Blood pressure cuff and stethoscope
- CPR face shield
2. Carnoy's Solution
Definition:
Historical Background:
Composition:
| Component | Volume | Role |
|---|---|---|
| Absolute (100%) Ethyl Alcohol | 6 mL | Dehydrant/fixative |
| Chloroform | 3 mL | Lipid solvent; enhances penetration |
| Glacial Acetic Acid | 1 mL | Denatures proteins; fixes nucleic acids |
| Ferric Chloride (FeCl₃) | 1 gram | Cauterizes/coagulates; enhances fixation |
Mnemonic: "6-3-1-1" = Alcohol 6 + Chloroform 3 + Acetic acid 1 + FeCl₃ 1g
- Excludes chloroform due to its carcinogenicity (hepatotoxic; IARC Group 2A carcinogen)
- Contains only ethanol + glacial acetic acid + ferric chloride
- Slightly less effective penetration but safer
Mechanism of Action:
- Ethanol - dehydrates and precipitates cellular proteins; damages cell membranes
- Chloroform - penetrates lipid-rich cell membranes; allows deeper tissue fixation
- Glacial acetic acid - denatures nuclear proteins; precipitates histones; causes cell shrinkage
- Ferric chloride - coagulation of tissue proteins; cauterizes blood vessels; deeper tissue penetration
Indications:
- Odontogenic Keratocyst (OKC/KCOT) - primary indication (high recurrence ~25-60% without adjunctive treatment)
- Unicystic ameloblastoma (after enucleation)
- Gorlin-Goltz syndrome (multiple OKCs - to minimize recurrence after each enucleation)
- Any jaw cyst with high recurrence potential where complete enucleation is difficult
Application Technique:
- Surgical enucleation of the cyst lining is first completed
- Protect adjacent soft tissues with petroleum jelly (Vaseline)-soaked gauze or a rubber dam around the wound margins
- Protect IAN: If inferior alveolar nerve is in close proximity, pack with Vaseline-soaked gauze to shield it
- Apply Carnoy's solution into the bony cavity using a cotton pellet or swab
- Allow contact for exactly 3-5 minutes (timer used)
- Remove the cotton pellet; thoroughly irrigate the cavity with copious normal saline to neutralize
- Pack/close wound as per standard post-enucleation protocol
Contraindications:
- Proximity to inferior alveolar nerve (without nerve protection) - can cause permanent paresthesia/anesthesia
- Near the mental foramen without protection
- In the presence of infection/acute inflammation
- Near vital tooth roots (risk of ankylosis/root resorption)
- Not for use near the maxillary sinus floor without protection
Advantages:
- Significantly reduces OKC recurrence from ~25% to ~5%
- Simple application technique
- No complex equipment required
- Chemical treatment of residual satellite cysts in cortical bone
Disadvantages:
- Chloroform - hepatotoxic and carcinogenic; WHO/IARC concern
- Risk of IAN damage if nerve not adequately protected
- Cannot be used in infected sites
- Possible root resorption/ankylosis of adjacent vital teeth
- Modified version (without chloroform) has slightly less penetration
3. Clinical Features and Surgical Management of Chronic Osteomyelitis of the Jaw
Definition:
Classification (Zurich Classification / Marx & Topazian):
- Primary chronic osteomyelitis - insidious onset; no suppuration; cause unknown (may be autoimmune); difficult to treat
- Secondary chronic osteomyelitis - sequel to acute suppurative osteomyelitis (inadequately treated); most common form
- Chronic suppurative
- Chronic sclerosing (diffuse/focal)
- Actinomycotic osteomyelitis
Etiology and Predisposing Factors:
- Inadequately treated acute osteomyelitis (most common cause)
- Odontogenic infection (periapical abscess, pericoronitis, periodontal disease)
- Post-extraction wound contamination
- Infected jaw fractures (especially compound mandibular fractures)
- Radiation (osteoradionecrosis)
- Systemic compromise: Diabetes mellitus, immunosuppression, sickle cell disease, chronic alcoholism, malnutrition
- Actinomyces israelii (in actinomycotic form)
Clinical Features:
- Dull, deep-seated, continuous pain (less intense than acute phase)
- Swelling - firm, indurated; may be intermittently tender
- Trismus - limited mouth opening (if masseteric/pterygoid muscles involved)
- Paresthesia/anesthesia of lower lip (Vincent's symptom) - IAN involvement
- Foul taste; halitosis
- Sinus tract/fistula - single or multiple intraoral and/or extraoral (skin of face/neck) openings discharging pus
- Pus discharge (purulent) from sinus openings
- Sequestrum - visible/palpable loose dead bone (may be discharged spontaneously through sinus)
- Lymphadenopathy - regional lymph nodes enlarged and tender
- Tooth loss - involved teeth become mobile and may be lost
- Pathological fracture - in advanced cases where extensive bone destruction weakens the mandible
- Masseter hypertrophy appearance if chronic and long-standing
- Extraoral: indurated swelling with scarring from healed/active sinuses
Investigations:
- OPG (Orthopantomogram): Moth-eaten (patchy radiolucent areas) + radio-opaque sequestra within; loss of trabecular pattern; involucrum (periosteal new bone formation visible as radioopaque rim)
- CT scan (best for extent, cortical erosion, and sequestra)
- MRI: Assesses soft tissue extension and medullary involvement; T1 low signal (edema replacing marrow fat)
- Tc-99m bone scan (scintigraphy): Increased uptake in active osteomyelitis; useful for staging; distinguishes from osteoradionecrosis
- Biopsy + culture/sensitivity: Microbiological diagnosis; mandatory for antibiotic selection (Staphylococcus aureus, Streptococcus, anaerobes, Actinomyces)
- Haematology: CBC (leukocytosis, elevated ESR, CRP); elevated WBC in acute exacerbations
Management of Chronic Osteomyelitis:
A. Medical Management:
- Long-term; guided by culture and sensitivity
- Empirical: IV Penicillin G + Metronidazole (covers aerobic streptococci + anaerobes)
- If S. aureus suspected: IV Cloxacillin or Vancomycin (MRSA)
- For actinomycotic: Prolonged penicillin (6-12 months)
- Clindamycin - excellent bone penetration; for penicillin-allergic patients
- Duration: Minimum 4-6 weeks; up to 3 months for severe cases
- Route: IV for 2-3 weeks; then oral completion
- Hyperbaric oxygen (HBO) - for refractory cases; as per Marx protocol
- NSAIDs + analgesics for pain
- Nutritional support
- Management of systemic predisposing conditions (diabetic control, etc.)
B. Surgical Management:
- Removal of the sequestrum (necrotic bone) from within the involucrum
- Approach: Mucoperiosteal flap elevated over the affected area
- Sequestra identified (loose, avascular, grayish bone without bleeding when cut) and removed with rongeurs/elevators
- Curettage of the granulation tissue lining the cavity
- Thorough irrigation with saline ± antiseptic
- Indicated for: Early/limited chronic osteomyelitis when sequestrum is well-demarcated and involucrum is adequate
- Removal of the outer cortical plate overlying the infected medullary cavity, converting a closed cavity to an open saucer-shaped wound
- Exposes the marrow cavity to the oral environment, allowing drainage and granulation tissue formation
- Bur used to drill multiple holes through cortex (trephination) to allow drainage in early phases
- Indicated for: Localized chronic osteomyelitis without sufficient natural drainage; combined with sequestrectomy
- Extensive removal of cortical bone and curettage of infected medullary bone
- Leaves the mandibular inferior border intact if possible
- Combined with long-term antibiotics and possible HBO
- For advanced, refractory, diffuse chronic osteomyelitis with:
- Pathological fracture
- Massive bone destruction
- Failure of conservative surgical treatment
- Actinomycotic involvement unresponsive to antibiotics
- Marginal resection: Removes infected cortical bone while preserving mandibular continuity
- Segmental (continuity) resection: Removes full segment of mandible when lower border is involved; immediate or delayed reconstruction with:
- Autogenous bone graft (iliac crest)
- Vascularized free fibula flap (preferred for large defects >6 cm)
- Titanium reconstruction plate (as spacer)
- Causative teeth and any teeth within the infected zone should be extracted
- Facilitates drainage and removes the microbial source
- Any pre-existing metalwork (plates, screws) within infected bone should be removed
Post-operative Care:
- Continue IV/oral antibiotics for 4-6 weeks minimum
- Regular wound irrigations
- Serial OPG/CT at 3-6 month intervals
- Nutritional support; physiotherapy for trismus
4. Basic Life Support (BLS)
Definition:
AHA 2020 Chain of Survival - Out of Hospital (6 links):
- Recognition and activation of emergency response
- Immediate high-quality CPR
- Rapid defibrillation (AED)
- Advanced resuscitation
- Post-cardiac arrest care
- Recovery (new 2020 link)
BLS Algorithm - Adult (C-A-B Sequence, AHA 2010 onwards):
- No normal breathing (gasping ≠ breathing) AND no pulse → begin CPR
| Parameter | Value |
|---|---|
| Position | Heel of dominant hand on lower half of sternum; second hand on top; fingers interlaced; arms locked straight |
| Depth | 5-6 cm (2-2.4 inches) adults |
| Rate | 100-120 compressions/minute |
| Recoil | Full chest recoil after each compression; do not lean on chest |
| Interruptions | Minimize; no pause >10 seconds |
- Head-tilt chin-lift (no suspected cervical spine injury)
- Jaw thrust (if cervical spine injury suspected)
- Pinch nose; seal mouth to mouth (or use face mask/barrier device)
- Give 1 breath over 1 second; watch for visible chest rise
- Ratio: 30 compressions : 2 breaths (all ages, single rescuer)
- Compression-only CPR acceptable for untrained rescuers
- With advanced airway (ET tube): 1 breath every 6 seconds (10/min); continuous compressions without pause
- Apply AED pads as soon as available (do not delay compressions to do this)
- Analyse rhythm: if shock advised → deliver shock → immediately resume CPR (2 min)
- If no shock advised → continue CPR → re-analyse every 2 minutes
Special Scenarios:
- 30:2 (single rescuer); 15:2 (two rescuers)
- 2 hands OR 1 hand compression; depth = 5 cm (2 inches); 1/3 of chest depth
- Rate: 100-120/min
- 2 fingers or 2-thumb encircling technique
- Depth = 4 cm (1.5 inches); Rate: 100-120/min
- 30:2 (single); 15:2 (two rescuers)
Recovery Position:
- For unconscious patients who have spontaneous breathing and pulse
- Roll into lateral (left lateral/recovery) position to prevent airway obstruction from tongue and vomit
BLS End Points:
- ROSC (return of spontaneous circulation)
- Advanced medical team takes over
- Rescuer physically exhausted and cannot continue
- Environmental/scene safety issues
5. Landmarks and Technique of Inferior Alveolar Nerve Block
Definition:
Structures Anaesthetized:
- All mandibular teeth on the side of injection (incisors to third molar)
- Buccal gingiva anterior to the mental foramen (via mental nerve)
- Lower lip and chin (via mental nerve)
- Anterior 2/3 of tongue + lingual gingiva (via lingual nerve - blocked as it traverses the pterygomandibular space)
- Floor of mouth (via lingual nerve)
Note: Buccal gingiva posterior to the premolars is supplied by the long buccal nerve (not anaesthetized by IANB; requires separate buccal nerve infiltration)
Anatomical Basis:
- The mandibular foramen lies on the medial aspect of the ramus, below and slightly behind the level of the coronoid notch
- Guarded anteriorly by the lingula (spine of Spix)
- The IAN is accompanied by the inferior alveolar artery and vein (vein is medial to artery; nerve is medial to both)
- The pterygomandibular space contains the IAN, lingual nerve, and sphenomandibular ligament
External Landmarks (Intraoral):
- Coronoid notch - the deepest concavity on the anterior border of the mandibular ramus (palpable intraorally by pressing on the anterior border of the ramus)
- Pterygomandibular raphe - a visible mucosal fold (tendinous junction of buccinator + superior pharyngeal constrictor muscles) running from the upper to lower alveolar ridge, medial to the coronoid notch
- Pterygomandibular triangle - the triangular fatty space bounded laterally by the coronoid notch and medially by the pterygomandibular raphe; the injection target
- Occlusal plane of mandibular teeth - horizontal reference; the needle is inserted approximately 1 cm (10 mm) above this plane
Needle Insertion Point:
- Horizontal: Three-quarters of the distance from the coronoid notch toward the pterygomandibular raphe (i.e., 3/4 from the coronoid notch = 1/4 from the raphe)
- Vertical: Approximately 1 cm above the mandibular occlusal plane
Syringe/Approach Angle:
- The barrel of the syringe is placed over the contralateral lower premolars (first/second premolars on the opposite side)
- This gives the needle the correct angulation to aim toward the medial ramus surface
- The bevel of the needle faces the ramus (bone)
- A long (32 mm), 25-gauge needle is standard
Technique - Step by Step:
- Patient seated semi-reclined; mouth wide open
- Operator positioned at 7-8 o'clock (right-handed operator, right IANB)
- Place thumb/index finger in the coronoid notch to establish vertical height
- Identify the pterygomandibular raphe medially
- Use aspirating syringe with 1.8 mL cartridge (2% lidocaine with 1:100,000 epinephrine)
- Long 25G needle, bevel orientation checked
- Retract the cheek with the non-dominant hand to expose the pterygomandibular triangle
- Place barrel over contralateral lower premolars
- Insertion point at 3/4 distance from coronoid notch toward raphe, 10 mm above occlusal plane
- Needle inserted at the established point; advance through the mucosa
- Penetrate through the buccinator/pterygomandibular space soft tissues
- The needle is advanced until it contacts bone (medial surface of mandibular ramus)
- Typical depth: 20-25 mm (approximately 3/4 of the needle length)
- If bone contact is NOT felt at 25 mm: needle may be posterior to ramus; withdraw slightly and redirect more medially
- If bone contact at <15 mm: needle too anterior (on coronoid); withdraw and re-angle more posteriorly
- Once bone contact is confirmed, withdraw the needle 1 mm away from periosteum
- Aspirate for 5-10 seconds; check for blood in the cartridge
- If blood aspirated → repositioned needle required (pterygoid plexus or inferior alveolar vessels punctured)
- Must aspirate twice (rotate needle 45° between aspirations) in two planes
- Inject 1.5-1.8 mL (full cartridge) slowly over 60-90 seconds (never inject fast)
- Slow injection reduces pain and minimises risk of toxicity
- As the needle is withdrawn halfway (approx 10-15 mm depth), deposit 0.3-0.5 mL of solution - this anaesthetises the lingual nerve en route
- Lingual nerve: 2-3 minutes (superficial position)
- IAN: 5-10 minutes (deeper; must wait before proceeding with treatment)
- Test: Ask patient if lip/tongue feels numb; test with probe before commencing surgery
Signs of Successful Block:
- Numbness of ipsilateral lower lip and chin
- Numbness of anterior 2/3 of tongue
- Absence of pain on probing the involved teeth
Complications:
- Failed block (~5-15%): Due to variant anatomy (bifid canal, high foramen), incorrect technique
- Intravascular injection (if aspiration not performed): LA toxicity
- Haematoma (pterygoid plexus puncture) → trismus
- Trismus (if muscle irritation from needle trauma or intramuscular injection)
- Temporary facial nerve palsy (parotid injection if needle too posterior and deep)
- Needle breakage (very rare; do not redirect bevel forcefully on bone)
- Transient IAN paresthesia (prolonged beyond expected duration due to direct nerve trauma)
6. Partsch II Procedure
Historical Background:
- Partsch I = Marsupialization (cystostomy): Window + suture cyst lining to oral mucosa; cyst decompresses and shrinks over time
- Partsch II = Enucleation with primary closure: Complete removal of the cyst lining and closure of the wound
Definition:
Indications:
- Small to medium-sized cysts that can be safely enucleated without risk to adjacent structures
- Radicular (periapical) cysts - after root canal treatment or extraction of the causative tooth
- Dentigerous cysts (when enucleation is possible without IAN/adjacent tooth risk)
- Residual cysts (after extraction)
- Primordial cysts
- Any cyst where definitive diagnosis and treatment are desired simultaneously
- Cysts where the operator is confident of complete removal of the entire cyst lining
Contraindications (prefer Partsch I instead):
- Very large cysts (risk of pathological fracture, IAN injury)
- Cysts in close proximity to vital structures (IAN, adjacent vital teeth, antrum floor)
- Pediatric patients with developing teeth
- Immunocompromised or high-risk patients
- Infected cysts (drainage/marsupialisation preferred first)
Surgical Technique:
- OPG, CBCT to determine cyst extent, proximity to IAN, teeth
- Blood investigations (if GA)
- LA (for small/medium cysts) or GA (large/posterior/multiple)
- Regional block + local infiltration around the cyst site
- Semi-lunar (Neumann's) incision OR envelope flap / three-sided flap (Ochsenbein incision)
- Incision design must provide adequate access without compromising flap vascularity
- Base of flap must be wider than the free margin (to preserve blood supply)
- Incision must not cross over the cyst (base of flap must rest on sound bone)
- Full-thickness mucoperiosteal flap elevated with Howarth periosteal elevator
- Expose the bone overlying the cyst
- Thin/perforated bone over the cyst removed with a bur/rongeur to create a window of access
- The cystic lining (bluish-white; tense) is now visible
- Using a Mitchell trimmer, periosteal elevator or Kilner's dissector, the cyst lining is carefully separated from the bone by blunt dissection
- Enucleation proceeds systematically from one edge - the lining must be kept intact (perforation increases risk of incomplete removal and increases recurrence risk)
- Work systematically around the entire circumference; keep the specimen intact
- If the apical root tips are within the cyst wall, apicoectomy may be performed simultaneously
- If the causative tooth requires extraction, this is done prior to enucleation
- Once fully separated, the complete cyst is removed in one piece if possible
- Inspect for completeness; check the bony cavity walls for any residual lining fragments
- Bony cavity walls curetted to remove any residual epithelial remnants
- For OKC/KCOT: Apply Carnoy's solution for 3-5 minutes to reduce recurrence
- For ameloblastoma: Peripheral ostectomy with bone bur (1-2 mm rim of bone removed)
- Thorough irrigation with sterile saline
- Most cavities fill naturally with blood clot then bone over 6-12 months
- Large cavities: May pack with iodoform gauze, Alvogyl, or bone substitute (Bio-Oss) or leave to fill with blood clot; or fill with autogenous bone chips/PRF (platelet-rich fibrin)
- Mucoperiosteal flap repositioned
- Interrupted sutures (3-0 Vicryl or chromic catgut) placed to achieve tension-free primary closure
- No dead space; flap must be well-supported on underlying bone
- Antibiotics (amoxicillin 500 mg TDS × 5-7 days)
- Analgesics (NSAIDs + paracetamol)
- Chlorhexidine mouthwash
- Specimen submitted for histopathology (mandatory)
- Review at 1 week (sutures), then serial OPGs at 3, 6, 12 months to monitor bone fill
Advantages of Partsch II over Partsch I:
- Definitive treatment in a single operation
- Provides complete histological specimen for diagnosis
- Shorter recovery time
- No foreign body in cavity
- Lower overall recurrence for most cysts (except OKC where marsupialization + delayed enucleation may be preferred)
Disadvantages:
- More technically demanding
- Risk to adjacent structures if cyst is large
- Risk of pathological fracture if aggressive in large cysts
- Risk of IAN damage
- Risk of incomplete removal (→ recurrence)
7. Genioplasty
Definition:
Indications:
| Deformity | Genioplasty Type |
|---|---|
| Microgenia (chin deficiency - commonest) | Sliding advancement |
| Macrogenia (chin protrusion) | Sliding setback |
| Vertical excess (long face chin) | Reduction genioplasty (wedge resection) |
| Vertical deficiency (short face chin) | Vertical augmentation (interposition graft) |
| Asymmetry (chin shift L or R) | Lateral repositioning / asymmetric cut |
| As adjunct to BSSO or LeFort I | To optimize chin position after jaw movement |
Pre-operative Assessment:
- Cephalometric analysis: Measure Pog-NB distance; soft tissue chin position; lower facial height
- Facial photographs (frontal + lateral + worm's eye view)
- Dental study models
- Surgical simulation/planning (digital or model)
- Mental nerve relationship to planned osteotomy
Surgical Technique - Sliding Genioplasty (Advancement):
- Nasotracheal intubation for GA
- Local anaesthetic (LA) infiltration to reduce bleeding and provide post-op analgesia
- Vestibular (sulcular) incision on the labial side, horizontally from canine to canine region
- Incision placed through mucosa and mentalis muscle; approx 1-1.5 cm above the gingival margin
- Must preserve an adequate band of mentalis muscle attached to bone to allow reattachment at closure (prevents chin ptosis/witch's chin deformity)
- Expose the entire symphysis and parasymphysis
- Identify and protect the mental foramina (both sides): exit the mental nerve bilaterally
- Blunt dissection around the mental foramen; maintain periosteal cuff around it
- Mark the chin midline (scored between the central incisors for alignment reference)
- Mark the planned osteotomy line with a sterile surgical marker
- Osteotomy must be at least 5 mm below the apices of the anterior teeth (canine root apices: 25-27 mm length; mental foramen is at the level of the second premolar root tip)
- Mark the planned advancement distance on the lateral bone surface
- Using a reciprocating or oscillating saw (Hall micro-sagittal saw / Stryker saw)
- Cut made in an upside-down V shape (or straight horizontal cut) from one side of the symphysis to the other, below the mental foramina bilaterally
- Osteotomy must extend through both cortices (buccal and lingual) completely
- Copious irrigation to prevent heat necrosis
- Osteotomes placed in the osteotomy to complete the cut and downfracture the chin segment
- The chin (distal) segment is now mobile and attached only to the inferior soft tissue pedicle (geniohyoid, genioglossus, digastric muscle attachments)
- The soft tissue pedicle maintains vascularity to the segment - CRITICAL (do not strip periosteum from the inferior surface)
- Chin segment advanced (or set back/rotated) to the pre-planned position
- Check the midline using the reference marks scored on the bone
- Check symmetry and the planned amount of movement
- Hold the chin segment in planned position
- Fix with a straight titanium plate (typically a 4-hole 1.5 mm or 2.0 mm plate) applied across the osteotomy site on the anterior surface with monocortical screws
- Confirm stable fixation
- Mentalis muscle reattachment is critical - the mentalis must be reapproximated to its superior stump with resorbable sutures to prevent post-operative chin ptosis (witch's chin)
- Mucosa closed with resorbable sutures (Vicryl 3-0 or chromic catgut)
Types of Genioplasty:
| Type | Technique | Indication |
|---|---|---|
| Sliding advancement | Chin segment advanced forward | Microgenia (most common) |
| Sliding setback | Chin segment moved posteriorly | Macrogenia/prognathic chin |
| Reduction (wedge resection) | Two parallel horizontal cuts; remove wedge of bone; close gap | Vertical excess |
| Augmentation (interposition) | Bone graft or alloplast placed between segments | Vertical deficiency |
| Double-step genioplasty | Two osteotomies for severe deficiency | Severe microgenia |
| Centralising | Asymmetric movement with rotation | Chin asymmetry |
Post-operative Care:
- Pressure dressing chin wrap for 2-3 weeks
- Soft diet for 6 weeks
- Avoid chin contact/trauma
- Post-op OPG to confirm plate position
Complications:
| Intraoperative | Postoperative |
|---|---|
| Mental nerve injury (most common) | Chin ptosis/witch's chin (mentalis not reattached) |
| Asymmetric osteotomy | Paresthesia/anaesthesia of chin (mental nerve) |
| Inadequate fixation/instability | Relapse |
| Condylar sag | Infection; plate exposure |
| Avascular necrosis (if inferior pedicle stripped) | Hardware failure |
8. Local Hemostatic Agents
Classification:
A. Mechanical (Passive) Agents - Form physical scaffold for clot
- Porcine-derived denatured gelatin; available as sponge, powder, or sheet
- Placed dry or moistened with saline/thrombin
- Mechanism: Highly absorbent (absorbs 40× its weight); provides porous matrix that activates platelet aggregation and supports fibrin clot formation; physical tamponade
- Absorption: Completely resorbed by hydrolysis in 4-6 weeks
- Use: Socket packing post-extraction; bone cavities; ENT/dental surgery
- Can be soaked in thrombin or tranexamic acid for enhanced effect
- Woven gauze/sheet of oxidized regenerated cellulose
- Mechanism: Lowers local pH → denatures blood proteins → forms gelatinous mass that physically occludes bleeding; also has bactericidal activity (low pH)
- Resorbed within 7-14 days
- Use: Surface bleeding; bony cavities; neurosurgery; dental extraction sockets
- Do NOT use with thrombin (the low pH inactivates thrombin)
- Mixture of beeswax + paraffin wax + isopropyl palmitate (softening agent)
- Mechanism: Pure mechanical tamponade; pressed into cancellous bone/bleeding marrow spaces; physically occludes vascular channels
- NOT absorbed; remains as foreign body
- Use: Cranial bone bleeding; sternal closure; mandibular cancellous bone bleeding during osteotomies
- Limitation: Inhibits bone healing; acts as foreign body; not for infected sites
- Available as sponge, sheet, or powder; from bovine or equine collagen
- Mechanism: Contact with collagen activates platelet aggregation via collagen receptors; stimulates coagulation cascade
- Resorbed within weeks
- Use: Socket packing; periodontal surgery; ENT; general surgery
B. Active (Chemical/Biochemical) Agents
- Human or bovine thrombin; available as powder or solution
- Mechanism: Converts fibrinogen directly to fibrin (bypasses earlier coagulation cascade steps); activates platelets via PAR-1 receptors
- Used alone (sprayed/dripped on wound) or combined with gelatin sponge (for deeper cavities)
- Use: Surface bleeding; combined with gelatin matrix (FloSeal = gelatin + thrombin)
- Two-component dual-syringe system: fibrinogen concentrate + thrombin solution (with calcium chloride and antifibrinolytic agents)
- Mechanism: Mimics the final stage of the coagulation cascade - thrombin converts fibrinogen to fibrin → fibrin polymerizes → forms an adherent fibrin clot that seals the wound surface
- Also provides tissue adhesion (used as tissue sealant/glue)
- Resorbed within 10-14 days
- Use: Difficult-to-suture wounds; liver lacerations; maxillofacial surgery; cardiac surgery; patients with coagulopathies
- Caution: Risk of viral transmission (if pooled plasma-derived); bovine aprotinin may cause hypersensitivity
- Gelatin matrix (granular) + bovine thrombin mixed into a flowable paste
- Mechanism: Gelatin swells and physically tamponades; thrombin converts local fibrinogen to fibrin
- Adapts to irregular wound shapes; can be injected into cavities
- Use: Complex geometries; bone cavities; spine surgery; dental implant sites
C. Antifibrinolytic Agents
- Synthetic lysine analogue
- Mechanism: Competitively inhibits plasminogen activation → prevents plasmin formation → inhibits fibrinolysis → prevents clot breakdown
- Routes: IV, oral, or topical (soaked gauze/mouthwash - especially in dental patients on anticoagulants)
- Topical use in dentistry: Tranexamic acid 4.8% mouthwash (Cyklokapron) - rinse 10 mL for 2 minutes QDS × 5 days; prevents socket bleeding in anticoagulated patients
- Indication: Patients on warfarin, haemophiliacs, platelet disorders, hereditary haemorrhagic telangiectasia
- IV use: major trauma/bleeding (CRASH-2 trial evidence)
- Similar to TXA; antifibrinolytic
- Less commonly used; oral/IV
- Epinephrine 1:1,000 or 1:200,000 in saline or LA solution
- Topical adrenaline-soaked gauze placed on wound
- Mechanism: α1-adrenergic receptor activation → vasoconstriction → reduces blood flow to wound
- Used intraoperatively to reduce surgical field bleeding
- Caution: Systemic absorption; do not use on fingers/toes (ischaemia risk); use cautiously in cardiac patients
Summary Table:
| Agent | Type | Mechanism | Absorption |
|---|---|---|---|
| Gelfoam | Mechanical | Physical scaffold | 4-6 weeks |
| Surgicel | Mechanical/chemical | pH↓, denatures proteins, bactericidal | 7-14 days |
| Bone wax | Mechanical | Physical tamponade of bone | NOT absorbed |
| Collagen sponge | Mechanical | Platelet activation | Weeks |
| Thrombin | Active | Fibrinogen → Fibrin | Days |
| Fibrin glue | Active | Final clotting cascade | 10-14 days |
| FloSeal | Mechanical + Active | Swelling + thrombin activation | Weeks |
| Tranexamic acid | Antifibrinolytic | Prevents plasmin | N/A (topical/systemic) |
| Epinephrine | Vasoconstrictor | Vasoconstriction | Minutes |
9. Universal Infection Control Precautions (Standard Precautions) in Dental Practice
Background:
- Aerosols and splatter generated by drills, scalers, and air-water syringes
- Direct exposure to blood and saliva
- Sharp instrument use (needles, scalpel blades, burs)
Components of Standard Precautions in Dentistry:
1. Hand Hygiene (Most Important Single Measure):
- Wash hands with soap and water for ≥20 seconds before gloving, after removing gloves, before/after patient contact
- Use alcohol-based hand rub (ABHR ≥60% alcohol) when hands are not visibly soiled
- WHO 5 Moments of Hand Hygiene: Before/after patient contact, before clean procedures, after body fluid exposure, after touching patient surroundings
2. Personal Protective Equipment (PPE):
| PPE | When Used | Standard |
|---|---|---|
| Gloves (non-sterile nitrile/latex) | All patient contact involving mucosa, blood, body fluids | Change between each patient; never wash/reuse |
| Surgical mask (ASTM Level 2-3) | All procedures generating aerosols; routine examinations | Change if wet or per-patient |
| N95/FFP2/FFP3 respirator | Aerosol-generating procedures (AGPs) on known/suspected TB, COVID-19, etc. | Fit-tested; sealed |
| Eye protection / face shield | Any risk of splatter to eyes (all drilling procedures) | Full-face shield during aerosol procedures |
| Protective gown/apron | All procedures; change if contaminated | Single-use or launderable |
3. Respiratory Hygiene/Cough Etiquette:
- Patients/staff: cover cough/sneeze with tissue; dispose immediately; hand hygiene
- Masks for symptomatic patients in waiting areas
4. Sharp Instrument Safety:
- Never recap needles with two hands; use one-hand scoop technique or needle re-capper device
- Dispose of all sharps (needles, scalpel blades, burs) immediately into a UN-approved puncture-resistant sharps container
- Never pass sharps hand-to-hand; use a neutral zone (tray/kidney dish)
- Sharps containers must be disposed of when 3/4 full (not completely full)
- Needle-stick injury protocol: Encourage bleeding, wash with soap and water, report to infection control officer, baseline serology (HIV, HBV, HCV), post-exposure prophylaxis (PEP) if indicated within 72 hours
5. Instrument Reprocessing (Sterilisation):
| Category | Definition | Decontamination |
|---|---|---|
| Critical (penetrate sterile tissue/blood) | Surgical instruments, needles, extraction forceps, burs | Sterilisation (autoclave) |
| Semicritical (contact mucosa/non-intact skin) | Dental mirrors, amalgam condensers | High-level disinfection minimum; sterilisation preferred |
| Non-critical (contact intact skin only) | X-ray aprons, blood pressure cuff | Intermediate/low-level disinfection |
- Pre-vacuum autoclave (134°C / 3 min or 121°C / 15 min) - gold standard for dental instruments
- Indicator testing: Class 6 chemical indicators in each pack; Geobacillus stearothermophilus biological indicators weekly
- Single-use items: Needles, cartridges, scalpel blades, suction tips - never reuse
- Instruments cleaned (ultrasonic bath / washer-disinfector) before bagging and sterilising
6. Environmental Surface Disinfection:
- Clinical contact surfaces (light handles, chair controls, bracket table) - barrier protection (plastic/paper wrap, changed per patient) OR wipe with intermediate-level disinfectant (sodium hypochlorite 1:100, or surface-compatible alcohol)
- Non-clinical housekeeping surfaces: regular cleaning; disinfectant if blood contamination
- Dental unit waterlines: Flushing protocols (run for 20-30 sec between patients); use sterile water for surgical procedures; anti-retraction valves
7. Dental Waterline Safety:
- Dental unit waterlines colonise with Pseudomonas, Legionella and other opportunistic organisms
- Flush lines for 20-30 seconds between patients and at start/end of day
- Sterile water for surgical irrigation; do not use municipal water for oral surgery
8. Waste Disposal:
- Clinical/hazardous waste (blood-contaminated items, used dressings): Yellow clinical waste bag (incinerated)
- Sharps: Yellow/orange sharps bin
- Domestic waste: Black bag
- Follow local authority/regulatory guidelines (UK: HTM 07-01)
9. Post-Exposure Protocol (Needle-stick/Blood Splash):
- Wound first aid: Encourage bleeding → wash soap+water → do not suck
- Eyes/mucosa: Irrigate copiously with water/saline
- Report to infection control officer within 1-2 hours
- Baseline serology (HIV, HBV, HCV) on both patient and healthcare worker
- Post-exposure prophylaxis (PEP): For HIV: 3-drug HAART regimen; must start within 72 hours (ideally <2 hours)
- Follow-up serology at 6 weeks, 3 months, 6 months
10. Anterior Maxillary Segmental Osteotomy (AMO)
Definition:
Historical Evolution:
- Cohn-Stock (1921): First described anterior maxillary osteotomy (palatal approach - rarely used)
- Wassmund (1935): Modified technique; labial approach only; periosteum preserved at base; segment repositioned through a palatal split (but without full mobilisation - orthodontic finishing required)
- Wunderer (1962): Palatal pedicle technique; segment mobilized with palatal blood supply preserved; allows greater freedom of movement
- Cupar (1954): Combined buccal and palatal approach
- Epker (1977): Further refinements
Indications:
- Maxillary dentoalveolar protrusion (bimaxillary protrusion) - excessive forward position of the anterior maxillary teeth and alveolus
- Anterior open bite - correction by superior repositioning of the anterior segment (closing the bite)
- Anterior crossbite (mild) - where LeFort I is not necessary
- Excessive overjet limited to anterior alveolus
- When LeFort I is inappropriate (e.g., posterior dentition acceptable; only anterior problem)
- Post-orthodontic residual dentoalveolar protrusion that cannot be resolved by orthodontics alone
Contraindications:
- Insufficient bone between tooth roots and intended osteotomy site
- Inadequate pre-surgical orthodontic preparation
- Active dentoalveolar infection
- Poor blood supply/compromised vascularity to the segment
Anatomy of Blood Supply (Critical):
Techniques:
- Subperiosteal buccal dissection only
- Vertical osteotomies through buccal bone (premolar extraction sockets)
- Segment is NOT fully mobilised; it "swings back" on a periosteal hinge
- Useful for mild corrections; limited freedom of movement
- Provides full mobilisation of the segment
- Blood supply maintained via palatal mucoperiosteal pedicle
Surgical Steps (Wunderer/Standard Technique):
- Bilateral premolar extractions (first premolars in most cases) 3-6 weeks before surgery to allow initial socket healing
- Pre-surgical orthodontics to level/coordinate arches
- Surgical splint (occlusal) fabricated from model surgery
- General anaesthesia via nasotracheal intubation
- LA infiltration for hemostasis
- Horizontal vestibular incision in the labial/buccal sulcus from canine to canine (or premolar to premolar)
- Full-thickness mucoperiosteal flap elevated on the buccal/labial aspect of the anterior maxilla
- Do NOT reflect the palatal mucoperiosteum (preserve vascular pedicle)
- Two vertical osteotomies made through the premolar extraction sockets (or at the canine-premolar junction if sockets not available)
- Cut from the alveolar crest through the body of the maxilla upward toward the nasal floor
- Must be at least 5 mm from root apices of adjacent teeth to preserve vitality
- Oscillating saw or fine reciprocating saw
- A horizontal cut through the lateral maxillary wall bilaterally, connecting the upper ends of both vertical cuts
- Connects across the anterior face of the maxilla, above the root apices
- Cuts made from the buccal surface through to (but not violating) the palate
- If setback movement is planned, the anterior nasal spine and septal bone may need to be transected
- A downfracture or controlled greenstick of the nasal floor allows the segment to tilt
- The anterior segment is now mobile, attached only by the palatal mucoperiosteal pedicle
- Test mobility carefully with a Rowe disimpaction forceps or similar; ensure full freedom of movement in all planned directions
- Segment repositioned to the planned position using the surgical occlusal splint as a reference
- IMF established briefly to verify occlusion
- Fixation: Titanium miniplates (1.3-1.5 mm) placed on the lateral maxillary walls across the osteotomy at the junction of the vertical cuts; OR interosseous wiring
- Release IMF
- Labial mucoperiosteal flap closed with resorbable sutures
Movements Achievable:
- Setback (most common - for prognathism)
- Superior repositioning (intrusion - for open bite correction)
- Inferior repositioning (downward - for deep bite/vertical deficiency; needs bone graft)
- Forward advancement (for retruded anterior segment)
- Combination movements (setback + intrusion for bimaxillary protrusion with open bite)
Complications:
| Complication | Notes |
|---|---|
| Avascular necrosis of segment | Most serious; due to palatal pedicle damage; prevents healing |
| Loss of tooth vitality | Root proximity to osteotomy; ischaemia |
| Oro-nasal/oro-antral fistula | If nasal floor violated without repair |
| Relapse | Most common long-term complication |
| Wound dehiscence | Tension on closure; flap design errors |
| Nasal septal deviation | If anterior nasal spine not repositioned appropriately |
| Inadequate mobilisation | Insufficient bone removal |
Quick Summary Table
| Topic | Key Exam Points |
|---|---|
| Emergency drugs | O2, Epinephrine (anaphylaxis), GTN (angina), Aspirin (MI), Salbutamol (asthma), Glucagon (hypoglycaemia), Midazolam (seizures), Diphenhydramine (allergy) |
| Carnoy's solution | 6mL ethanol + 3mL chloroform + 1mL glacial acetic acid + 1g FeCl₃; adjunct to OKC enucleation; 3-5 min application; protect IAN with Vaseline |
| Chronic osteomyelitis | Sequestrum + involucrum + sinus; Vincent's symptom; treatment = sequestrectomy, saucerization, decortication, resection ± HBO |
| BLS | C-A-B; 30:2; 100-120/min; 5-6 cm depth; AED as soon as available; 2020 = added "Recovery" link |
| IAN block | 3/4 from coronoid notch to raphe; 1 cm above occlusal plane; barrel over contralateral premolars; 20-25 mm depth; aspirate × 2 before injecting |
| Partsch II | Complete enucleation + primary closure; flap-bone window-dissect intact cyst-curettage-Carnoy's (OKC)-closure; specimen to histology |
| Genioplasty | Horizontal osteotomy ≥5 mm below root apices; preserve inferior pedicle (vascularity); protect mental nerve; mentalis reattachment prevents chin ptosis |
| Local hemostatic agents | Mechanical (Gelfoam, Surgicel, bone wax, collagen); Active (thrombin, fibrin sealant, FloSeal); Antifibrinolytic (tranexamic acid) |
| Infection control | Hand hygiene; PPE; single-use sharps; autoclave (134°C/3min); Spaulding classification; needle-stick PEP within 72h |
| AMO | Wassmund (labial approach) / Wunderer (palatal pedicle); preserve palatal vasculature; premolar extractions pre-op; miniplates; for maxillary prognathism/open bite |
1. Cryosurgery. 2. Principles of Elevator. 3. Mental nerve block. 4. Dentigerous cyst. 5. Leukoplakia. 6. Miniplate Osteosynthesis. 7. Dry socket. 8. Frey’s syndrome. 9. Gow gates technique. 10. Bone grafts
principles dental elevator types uses fulcrum lever wheel axle wedge oral surgery impacted tooth extraction Gow Gates technique landmarks mandibular block
mental nerve block technique landmarks incisive nerve block indications oral surgery miniplate osteosynthesis Champy lines principles types titanium fixation
cryosurgery oral cavity liquid nitrogen mechanism freeze-thaw cycle indications complications dentigerous cyst radiograph treatment pathology
Gow Gates block technique condylar neck target area landmarks syringe angulation structures anesthetized dry socket alveolar osteitis pathogenesis management treatment
bone graft types classification autogenous allograft xenograft alloplast osteoconduction osteoinduction osteogenesis BMP properties oral maxillofacial
Enucleation. 2. Ossifying fibroma. 3. Internal derangement. 4. Trans alveolar extraction. 5. Local complications of local anesthesia. 6. Fibrous dysplasia. 7. Sub mandibular space infection. 8. Hyperbaric O2 therapy. 9. Osteoradionecrosis. 10. Bell’s palsy. Don’t answer previously answered questions