Why beta blockers are preferred for angina give answer in flowchart
A clean, detailed medical flowchart titled "Why Beta Blockers Are Preferred in Angina" showing the following logic flow: Top box: "ANGINA PECTORIS - Imbalance: Myocardial Oxygen Demand > Supply" Arrow down to box: "Core Mechanism: Beta-1 Receptor Blockade in the Heart" Arrow down to three parallel outcome boxes side by side: 1. "↓ Heart Rate (negative chronotropy)" 2. "↓ Myocardial Contractility (negative inotropy)" 3. "↓ Blood Pressure & LV Wall Stress" All three arrows converge down to: "↓ Myocardial Oxygen DEMAND (Double Product = HR × SBP reduced)" Arrow down to: "↑ Diastolic Filling Time → ↑ Coronary Perfusion Time → ↑ Oxygen SUPPLY" Arrow down to large central box: "SUPPLY-DEMAND BALANCE RESTORED → Angina Relieved" Below that, split into two branches: Left branch "Additional Benefits": - Reduces frequency & severity of attacks - ↑ Exercise tolerance & duration - Reduces risk of MI & death (post-MI patients) - Improves survival in HFrEF - First-line antianginal therapy Right branch "Preferred Agents": - Metoprolol (cardioselective β1) - Atenolol (cardioselective β1) - Carvedilol (α+β blocker) - AVOID agents with ISA (e.g. pindolol) Bottom box in red/orange: "EXCEPTION: Vasospastic Angina — Beta Blockers are INEFFECTIVE and may WORSEN symptoms (use calcium channel blockers instead)" Use a professional medical style with blue header boxes, white content boxes, red warning box, green benefit boxes, connecting arrows throughout. Clean typography.
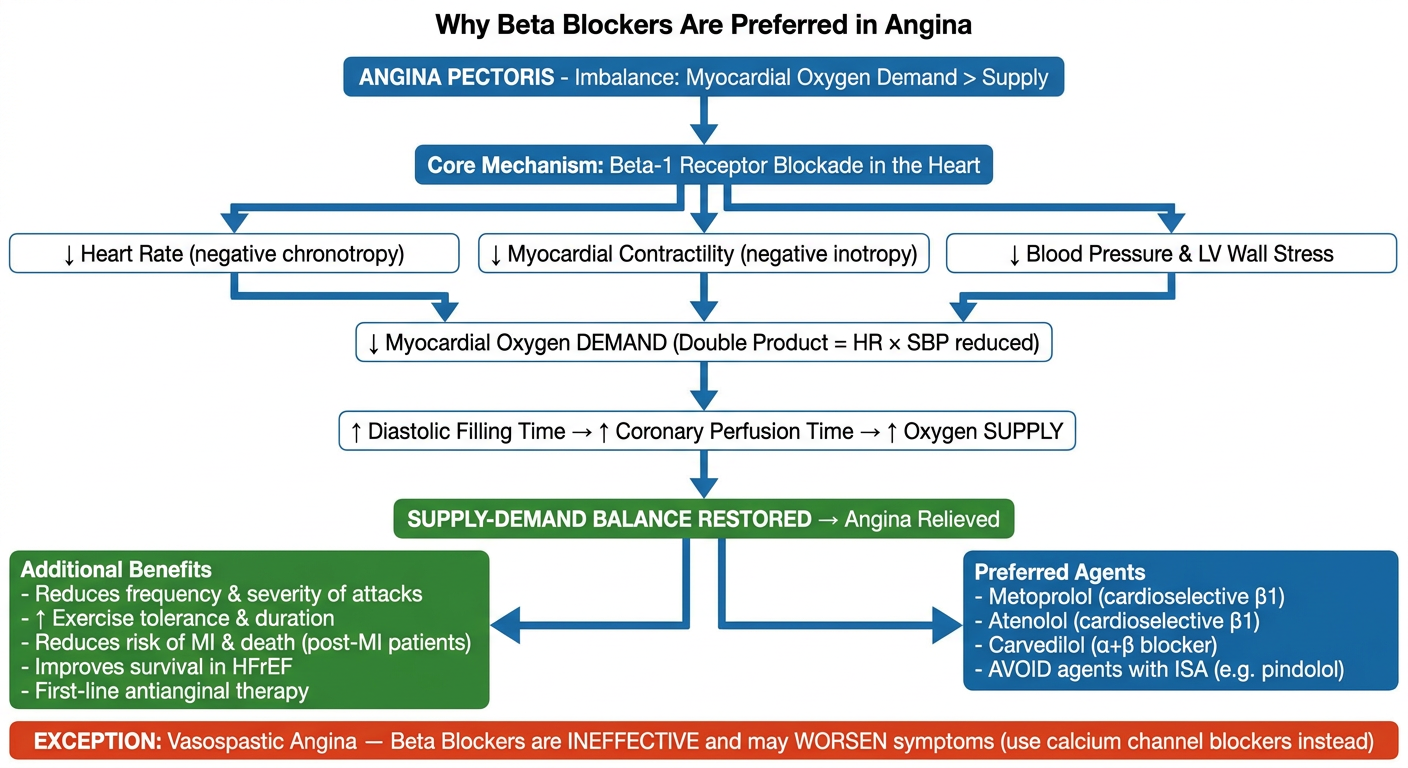
Why Beta Blockers Are Preferred in Angina
The Core Problem
Step-by-Step Mechanism (as shown in flowchart)
| Effect | Mechanism | Result |
|---|---|---|
| ↓ Heart Rate | Negative chronotropy | Less beats = less O2 consumed |
| ↓ Contractility | Negative inotropy | Less force = less O2 consumed |
| ↓ Blood Pressure / LV wall stress | Reduced afterload | Less wall tension = less O2 needed |
Why Beta Blockers Over Other Agents?
- First-line for all stable angina (unless contraindicated) - Lippincott Pharmacology, p.418
- Reduce risk of MI and death in post-MI patients
- Improve mortality in HFrEF - dual benefit in angina + heart failure
- Reduce both exertional and rest oxygen demand (unlike nitrates which mainly reduce preload)
- Better tolerability for long-term use vs. non-dihydropyridine CCBs (verapamil, diltiazem) which can cause more bradycardia/heart block concerns
Preferred Drugs
- Metoprolol, Atenolol (cardioselective beta-1 blockers) - preferred to avoid beta-2 side effects (bronchoconstriction, peripheral vasoconstriction)
- Carvedilol (alpha + beta blocker) - especially in patients with concurrent heart failure
- Avoid agents with intrinsic sympathomimetic activity (ISA) like pindolol in angina or post-MI