Diagnosis and management of ventricular fibrillation and pulseless VT
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ventricular fibrillation" AND "cardiac arrest" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full detailed answer.
Ventricular Fibrillation and Pulseless Ventricular Tachycardia: Diagnosis and Management
VF and pulseless VT (pVT) are the two shockable cardiac arrest rhythms. They are treated identically because they share the same underlying mechanisms and respond to the same interventions: high-quality CPR, defibrillation, vasopressors, and antidysrhythmics. Together they carry the best prognosis among all cardiac arrest rhythms - survival is relatively high, especially when VF is "coarse," the arrest is witnessed, and prompt CPR plus defibrillation are initiated.
1. Pathophysiology
Ventricular Fibrillation
VF is characterized by disordered electrical ventricular activation without identifiable QRS complexes. The underlying mechanisms include spiral wave reentry and multiple circulating reentry wavefronts. Sustained polymorphic or monomorphic VT that degenerates to VF is a common cause of out-of-hospital cardiac arrest. Both rhythms often have a primary cardiac origin. - Harrison's 22E, p. 2014
The autonomic nervous system plays a key role: elevated sympathetic signaling in heart disease leads to elevated norepinephrine and neuropeptide Y release, shortening of action potential and refractory period durations. Nerve death and nerve sprouting at scar border zones create a substrate for reentrant arrhythmias. - Braunwald's Heart Disease
ECG recognition:
- VF: Chaotic, irregular waveforms with no discernible P waves or QRS complexes; amplitude varies from coarse (larger deflections, more likely to respond to shock) to fine (smaller, lower-amplitude).
- Pulseless VT: Wide QRS complexes (>120 ms), regular rate typically >100 bpm, no palpable pulse despite organized electrical activity.
2. Immediate Management Algorithm
The standard resuscitation framework follows the CPR - Shock - Drug cycle. The two algorithms below (from Rosen's Emergency Medicine and Harrison's 22E) summarize current ACLS-based management:
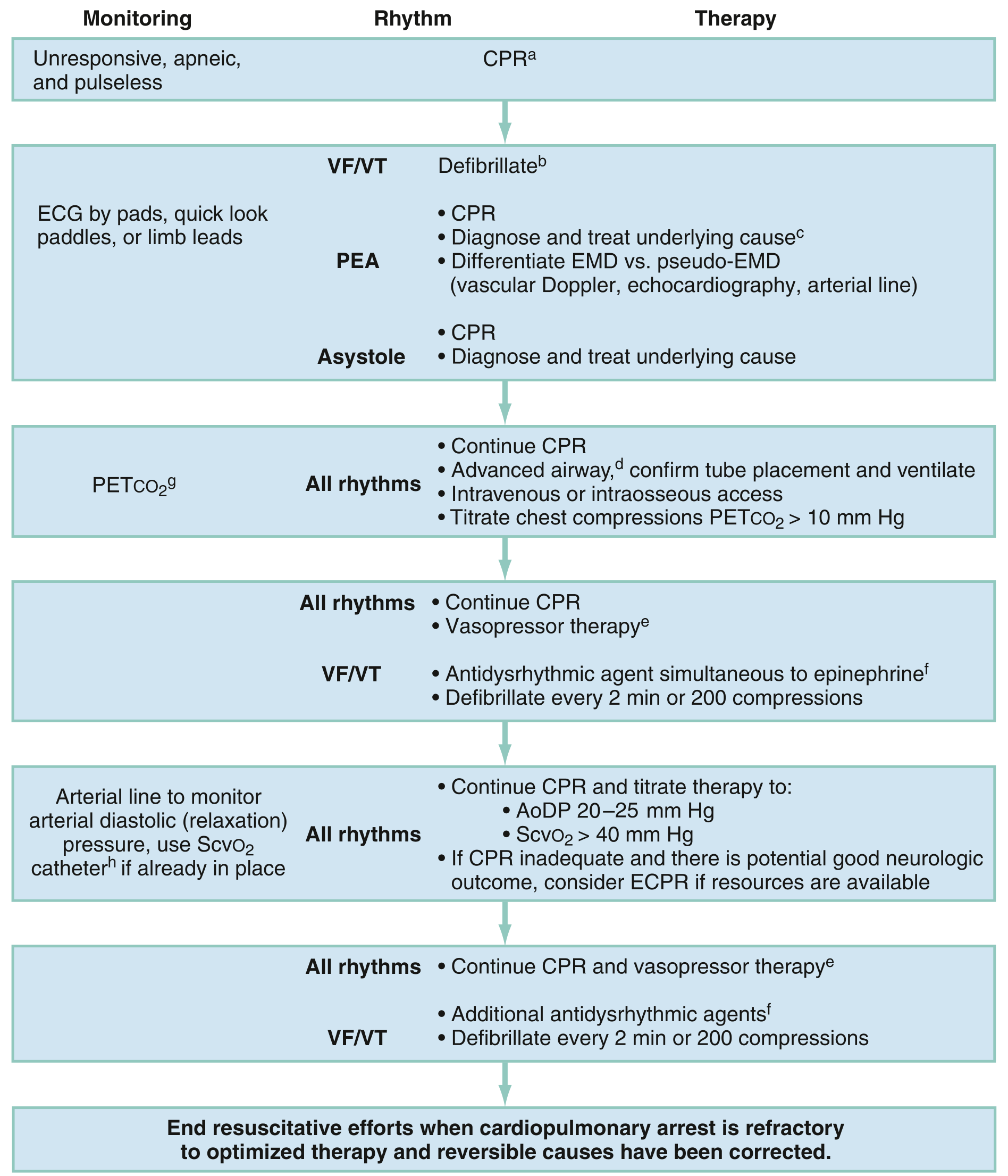
3. Step-by-Step Resuscitation Protocol
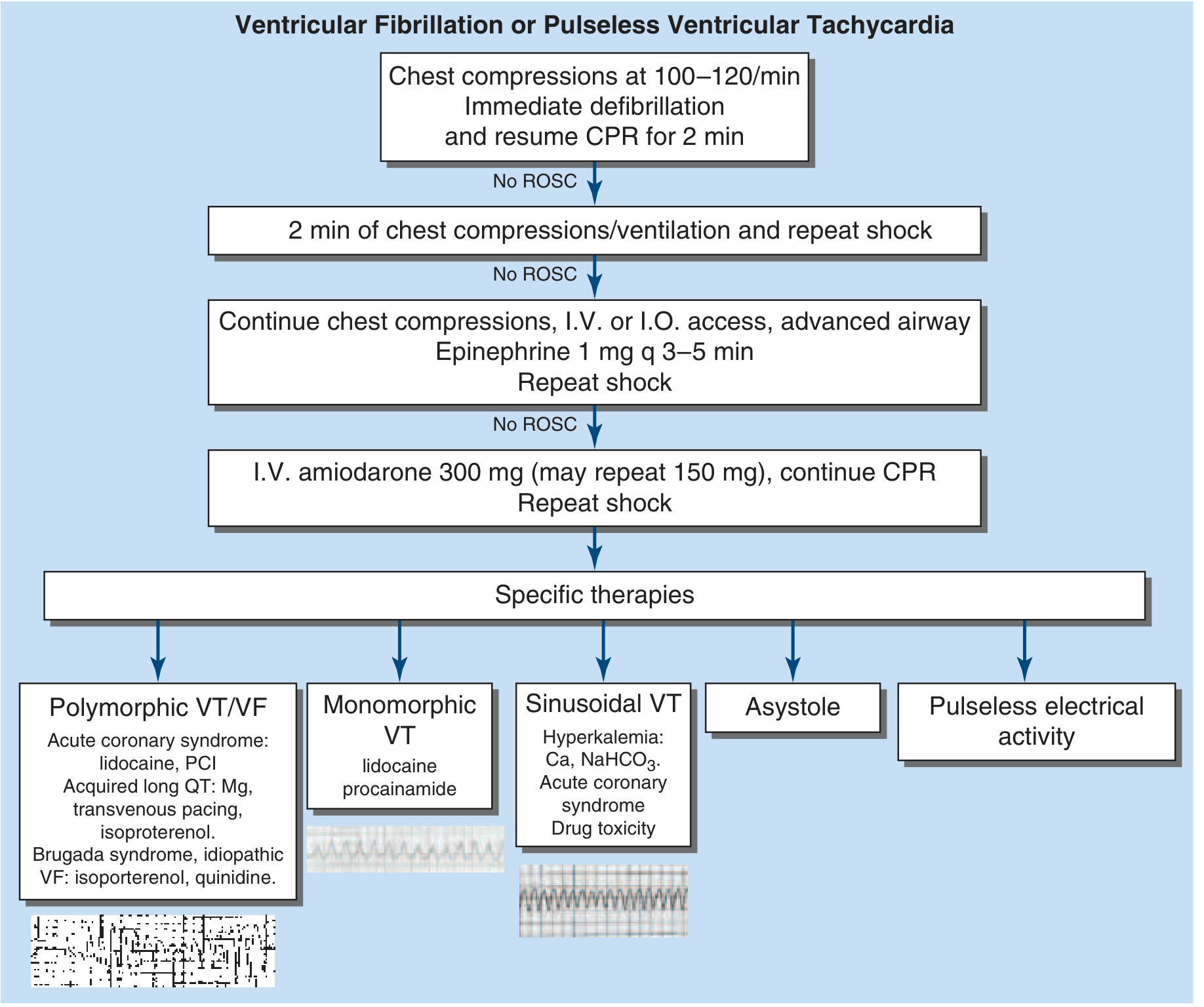
Step 1 - Immediate CPR + Defibrillation
- Begin chest compressions immediately upon confirming the patient is unresponsive and pulseless; continue until a defibrillator is available.
- Compression rate: 100-120/min, depth 2-2.4 inches, allow full chest recoil, minimize interruptions.
- Deliver a single shock with minimal interruption to CPR. Immediately resume compressions after the shock for 2 minutes before the next rhythm check.
- Biphasic defibrillators: use manufacturer-recommended energy (typically starting at 200 J, escalating to 360 J if needed). Monophasic: 360 J for all shocks.
- Biphasic waveforms lower the defibrillation threshold and reduce post-shock myocardial dysfunction vs. monophasic. However, superiority for ROSC or survival to discharge has not been conclusively demonstrated. - Rosen's EM, p. 80
- Placing defibrillation pads early allows continuous compressions while the device charges - this maximizes compression fraction.
Step 2 - Vascular Access + Advanced Airway (if no ROSC after 1st shock)
- Establish IV or intraosseous (IO) access while CPR continues.
- Advanced airway (endotracheal intubation or supraglottic airway) should be placed with minimal interruption to compressions.
- Monitor PetCO₂ - target >10 mmHg; values >20 mmHg suggest adequate CPR quality and correlate with ROSC.
Step 3 - Vasopressor Therapy
- Epinephrine 1 mg IV/IO every 3-5 minutes.
- Mechanism: increases myocardial contractility, elevates perfusion pressure, may convert electromechanical dissociation, and improves chances of successful defibrillation. - Braunwald's Heart Disease
- Vasopressin was previously listed as an alternative but has been removed from current ACLS algorithms due to lack of added benefit. - Tintinalli's EM
Step 4 - Antidysrhythmic Therapy (if VF/pVT persists after epinephrine + shocks)
No antidysrhythmic agent is superior to electrical defibrillation. Drugs should never delay or replace defibrillation - the priority is always shock first.
| Drug | Dose | Notes |
|---|---|---|
| Amiodarone (first-line) | 300 mg IV rapid push; repeat 150 mg for recurrent/resistant VF; max 2 g/day | Has Na, K, Ca, alpha, and beta-blocking properties. Three RCTs showed improved survival to hospital admission (not to discharge) vs. placebo in shock-resistant arrest |
| Lidocaine (alternative if amiodarone unavailable) | 1-1.5 mg/kg IV bolus; repeat 0.5-0.75 mg/kg q5-10 min; max 3 mg/kg | Primarily antiectopic; few hemodynamic effects; reverses ischemia-induced reduction in VF threshold |
| Magnesium sulfate | 1-2 g IV | Use specifically for torsades de pointes (TdP) or documented hypomagnesemia; not for routine VF |
Sources: Barash Clinical Anesthesia 9e; Rosen's EM; Tintinalli's EM
After giving any drug, provide at least 30-60 seconds of effective CPR to allow the drug to reach the central circulation before delivering the next shock. - Tintinalli's EM, p. 201
Step 5 - Continue the Cycle
Maintain the rhythm: CPR (2 min) → Rhythm check → Shock if shockable → CPR → Vasopressor ± antidysrhythmic → Repeat until ROSC, rhythm change, or decision to terminate.
4. Refractory VF/pVT
When VF persists despite multiple shocks, quality CPR, and pharmacotherapy:
Double Sequential External Defibrillation (DSED)
- Appropriate for shock-refractory VF (defined as ≥3 sustained episodes of VT/VF or ICD shocks within 24 hours).
- A second set of defibrillator pads is placed in the anterior-posterior position (if the first set is apex-sternum), for a total of 4 pads. Both defibrillators are charged to maximum and discharged simultaneously.
- Theorized mechanism: reduces VF threshold and overrides the relative refractory period of cardiac tissue. - Tintinalli's EM, p. 201
ECPR (Extracorporeal CPR)
- Consider if CPR is inadequate and there is potential for good neurologic outcome, and resources are available. - Rosen's EM algorithm
5. Specific Therapies Based on Rhythm Subtype
Once ROSC or rhythm clarification occurs, specific underlying causes guide therapy:
| Rhythm Subtype | Likely Cause | Specific Therapy |
|---|---|---|
| Polymorphic VT / VF | Acute coronary syndrome | Lidocaine, emergent PCI |
| Acquired long QT (TdP) | Drug toxicity, electrolytes | Magnesium sulfate, transvenous pacing, isoproterenol |
| Brugada syndrome / Idiopathic VF | Channelopathy | Isoproterenol, quinidine |
| Monomorphic VT | Scar reentry | Lidocaine, procainamide |
| Sinusoidal VT | Hyperkalemia | Calcium gluconate/chloride, NaHCO₃, treat underlying cause |
| Drug toxicity | QT prolongation | Identify and treat offending agent, magnesium |
Source: Harrison's 22E algorithm (Figure 317-2)
6. Post-ROSC (Post-Cardiac Arrest) Care
Hemodynamic Stabilization
- Maintain systolic BP >90 mmHg and mean arterial pressure >65 mmHg.
- Use vasopressors and volume adjustment as needed.
- Correct electrolyte abnormalities: hyperkalemia, severe hypokalemia, drug toxicity causing QT prolongation.
Coronary Angiography Considerations
- ST-elevation on post-ROSC ECG → emergent coronary angiography and PCI is recommended (majority will have a culprit lesion). - Harrison's 22E
- No ST-elevation → emergent angiography has NOT been shown to improve outcomes vs. delayed angiography; decisions are guided by hemodynamic/electrical instability and ongoing ischemia.
Targeted Temperature Management (TTM)
- Therapeutic hypothermia / TTM improves survival and neurologic recovery in patients presenting with shockable rhythms (VT/VF).
- Recommended for all post-arrest patients who remain comatose (lack of purposeful response to verbal commands) after ROSC, regardless of presenting rhythm.
- Target temperature: 32-37.5°C for at least 24 hours.
- A recent trial failed to demonstrate benefit of TTM vs. targeted normothermia with aggressive fever treatment, so active fever prevention remains a key component.
- Shivering suppression with analgesics and sedatives is often required.
- Do not initiate TTM pre-hospital with large-volume cold saline - this increased pulmonary edema risk without benefit. - Harrison's 22E, p. 2381
Neurological Monitoring
- Seizures and status epilepticus post-arrest worsen outcomes; monitor with periodic or continuous EEG.
- Treat clinically apparent seizures; also reasonable to treat ictal-interictal EEG patterns.
- Prognostication should be deferred ≥72 hours after return to normothermia (typically 4-5 days post-arrest) due to hypothermia and sedation confounding exam findings.
Predictors of poor neurologic outcome:
- Absent pupillary light reflex
- Status myoclonus
- Absence of EEG reactivity to external stimuli
- Persistent burst suppression on EEG
ICD for Secondary Prevention
- Patients with shockable arrest rhythms (VF/VT) not due to a transient reversible cause should receive an ICD for secondary prevention of sudden cardiac death (SCA/SCD). - Harrison's 22E
- Exception: VF occurring within the first 48 hours of a documented acute MI does not require ICD (similar 5-year SCD risk as non-arrest infarct survivors).
- However, large infarction with acutely depressed LVEF (e.g., <35%) warrants reassessment for ICD after recovery.
7. Long-Term Evaluation After Survival
Full workup to determine underlying etiology:
- Coronary artery disease: stress testing or angiography
- Structural heart disease: echocardiography, cardiac MRI (for cardiomyopathy, prior MI, valvular disease, LVEF)
- Inflammatory cardiomyopathy (sarcoidosis, myocarditis): cardiac PET scan, endomyocardial biopsy
- Primary electrical disease: Long QT syndrome, Brugada syndrome, early repolarization syndrome, WPW
- Epinephrine challenge for LQTS
- Sodium channel blocker challenge (procainamide) for Brugada
- Genetic evaluation if heritable syndrome suspected
- Catheter ablation: role in polymorphic VT and VF is rapidly evolving - simultaneous electrical recordings from basket catheters are being used to define critical ablation sites. - Harrison's 22E, p. 2015
Key Drug Summary
| Drug | Indication | Dose in Arrest |
|---|---|---|
| Epinephrine | All shockable + non-shockable arrest | 1 mg IV/IO q3-5 min |
| Amiodarone | VF/pVT refractory to shock | 300 mg IV push; +150 mg prn; max 2 g/day |
| Lidocaine | Alt. to amiodarone | 1-1.5 mg/kg IV; repeat 0.5-0.75 mg/kg q5-10 min; max 3 mg/kg |
| Magnesium sulfate | TdP, hypomagnesemia | 1-2 g IV |
| Calcium | Hyperkalemia-induced VT | IV calcium gluconate or chloride |
| Atropine | NOT recommended for VF/pVT or asystole | - |
| Vasopressin | Removed from ACLS algorithm | - |
Sources: Rosen's Emergency Medicine 10e; Tintinalli's Emergency Medicine 9e; Harrison's Principles of Internal Medicine 22E (2025); Barash Clinical Anesthesia 9e; Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.