Caissons disease inthe form of saq
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have excellent, comprehensive content from multiple authoritative textbooks. Let me compose the full SAQ answer.
Caisson's Disease (Decompression Sickness / "The Bends")
Definition
Caisson's disease is a form of decompression sickness caused by the formation of nitrogen gas bubbles in the blood and tissues following rapid ascent from a high-pressure environment. The name comes from the pressurized underwater vessels ("caissons") used in bridge construction, where workers developed both acute and chronic forms of the condition.
- Robbins Pathologic Basis of Disease
Etiology / At-Risk Groups
- Scuba and deep-sea divers (most common)
- Underwater construction workers
- Aviators in unpressurized aircraft
- Astronauts (rapid decompression)
- Caisson workers (pressurized tunnel/bridge construction)
Risk factors: long/deep/repetitive dives, rapid ascent, cold water, heavy exertion at depth, obstructive lung disease, patent foramen ovale.
Pathophysiology (Henry's and Boyle's Laws)
- Henry's Law: At high ambient pressure, increased amounts of nitrogen dissolve in blood and tissues (especially fat, where N₂ is 5x more soluble than water).
- Rapid decompression (ascent): Ambient pressure drops quickly; tissues become supersaturated with nitrogen.
- Bubble formation: Nitrogen comes out of solution as gas bubbles in blood vessels and tissues.
- Consequences of bubbles:
- Mechanical compression of surrounding tissues
- Vascular occlusion → endothelial damage, ischemia, inflammation
- Activation of inflammatory mediators and reperfusion injury
- In the spinal cord: bubbles trapped in spinal vessels → ischemic myelopathy (predominantly upper thoracic cord, white matter, posterior > lateral > anterior columns)
- Goldman-Cecil Medicine; Adams and Victor's Principles of Neurology
Classification
| Type | Features |
|---|---|
| Type I (mild) | Joint pain ("bends"), limb numbness, rashes, lymphedema |
| Type II (severe) | Neurological, cardiopulmonary, or otic involvement |
Clinical Features
Type I - "The Bends"
- Joint pain (mild to severe) - classically knees, hips, shoulders
- Numbness/tingling in extremities
- Skin rashes, pruritus
- Lymphedema
Type II - Systemic/Neurological
- Neurological: Spastic myelopathy (upper thoracic cord), ataxia, aphasia, visual disturbances, paralysis, incontinence, confusion, loss of consciousness
- Cardiopulmonary ("Chokes"): Cough, substernal chest pain, tachypnea, dyspnea, pulmonary edema, respiratory distress; caused by gas bubbles in pulmonary vasculature causing edema, hemorrhage, and focal atelectasis/emphysema
- Otic: Vertigo, tinnitus, hearing loss (may be permanent if inner ear involved)
- Systemic: Fatigue, hypovolemic shock
Chronic Form - Caisson Disease (stricto sensu)
-
Persistence of gas emboli in the skeletal system → avascular necrosis
-
Common sites: femoral heads, tibia, humeri
-
Robbins Pathologic Basis of Disease; Goldman-Cecil Medicine; Adams and Victor's Neurology
Spinal Cord Involvement (Myelopathy)
-
Upper thoracic cord predominantly affected
-
White matter more than gray matter; posterior columns > lateral > anterior columns
-
May present as complete transverse myelopathy initially, then partially recover
-
Can leave permanent asymmetric, incomplete deficit
-
Residual: spasticity (lateral column damage) or leg numbness (posterior column damage)
-
Adams and Victor's Principles of Neurology
Diagnosis
- Clinical - based on history of pressure exposure + compatible symptoms
- Symptoms can appear within minutes to 24 hours after ascent (dives ≥20 feet)
- MRI: spinal cord ischemic lesions (upper thoracic)
- Arterial gas embolism: may show CNS or cardiac effects
Treatment
| Intervention | Details |
|---|---|
| Hyperbaric oxygen (HBO) - primary treatment | Recompression in hyperbaric chamber; forces gas bubbles back into solution. U.S. Navy Treatment Table 6 most commonly used. |
| Slow decompression | Gradual resorption and exhalation of gases; prevents re-formation of obstructive bubbles |
| 100% O₂ at surface | Given immediately while arranging HBO (displaces N₂) |
| IV fluids | Hydration to treat hypovolemia |
| Antispasticity drugs | For residual myelopathy |
| Physical therapy | For neurological sequelae |
- Contact Divers Alert Network (DAN): 919-684-9111 (24-hour consultation)
- Tintinalli's Emergency Medicine; Murray & Nadel's Respiratory Medicine; Adams and Victor's Neurology
Pathological Findings (Autopsy / Chronic)
-
Spinal cord: ischemic necrosis over 1-2 segments; occlusion of small arteries and veins
-
Skeletal system: multiple foci of ischemic (avascular) necrosis at femoral heads, tibia, humeri (from persistent gas emboli)
-
Lungs: edema, hemorrhage, focal atelectasis/emphysema
-
Fat embolism may coexist (N₂ dissolves preferentially in fat; fat may be released)
-
Robbins Pathologic Basis of Disease
Forensic Significance
-
Deaths may occur from pulmonary barotrauma, air embolism, or severe neurological injury
-
Annual incidence: ~1 case per 5,000-10,000 recreational dives; up to 10% of cases requiring recompression are fatal
-
Must be distinguished from high-altitude decompression sickness (similar symptoms, different circumstances)
-
Pulmonary barotrauma is the second leading cause of death among divers
-
Goldman-Cecil Medicine; P.C. Dikshit Forensic Medicine
Summary Box (SAQ Quick Recall)
Cause: Rapid ascent from high pressure → N₂ supersaturation → gas bubbles
Acute: Joint pain (bends), chokes (pulmonary), neurological myelopathy
Chronic: Avascular necrosis (femoral head, tibia, humerus)
Spinal cord: Upper thoracic, white > gray, posterior > anterior columns
Treatment: Hyperbaric oxygen (recompression) - U.S. Navy Table 6
Prevention: Slow, staged ascent; decompression stops
Define Apnoea,hyperpnoea,tachypnoea,dyspnoea
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Excellent content from Ganong's and Murray & Nadel's. I have everything needed for a thorough answer.
Definitions: Abnormal Breathing Patterns
1. Apnoea (Apnea)
Definition: Complete cessation of breathing (airflow) for a defined period of time.
- In clinical practice (e.g., sleep studies), an apnoea is defined as a >90% reduction in nasal airflow lasting for at least 10 seconds, regardless of whether it causes oxygen desaturation.
- May be central (no respiratory effort), obstructive (effort present but airway blocked), or mixed.
- Physiological apnoea occurs briefly after a deep breath (Hering-Breuer reflex) or voluntarily.
- Pathological apnoea occurs in obstructive sleep apnoea (OSA), neonatal apnoea, drug-induced respiratory depression, and brainstem injury.
"An apnoea is regarded as a completed cessation of airflow (more than 90% reduction in nasal airflow/pressure signal amplitude) for at least 10 seconds."
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
2. Hyperpnoea (Hyperpnea)
Definition: A general increase in the rate and/or depth of breathing, regardless of the patient's subjective awareness or discomfort.
- The patient may or may not be conscious of the increased ventilation.
- It is an objective sign, not a symptom.
- Causes include: exercise (physiological), fever, metabolic acidosis (e.g., diabetic ketoacidosis - Kussmaul breathing), anaemia, hypoxia, high altitude.
- Distinguished from dyspnoea: hyperpnoea does not require the patient to feel uncomfortable - it is simply increased ventilation.
"Hyperpnea is the general term for an increase in the rate or depth of breathing regardless of the patient's subjective sensations."
- Ganong's Review of Medical Physiology, 26th Edition
3. Tachypnoea (Tachypnea)
Definition: Rapid, shallow breathing - an increase in respiratory rate above normal (generally >20 breaths/minute in adults).
- It is an objective sign observed by the clinician.
- The rate is increased but tidal volume may be relatively shallow (unlike hyperpnoea, where depth also increases).
- Clinically significant thresholds: mild tachypnoea = 20-30 breaths/min; severe = >30-35 breaths/min (indicates impending respiratory failure).
- Tachypnoea is indicative of increased drive to breathe, but does not necessarily indicate alveolar hyperventilation (which is determined by rate AND tidal volume together).
- Causes: pneumonia, pulmonary embolism, heart failure, sepsis, pain, anxiety, fever, metabolic acidosis.
"Tachypnea is rapid, shallow breathing." "Tachypnea is indicative of an increased drive to breathe, although it is not necessarily evidence of alveolar hyperventilation, which is determined by rate and tidal volume."
- Ganong's Review of Medical Physiology; Murray & Nadel's Textbook of Respiratory Medicine
4. Dyspnoea (Dyspnea)
Definition: A subjective experience of breathing discomfort - the patient is consciously aware of difficulty or laboured breathing (shortness of breath, breathlessness).
The American Thoracic Society (ATS) consensus definition states:
"Dyspnea is a term used to characterize a subjective experience of breathing discomfort that is comprised of qualitatively distinct sensations that vary in intensity. The experience derives from interactions among multiple physiological, psychological, social, and environmental factors, and it may induce secondary physiological and behavioral responses."
Key points from the definition:
-
It is a symptom (reported by the patient), not a sign (observed by the clinician).
-
It is distinct from respiratory distress (which is the physical manifestation observed by others).
-
Multiple neural pathways are involved; causes include hypercapnia, hypoxia, and increased work of breathing.
-
Qualitative descriptors: "air hunger / not getting enough air" (increased respiratory drive); "chest tightness" (bronchoconstriction); "increased effort/work of breathing" (mechanical load or muscle weakness); "inability to get a deep breath" (dynamic hyperinflation).
-
Murray & Nadel's Textbook of Respiratory Medicine; Ganong's Review of Medical Physiology; Goldman-Cecil Medicine
Comparison Table
| Term | Type | Rate | Depth | Patient Aware? | Key Feature |
|---|---|---|---|---|---|
| Apnoea | Sign | Zero | Zero | Variable | Complete cessation of breathing |
| Hyperpnoea | Sign | ↑ or normal | ↑ | Not required | Increased ventilation (rate and/or depth) |
| Tachypnoea | Sign | ↑ (>20/min) | ↓ or normal | Not required | Rapid, shallow breathing |
| Dyspnoea | Symptom | Variable | Variable | Yes (essential) | Subjective breathing discomfort |
Key Distinctions to Remember
- Dyspnoea vs Hyperpnoea: Hyperpnoea is an objective increase in ventilation; dyspnoea is the subjective feeling of breathing difficulty. They often coexist but are not the same - a patient can have hyperpnoea without dyspnoea (e.g., during mild exercise).
- Tachypnoea vs Hyperpnoea: Tachypnoea = fast + shallow; Hyperpnoea = increased rate and/or depth.
- Apnoea vs Hypopnoea: Apnoea = >90% cessation of airflow; Hypopnoea = partial reduction in airflow (usually >30-50% reduction).
- A normal individual does not become conscious of breathing until ventilation is doubled, and breathing is not uncomfortable until ventilation is tripled or quadrupled (Ganong's).
Define Surfactant Through The Following :************ A) Composition B) Source And Secretion C) Functions**** D) Respiratory Distress Syndrome
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive, well-illustrated answer.
Surfactant - Complete SAQ Answer
A) Composition
Pulmonary surfactant is a complex mixture of phospholipids and proteins that lines the alveolar epithelium.
Lipid Component (~90% of total mass)
| Component | Details |
|---|---|
| Dipalmitoylphosphatidylcholine (DPPC) - also called dipalmitoyl lecithin | The most important component; accounts for almost all surface tension-reducing properties of surfactant |
| Phosphatidylglycerol | Second most abundant phospholipid |
| Other phospholipids | Phosphatidylethanolamine, phosphatidylinositol, sphingomyelin |
| Neutral lipids | Cholesterol, triglycerides (~10%) |
Protein Component (~10% of total mass)
Surfactant contains four specific surfactant-associated apoproteins (SP):
| Protein | Type | Function |
|---|---|---|
| SP-A | Hydrophilic (collectin) | Most abundant SP. Regulates surfactant homeostasis (synthesis & secretion). Modulates immune responses to viruses, bacteria, fungi. |
| SP-B | Hydrophobic | Transforms lamellar bodies into surface film. Critical for adsorption and spreading of surfactant onto alveolar epithelium. |
| SP-C | Hydrophobic | ~1% of total SP mass. Works with SP-B to orient DPPC within surfactant and maintain the thin film layer. |
| SP-D | Hydrophilic (collectin) | Primary host defense protein. Binds Gram-negative bacteria and lymphocytes; modulates innate immunity and inflammatory response to acute lung injury. |
- The superficial layer (facing alveolar air) is made of surface-active phospholipids, notably DPPC.
- The deeper layer (hypophase) consists of surface-active phospholipids linked to protein.
"The superficial layer of the film facing the alveolar air is made up of surface-active phospholipids, notably dipalmitoyl lecithin. The deeper layer, termed the hypophase, consists of surface-active phospholipids linked to protein."
- Fishman's Pulmonary Diseases and Disorders; Histology: A Text and Atlas (Ross & Pawlina)
B) Source and Secretion
Source
- Surfactant is produced exclusively by Type II alveolar pneumocytes (Type II alveolar epithelial cells), also known as granular pneumocytes or septal cells.
- Type II cells make up only ~5% of the alveolar surface area but are metabolically the most active alveolar cells.
- SP-B is also expressed by club cells (Clara cells) of the bronchioles, but SP-C is exclusive to Type II cells.
Intracellular Synthesis and Storage
- Phospholipids and proteins are synthesized in the endoplasmic reticulum.
- Processed via the Golgi complex and multivesicular bodies.
- Stored intracellularly in characteristic membrane-bound organelles called lamellar bodies (intracellular storage form of surfactant).
- Lamellar bodies appear as concentric whorls of lipid membranes on electron microscopy.
Secretion
- Secreted by constitutive exocytosis - the lamellar body fuses with the apical plasma membrane and releases surfactant into the alveolar lining fluid.
- After secretion, surfactant undergoes structural change in the aqueous layer, forming a meshwork called tubular myelin, which is rich in surfactant apoproteins.
- From tubular myelin, it forms the surface film at the air-water interface.
Stimuli that INCREASE secretion:
- Hyperinflation of the lungs (sighing, yawning, deep breathing)
- Exercise
- Beta-adrenergic agonists (clinical use!)
- Corticosteroids - stimulate surfactant lipid and protein formation
- Labor itself stimulates surfactant synthesis
- Fetal stress / intrauterine growth restriction (raises cortisol)
Factors that SUPPRESS secretion / maturation:
- Prematurity (<35 weeks gestation) - Type II cells are immature
- Maternal diabetes (high fetal insulin suppresses surfactant synthesis)
- Elective cesarean section before labor onset
Removal
Two mechanisms clear surfactant from the alveolar surface:
- Alveolar macrophages degrade some surfactant.
- Type II cells re-uptake the rest via endocytosis, then recycle or destroy it.
Fetal Development
- Surfactant synthesis begins after approximately week 20 of fetal gestation (in Type II cells as they differentiate).
- Clinically adequate quantities are produced after ~35 weeks gestation.
- A surge in maternal glucocorticoid levels just before birth triggers surfactant synthesis and secretion.
"The secretion of pulmonary surfactant occurs by constitutive exocytosis. In the fetus, both synthesis and secretion are quite low until immediately before birth, when a surge in maternal glucocorticoid levels triggers these processes."
- Medical Physiology (Boron & Boulpaep); Fishman's Pulmonary Diseases and Disorders
C) Functions
1. Reduces Alveolar Surface Tension (MOST IMPORTANT)
- By Laplace's law: Pressure = 2T/r - without surfactant, smaller alveoli (smaller radius) would have higher recoil pressure and empty into larger ones, causing atelectasis.
- Surfactant lowers surface tension in proportion to its concentration - as alveoli become smaller on expiration, surfactant becomes more concentrated on the surface and surface tension drops further, preventing collapse.
- This ensures equal pressure across alveoli of different sizes, maintaining alveolar stability.
2. Increases Lung Compliance
- By reducing surface tension, surfactant dramatically increases lung compliance (ease of inflation).
- Without surfactant, total elastic recoil increases by 2x or more, forcing the infant to exert tremendous effort with every breath.
3. Prevents Pulmonary Oedema
- Without surfactant, high surface tension would draw fluid from the interstitium into the alveolar space by a "sucking" effect, thickening the fluid layer and impairing gas diffusion.
- Surfactant keeps surface tension low, balancing the negative interstitial hydrostatic pressure and keeping alveoli dry.
4. Promotes Uniform Ventilation
- Surfactant allows alveoli to dynamically adjust their inflation/deflation rates, so that ventilation is uniform across alveoli of different sizes - preventing "fast alveoli" from emptying into "slow alveoli."
5. Reduces Work of Breathing
- By increasing compliance and stabilising alveoli, surfactant significantly reduces the muscular effort required for breathing.
6. Innate Immune Defence (SP-A and SP-D)
- SP-A and SP-D (collectins) bind to bacteria, viruses, and fungi, promoting opsonisation and phagocytosis by alveolar macrophages.
- SP-D participates in local inflammatory responses to acute lung injury and modulates immune responses to inhaled antigens.
"The pulmonary surfactant present at the alveolar air-water interface has three major effects: it increases compliance, it minimizes fluid accumulation, and it promotes uniform ventilation."
- Medical Physiology (Boron & Boulpaep); Fishman's Pulmonary Diseases and Disorders
D) Respiratory Distress Syndrome (RDS)
Also Known As:
- Infant / Neonatal Respiratory Distress Syndrome (IRDS / NRDS)
- Hyaline Membrane Disease (HMD)
Etiology
Surfactant deficiency in the immature lung of premature infants who cannot synthesize sufficient surfactant.
Incidence by gestational age:
- < 28 weeks gestation: ~60% of infants affected
- 28-34 weeks: ~30%
-
34 weeks: < 5%
Additional risk factors:
- Male gender
- Maternal diabetes (high fetal insulin suppresses surfactant)
- Cesarean section (before onset of labor)
- Perinatal asphyxia
Protective factors: Intrauterine stress, fetal growth restriction (raises cortisol - matures surfactant system faster), antenatal steroids given to mother.
Pathogenesis (Vicious Cycle)
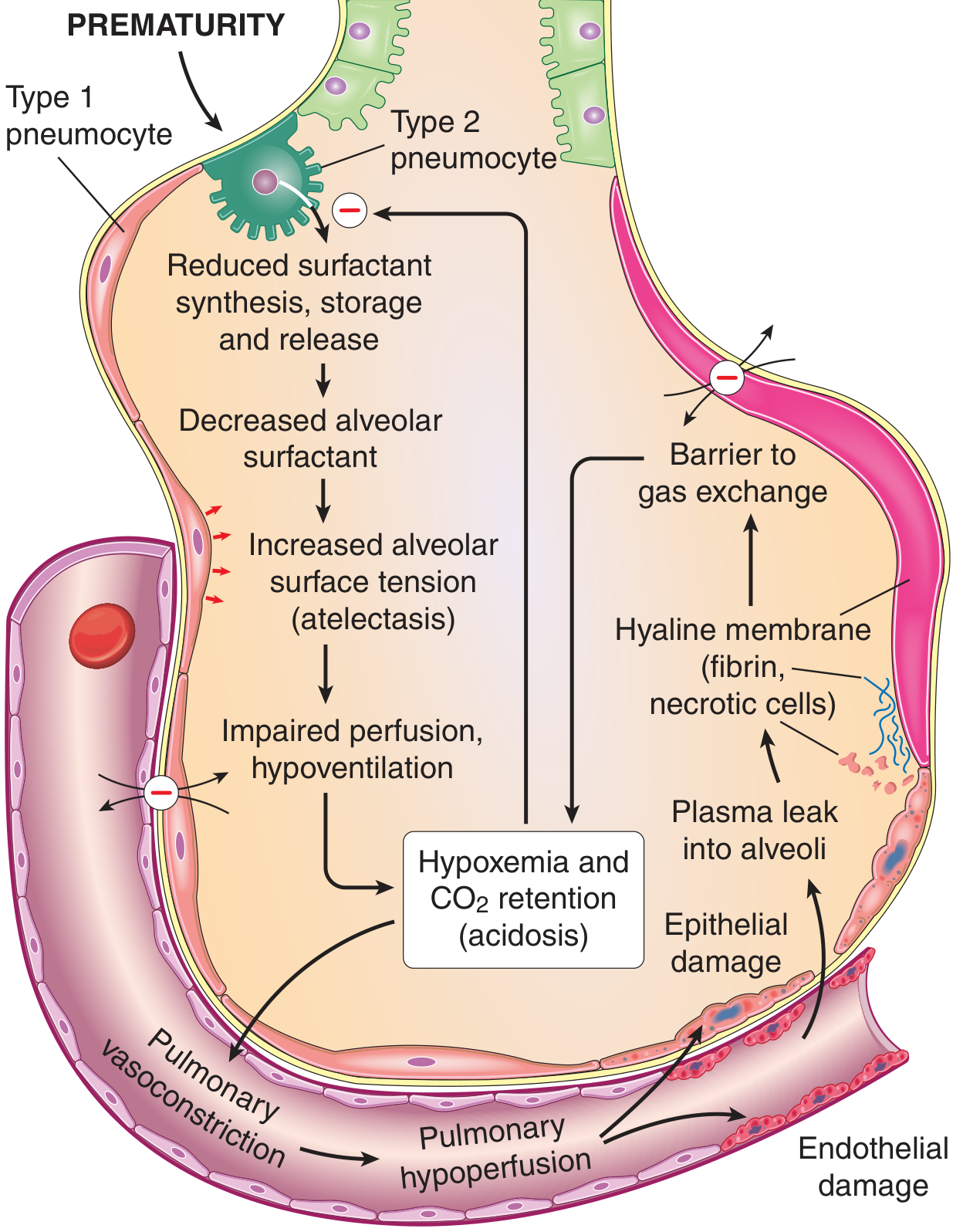
FIG. 4.28 Pathophysiology of RDS - Robbins & Kumar Basic Pathology
The cascade:
- Prematurity → Immature Type II pneumocytes → Reduced surfactant synthesis, storage, and release
- Decreased alveolar surfactant → Increased alveolar surface tension → alveolar collapse (atelectasis)
- Atelectasis → Impaired perfusion, hypoventilation
- → Hypoxemia + CO₂ retention (acidosis)
- Acidosis + hypoxia → Pulmonary vasoconstriction → Pulmonary hypoperfusion
- Hypoperfusion → Endothelial damage and epithelial damage
- Damage → Plasma leaks into alveoli → plasma proteins (fibrin, fibrinogen) mix with necrotic cells
- → Formation of Hyaline Membranes → barrier to gas exchange
- Hyaline membranes + surfactant inactivation → further surfactant deficiency (vicious cycle)
Morphology (Pathology)
- Lungs: Normal size but heavy, relatively airless, mottled purple color.
- Microscopy:
- Poorly developed, collapsed (atelectatic) alveoli
- Eosinophilic hyaline membranes lining respiratory bronchioles, alveolar ducts, and alveoli
- Membranes contain: necrotic Type II pneumocytes + extravasated plasma proteins (mainly fibrin)
- No significant neutrophilic infiltrate
- If infant survives days: Type II pneumocyte proliferation + interstitial fibrosis (repair)
Clinical Features
- Presents within hours of birth
- Progressive tachypnoea, grunting, nasal flaring, intercostal retractions
- Cyanosis
- Worsens over first 2-3 days; recovery begins by day 3-4 (if treated)
- Chest X-ray: Diffuse ground-glass opacification ("white-out"), air bronchograms, diminished lung volumes
Treatment and Prevention
| Approach | Details |
|---|---|
| Antenatal corticosteroids (betamethasone/dexamethasone to mother) | Accelerates fetal lung maturity and surfactant production; given at 24-34 weeks if preterm delivery threatened |
| Exogenous surfactant replacement | Given intratracheally at birth to premature infants (<28 weeks); dramatically reduces mortality |
| CPAP / mechanical ventilation | Maintains alveolar patency |
| Supplemental oxygen | Monitor carefully - prolonged hyperoxia causes complications |
| Assessment of fetal lung maturity | Lecithin/sphingomyelin (L/S) ratio in amniotic fluid (>2 = lung maturity) |
Complications of oxygen therapy:
- Retinopathy of prematurity (retrolental fibroplasia) - VEGF dysregulation causing retinal neovascularization
- Bronchopulmonary dysplasia - decreased alveolar septation, dysmorphic capillary configuration
Adult RDS (ARDS) - Brief Note
-
In adults, surfactant dysfunction occurs due to inactivation (not developmental deficiency).
-
Causes: sepsis, trauma, aspiration, pneumonia, burns.
-
Mechanism: microvascular injury → protein and fluid leak into alveoli → surfactant inactivated by albumin, immunoglobulins, fibrinogen, fatty acids, lyso-PC.
-
Treatment: ventilatory support + prone positioning (exogenous surfactant has NOT been shown to benefit adult ARDS).
-
Robbins & Kumar Basic Pathology; Fishman's Pulmonary Diseases and Disorders; Medical Physiology (Boron & Boulpaep); Histology: A Text and Atlas (Ross & Pawlina); Langman's Medical Embryology
Define Surfactant Through The Following :************ A) Composition B) Source And Secretion C) Functions**** D) Respiratory Distress Syndrome
This question was answered in detail just above in our conversation. Here is the complete answer again for your reference:
Surfactant - Complete SAQ Answer
A) Composition
Pulmonary surfactant is a complex mixture of phospholipids (~90%) and proteins (~10%) lining the alveolar epithelium.
Lipid Component (~90%)
| Component | Details |
|---|---|
| Dipalmitoylphosphatidylcholine (DPPC) - also called dipalmitoyl lecithin | Most important; accounts for almost all surface tension-reducing properties |
| Phosphatidylglycerol | Second most abundant phospholipid |
| Other phospholipids | Phosphatidylethanolamine, phosphatidylinositol, sphingomyelin |
| Neutral lipids | Cholesterol, triglycerides |
Protein Component (~10%) - Four Surfactant Apoproteins (SP)
| Protein | Type | Function |
|---|---|---|
| SP-A | Hydrophilic (collectin) | Most abundant SP. Regulates surfactant homeostasis. Modulates immune responses to viruses, bacteria, fungi. |
| SP-B | Hydrophobic | Transforms lamellar body into surface film. Critical for adsorption and spreading of surfactant onto alveolar epithelium. |
| SP-C | Hydrophobic | ~1% of total SP. Works with SP-B to orient DPPC and maintain thin film layer. |
| SP-D | Hydrophilic (collectin) | Primary host defence. Binds Gram-negative bacteria; modulates innate immunity. |
Structure:
- Superficial layer (facing alveolar air): surface-active phospholipids (mainly DPPC)
- Deep layer / Hypophase: surface-active phospholipids linked to protein
B) Source and Secretion
Source
- Type II alveolar pneumocytes (granular pneumocytes / septal cells) - the sole producers of surfactant.
- Type II cells cover only ~5% of alveolar surface but are metabolically the most active alveolar cells.
- SP-B is also expressed by club cells (Clara cells) of bronchioles; SP-C is exclusive to Type II cells.
Intracellular Synthesis Pathway
- Phospholipids + proteins synthesized in endoplasmic reticulum
- Processed via Golgi complex and multivesicular bodies
- Stored in lamellar bodies (characteristic concentric whorled membrane organelles - intracellular storage form)
Secretion Steps
- Lamellar body fuses with apical plasma membrane → exocytosis into alveolar lining fluid
- Released surfactant forms a meshwork called tubular myelin (rich in SP apoproteins) in the aqueous layer
- From tubular myelin → forms surface film at the air-water interface
- Recycled back into Type II cells by endocytosis, or degraded by alveolar macrophages
Stimuli Increasing Secretion
- Lung hyperinflation (sighing, yawning, deep breathing)
- Exercise
- Beta-adrenergic agonists (clinical importance)
- Corticosteroids (stimulate synthesis of lipids AND proteins)
- Labor (stimulates synthesis)
- Fetal stress / intrauterine growth restriction (via increased cortisol)
Factors Suppressing Maturation
- Prematurity (<35 weeks) - immature Type II cells
- Maternal diabetes - high fetal insulin suppresses surfactant synthesis
- Elective caesarean section before labor onset
Fetal Development Timeline
- Type II cells differentiate and begin surfactant synthesis from ~week 20 of gestation
- Clinically adequate amounts produced after ~35 weeks gestation
- A surge in maternal glucocorticoids just before birth triggers the final maturation
C) Functions
1. Reduces Alveolar Surface Tension (Primary Function)
- By Laplace's Law: Pressure = 2T/r
- Without surfactant: small alveoli (small r) have higher recoil pressure and empty into larger ones → atelectasis
- Surfactant lowers tension as alveoli shrink (concentration rises at smaller surface area) → tension drops proportionally → prevents collapse on expiration
2. Increases Lung Compliance
- Lower surface tension = less elastic recoil = easier to inflate lungs
- Without surfactant, compliance drops 2x or more, forcing enormous inspiratory effort with every breath
3. Prevents Pulmonary Oedema
- High surface tension (without surfactant) would suck fluid from interstitium into alveoli
- Surfactant keeps tension low → alveoli remain dry → diffusion distance is minimized
4. Maintains Alveolar Stability (Equalises Pressure Across Alveoli)
- Small and large communicating alveoli maintain equal transpulmonary pressure
- Prevents small alveoli from emptying into large ones (prevents inter-alveolar instability)
5. Reduces Work of Breathing
- Improved compliance + alveolar stability = significantly less muscular effort required per breath
6. Promotes Uniform Ventilation
- Dynamically adjusts surface tension during inflation/deflation cycles → uniform ventilation across all alveoli
7. Innate Immune Defence (SP-A and SP-D)
- Opsonise bacteria, viruses, fungi → promote phagocytosis by alveolar macrophages
- Modulate local inflammatory response to inhaled antigens and acute lung injury
D) Respiratory Distress Syndrome (RDS)
Synonyms: Infant/Neonatal RDS (IRDS/NRDS) | Hyaline Membrane Disease (HMD)
Aetiology
Primary cause: Insufficient surfactant synthesis by immature Type II pneumocytes in the premature lung.
Incidence by gestational age:
- < 28 weeks: ~60%
- 28-34 weeks: ~30%
-
34 weeks: < 5%
Additional risk factors: Male sex, maternal diabetes, elective caesarean section (before labour), perinatal asphyxia
Protective factors: Intrauterine stress / fetal growth restriction (raises cortisol), antenatal corticosteroids to mother
Pathogenesis - The Vicious Cycle
Pathophysiology of RDS - Robbins & Kumar Basic Pathology
| Step | Event |
|---|---|
| 1 | Prematurity → Immature Type II cells → Reduced surfactant synthesis, storage, release |
| 2 | Decreased alveolar surfactant → Increased surface tension → Alveolar collapse (atelectasis) |
| 3 | Atelectasis → Impaired perfusion + hypoventilation |
| 4 | → Hypoxaemia + CO₂ retention (respiratory acidosis) |
| 5 | Acidosis + hypoxia → Pulmonary vasoconstriction → Pulmonary hypoperfusion |
| 6 | → Endothelial + Epithelial damage |
| 7 | → Plasma leak into alveoli (fibrinogen, fibrin, necrotic cells) |
| 8 | → Hyaline membrane formation → barrier to gas exchange |
| 9 | Membranes inactivate remaining surfactant → worsening surfactant deficiency (vicious cycle) |
Morphology (Histopathology)
- Macroscopy: Lungs normal size but heavy, airless, mottled purple
- Microscopy:
- Collapsed (atelectatic) alveoli alternating with dilated alveolar ducts
- Eosinophilic hyaline membranes lining respiratory bronchioles, alveolar ducts, and alveoli
- Membranes composed of: necrotic Type II pneumocytes + extravasated plasma proteins (fibrin)
- No significant neutrophilic infiltrate
- Survivors: Type II pneumocyte proliferation + interstitial fibrosis (repair phase)
Clinical Features
- Presents within hours of birth
- Progressive tachypnoea, grunting (positive end-expiratory pressure self-generated), nasal flaring, intercostal retractions
- Cyanosis
- Worsens over 2-3 days; recovery begins by day 3-4 if treated
- CXR: Diffuse bilateral ground-glass ("white-out"), air bronchograms, low lung volumes (atelectasis)
Treatment and Prevention
| Approach | Details |
|---|---|
| Antenatal corticosteroids (betamethasone / dexamethasone to mother) | Accelerates fetal lung maturity and surfactant production; given 24-34 weeks if preterm delivery threatened |
| Exogenous surfactant replacement (intratracheal) | Prophylactic at birth for <28 weeks; dramatically reduces mortality |
| CPAP / mechanical ventilation | Maintains alveolar patency |
| Supplemental O₂ | Use carefully - prolonged hyperoxia causes complications |
| L/S ratio (amniotic fluid) | Lecithin/Sphingomyelin ratio >2 = fetal lung maturity |
Complications of O₂ therapy:
- Retinopathy of prematurity (retrolental fibroplasia) - VEGF dysregulation → retinal neovascularisation
- Bronchopulmonary dysplasia - decreased alveolar septation, dysmorphic capillary configuration
ARDS in Adults - Key Difference
| Feature | Neonatal RDS | Adult ARDS |
|---|---|---|
| Cause | Surfactant deficiency (developmental) | Surfactant inactivation (by plasma proteins leaking into alveoli) |
| Trigger | Prematurity | Sepsis, trauma, aspiration, pneumonia |
| Surfactant therapy | Highly effective | Not proven beneficial in adults |
| Treatment | Surfactant + CPAP + antenatal steroids | Ventilatory support + prone positioning |
- Robbins & Kumar Basic Pathology; Fishman's Pulmonary Diseases and Disorders; Medical Physiology (Boron & Boulpaep); Histology: A Text and Atlas (Ross & Pawlina); Langman's Medical Embryology
This is a shared conversation. Sign in to Orris to start your own chat.