Epilepsy
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
"epilepsy" AND "management"
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Epilepsy - Comprehensive Medical Student Review
1. Definition
Epilepsy is a disease of the brain defined by the 2014 ILAE criteria as any ONE of:
- At least two unprovoked (or reflex) seizures occurring >24 hours apart
- One unprovoked seizure with a probability of further seizures ≥60% over the next 10 years (e.g., after a single seizure with a structural lesion on MRI, or epileptiform EEG)
- Diagnosis of an epilepsy syndrome
Key distinction: A seizure is a single event of abnormal excessive hypersynchronous neuronal activity. Epilepsy is the underlying disease predisposing to recurrent seizures. Provoked seizures (e.g., alcohol withdrawal, hypoglycemia, hyponatremia) are not epilepsy.
- Bradley and Daroff's Neurology in Clinical Practice
2. Pathophysiology
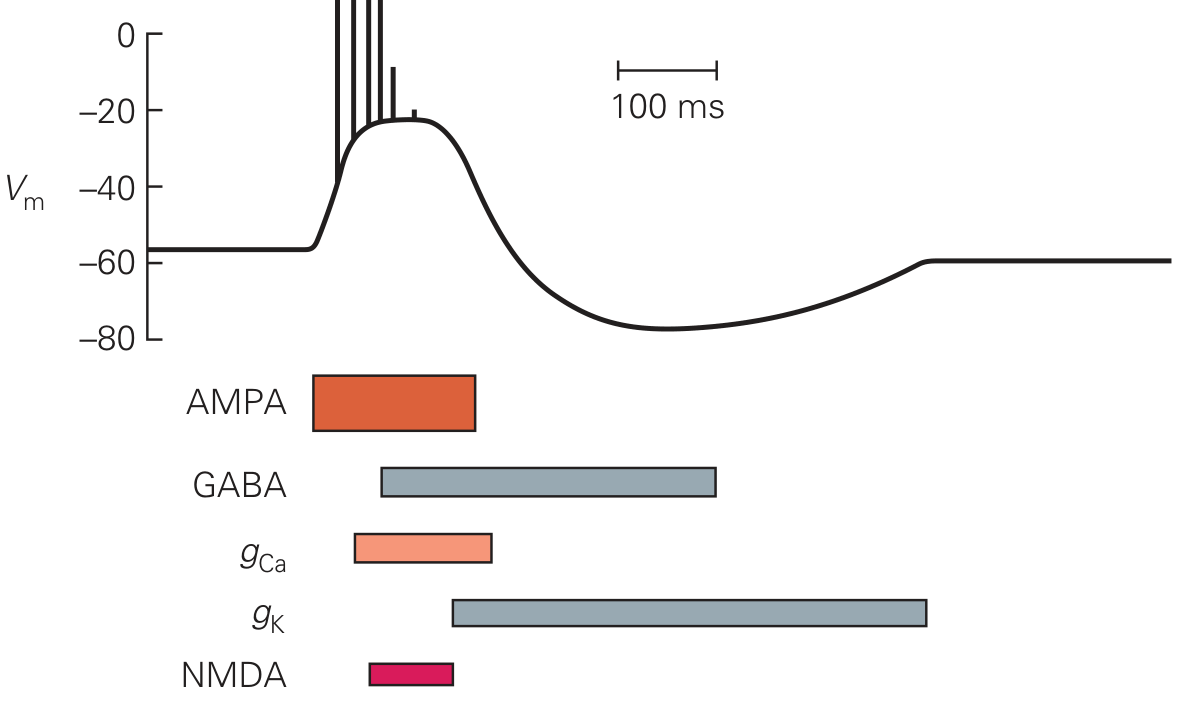
The Paroxysmal Depolarizing Shift (PDS)
The fundamental cellular event is the paroxysmal depolarizing shift - a massive, prolonged depolarization of neurons in a seizure focus driven by:
- AMPA- and NMDA-type glutamate receptor-channels (excitatory input)
- Voltage-gated Ca²⁺ channels (gCa) amplifying depolarization
- Followed by hyperpolarization via: GABA-A receptors (Cl⁻), GABA-B receptors (K⁺), and Ca²⁺-activated K⁺ channels (gK)
The PDS represents exaggerated excitation in a seizure focus. The afterhyperpolarization normally limits seizure duration. When it fails, seizures propagate.
Seizure Spread
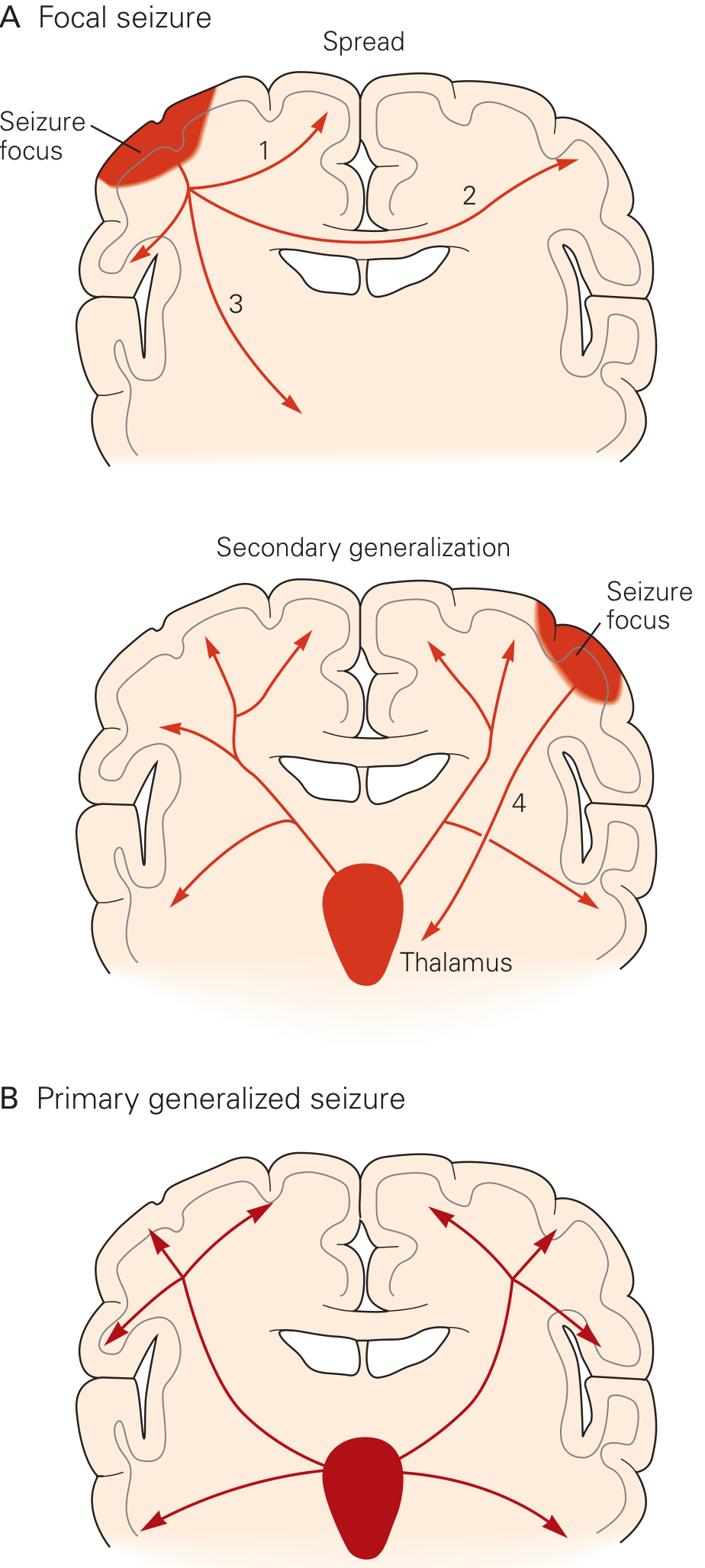
- Focal seizure: Starts in a focus, spreads via intrahemispheric fibers (1), to homotopic contralateral cortex via corpus callosum (2), and to subcortical centers (3)
- Secondary generalization: Thalamic involvement (4) propagates activity to both hemispheres simultaneously
- Primary generalized seizure: Both hemispheres activated simultaneously from onset via thalamocortical circuits (Panel B above)
Eric Kandel, Principles of Neural Science, 6th Ed.
Imbalance Summary (Exam High-Yield)
| Mechanism | Result |
|---|---|
| ↑ Glutamate (AMPA/NMDA) | ↑ Excitation → seizure |
| ↓ GABA-A/B function | ↓ Inhibition → seizure |
| Na⁺ channel dysfunction | Repetitive firing |
| T-type Ca²⁺ channel ↑ | Absence seizures (thalamocortical circuits) |
3. ILAE Classification (2017) - Three Levels
The 2017 ILAE framework has three levels. Classification at all three is ideal but not always achievable.
Level 1: SEIZURE TYPE
↓
Level 2: EPILEPSY TYPE
↓
Level 3: EPILEPSY SYNDROME
+ ETIOLOGY (at every level)
+ COMORBIDITIES
Level 1 - Seizure Types
A. Focal-Onset Seizures (arise from one hemisphere)
- Focal aware (previously "simple partial") - consciousness preserved
- Focal impaired awareness (previously "complex partial") - consciousness impaired
- Focal to bilateral tonic-clonic (previously "secondarily generalized")
Focal features by lobe of origin:
| Lobe | Typical Features |
|---|---|
| Temporal | Aura (déjà vu, rising epigastric sensation), automatisms (lip-smacking, hand fumbling), post-ictal confusion |
| Frontal | Motor signs, brief seizures, nocturnal, may generalize rapidly |
| Parietal | Sensory symptoms, tingling, numbness |
| Occipital | Visual hallucinations (lights, colors) |
B. Generalized-Onset Seizures (both hemispheres from onset)
| Type | Key Features |
|---|---|
| Absence (typical) | Sudden behavioral arrest + staring, 3-20 sec, no post-ictal phase, 3 Hz spike-wave on EEG |
| Absence (atypical) | Slower onset/offset, often in Lennox-Gastaut syndrome |
| Myoclonic | Brief (<100 ms) involuntary muscle jerks; morning predominance in JME |
| Tonic | Sustained muscle contraction, trunk/limb stiffening |
| Clonic | Rhythmic jerking movements |
| Tonic-clonic (GTC) | Tonic phase → clonic phase; post-ictal drowsiness/confusion |
| Atonic | Sudden loss of muscle tone ("drop attacks") |
| Epileptic spasms | West syndrome; flexion/extension of trunk |
C. Unknown Onset
Level 2 - Epilepsy Types
- Focal epilepsy
- Generalized epilepsy
- Combined generalized and focal (e.g., Dravet syndrome)
- Unknown
Level 3 - Common Epilepsy Syndromes (High-Yield)
| Syndrome | Age of Onset | Seizure Type | EEG | Key Feature |
|---|---|---|---|---|
| Childhood Absence Epilepsy (CAE) | 4-8 yr | Typical absence | 3 Hz generalized spike-wave | Hyperventilation triggers; ethosuximide/valproate |
| Juvenile Myoclonic Epilepsy (JME) | Adolescence | Myoclonic + GTC ± absence | 4-6 Hz polyspike-wave; morning | Lifelong treatment usually needed |
| Benign Rolandic Epilepsy (BECTS) | 3-13 yr | Focal sensorimotor face/arm | Centrotemporal spikes | Often outgrown by puberty |
| West Syndrome | 3-7 months | Epileptic spasms (clusters) | Hypsarrhythmia | ACTH/vigabatrin treatment |
| Lennox-Gastaut Syndrome | 1-7 yr | Multiple types (tonic, atonic, absence) | Slow (<2.5 Hz) spike-wave | Developmental regression, refractory |
| Dravet Syndrome | <1 yr | Febrile + afebrile GTC | Polyspike-wave | SCN1A mutation; sodium channel blockers WORSEN it |
| Temporal Lobe Epilepsy (TLE) | Any | Focal impaired awareness + GTC | Temporal spikes/sharp waves | Most common adult focal epilepsy; mesial TLE with hippocampal sclerosis |
4. Etiology
The ILAE 2017 framework emphasizes identifying the etiology at every classification level:
| Etiology Category | Examples |
|---|---|
| Structural | Hippocampal sclerosis, cortical dysplasia, tumors, stroke, trauma, encephalitis |
| Genetic | SCN1A (Dravet), KCNQ2, DEPDC5, chromosomal (Down, Angelman) |
| Infectious | Neurocysticercosis, HSV encephalitis, HIV |
| Metabolic | Pyridoxine deficiency, mitochondrial disease, PKU |
| Immune | Anti-NMDAR encephalitis, LGI1, CASPR2 antibodies |
| Unknown | ~50% of all epilepsies |
5. Clinical Assessment & Diagnosis
History (most important diagnostic tool)
- Full description of the episode (from witness): onset, progression, duration
- Pre-ictal aura (points to focal onset)
- Ictal features: automatisms, motor activity, eye deviation, head turn
- Post-ictal: confusion (Todd's paralysis, aphasia), duration
- Provoking factors, sleep deprivation, alcohol, medications
- Family history, birth history, febrile seizures
EEG (Electroencephalogram)
- Interictal EEG: Spike-and-wave discharges between seizures
- 3 Hz generalized spike-wave = absence epilepsy
- Centrotemporal spikes = BECTS
- Hypsarrhythmia = West syndrome
- Focal temporal spikes = TLE
- Ictal EEG: Rhythmic activity corresponding to clinical seizure
- EEG is normal in 50% of patients with epilepsy on a routine interictal recording
- Sleep deprivation, hyperventilation, and photic stimulation are activation procedures
- EEG bands: delta (0.5-4 Hz), theta (4-7 Hz), alpha (8-13 Hz), beta (13-30 Hz)
Neuroimaging
- MRI brain (preferred over CT): Structural causes (hippocampal sclerosis, tumors, dysplasia)
- FLAIR and T2 sequences most sensitive for cortical abnormalities
- CT head: Used acutely to exclude hemorrhage/mass
Initial Investigations for New-Onset Seizures
- Blood glucose, electrolytes (Na⁺, Ca²⁺, Mg²⁺), renal/liver function, FBC
- Toxicology screen
- EEG
- MRI brain
- LP if encephalitis/meningitis suspected
6. Antiseizure Medications (ASMs) - High-Yield Table
| Drug | Mechanism | Indications | Key Adverse Effects |
|---|---|---|---|
| Valproic acid | Na⁺ channel + GABA ↑ + T-Ca²⁺ ↓ + NMDA ↓ (multiple) | Focal + generalized + absence | Hepatotoxicity, teratogen (neural tube defects), weight gain, thrombocytopenia, pancreatitis |
| Phenytoin | Na⁺ channel inhibitor | Focal + generalized | Zero-order kinetics, gingival hyperplasia, hirsutism, nystagmus, ataxia, Stevens-Johnson syndrome; hepatic enzyme inducer |
| Carbamazepine | Na⁺ channel inhibitor | Focal + GTC; TN | Hyponatremia (SIADH), diplopia, SJS (HLA-B*1502 in Asian patients); enzyme inducer |
| Oxcarbazepine | Na⁺ channel inhibitor | Focal seizures | Less enzyme induction than CBZ; hyponatremia |
| Lamotrigine | Na⁺ channel inhibitor | Focal + generalized | Rash (slow titration prevents SJS); slow dose escalation needed; enzyme inducer |
| Levetiracetam | SV2A modulation | Focal + generalized | Mood disturbance, irritability, psychosis; minimal drug interactions |
| Brivaracetam | SV2A modulation (higher affinity) | Focal + generalized | Less psychiatric side effects than levetiracetam |
| Ethosuximide | T-type Ca²⁺ channel ↓ | Absence seizures only | GI upset, headache; NOT effective for focal seizures |
| Topiramate | Na⁺ + GABA ↑ + AMPA ↓ + Ca²⁺ ↓ | Focal + generalized | Cognitive impairment ("Dopamax"), nephrolithiasis, weight loss, glaucoma |
| Phenobarbital | GABA-A potentiation | Focal + generalized | Sedation, cognitive effects; enzyme inducer |
| Lacosamide | Na⁺ channel (slow inactivation) | Focal + generalized | PR interval prolongation |
| Zonisamide | Na⁺ + Ca²⁺ channels | Focal + generalized | Nephrolithiasis, cognitive effects, weight loss |
| Vigabatrin | Irreversible GABA-T inhibitor | Infantile spasms (1st-line); focal | Irreversible peripheral visual field loss |
| Perampanel | AMPA receptor antagonist | Focal + generalized | Dizziness, psychiatric effects |
| Gabapentin/Pregabalin | α2δ Ca²⁺ channel subunit | Focal seizures (adjunct) | Sedation, weight gain |
Adams and Victor's Principles of Neurology, 12th Ed.; Eric Kandel, Principles of Neural Science, 6th Ed.
Drug Selection Principles (High-Yield)
- Absence epilepsy: Ethosuximide (1st-line pure absence), Valproate (if GTC also present)
- Focal epilepsy: Carbamazepine or Lamotrigine (1st-line)
- JME: Valproate (most effective), Lamotrigine, Levetiracetam
- Dravet syndrome: AVOID Na⁺ channel blockers (phenytoin, carbamazepine, lamotrigine - they worsen); use valproate, clobazam, topiramate
- Infantile spasms (West syndrome): ACTH or prednisolone (1st-line); vigabatrin (especially in TSC)
- Women of childbearing age: Avoid valproate if possible (teratogenicity); lamotrigine preferred
7. Management Principles
When to Start Treatment
- After two unprovoked seizures - start ASM
- After one seizure with high recurrence risk (structural lesion, epileptiform EEG, epilepsy syndrome)
- After one seizure alone - treatment not automatically required
Monotherapy First
- Start with a single ASM at low dose and titrate
- Failure of two appropriately chosen and dosed ASMs defines drug-resistant epilepsy (~30% of patients)
Drug-Resistant Epilepsy
- Surgical evaluation is the 1st-line treatment for drug-resistant focal epilepsy
- Most common surgery: Anterior temporal lobectomy (for mesial TLE)
- Other surgical options: Corpus callosotomy (drop attacks), hemispherectomy
- Neuromodulation: Vagus nerve stimulation (VNS), responsive neurostimulation (RNS), deep brain stimulation (DBS - anterior nucleus of thalamus)
- Ketogenic diet: High-fat, low-carbohydrate; especially useful in pediatric drug-resistant epilepsy
Stopping ASMs
- Typically considered after 2 years seizure-free
- EEG guides decision - normal EEG = better prognosis
- Gradual taper over weeks-months
- Discuss driving implications
8. Status Epilepticus (SE)
Definition: Seizure lasting ≥5 minutes, OR two or more seizures without full recovery between them.
Convulsive SE lasting >30 min carries mortality up to 20%.
Most Common Cause
- Non-compliance with ASM (most common cause of tonic-clonic SE)
Management Protocol (Time-Critical)
0-5 min: ABCs, IV access, O2, glucose, vitals, bloods
Benzodiazepine (FIRST-LINE):
- IV Lorazepam 0.1 mg/kg (drug of FIRST choice in hospital)
- IM Midazolam (out-of-hospital or no IV access)
- Rectal Diazepam (community)
5-20 min: If seizure continues → SECOND-LINE:
- IV Levetiracetam, OR
- IV Valproate, OR
- IV Phenytoin/Fosphenytoin
20-40 min: If refractory SE → THIRD-LINE:
- Anaesthetic doses: Propofol, Thiopental, Midazolam infusion
- ICU admission, EEG monitoring
Super-refractory SE (>24h despite anaesthesia):
- Ketamine, Ketogenic diet, Immunotherapy
Plum and Posner's Diagnosis and Treatment of Stupor and Coma; Swanson's Family Medicine Review
9. Special Situations
Epilepsy in Pregnancy
- Discuss contraception - enzyme-inducing ASMs (phenytoin, carbamazepine, phenobarbital) reduce efficacy of oral contraceptives
- Valproate has highest teratogenic risk (10x neural tube defects, neurodevelopmental effects) - avoid if possible
- Lamotrigine and levetiracetam are preferred in pregnancy
- Folic acid supplementation (5 mg/day) for all women on ASMs planning pregnancy
- AAN/AES 2024 Practice Guideline (PMID: 38748979): confirms teratogenesis risk hierarchy and recommends shared decision-making
Sudden Unexpected Death in Epilepsy (SUDEP)
- Leading cause of epilepsy-related death
- Rate: ~1 in 1000 person-years; higher in drug-resistant epilepsy
- Mechanism: Postictal cardiorespiratory failure, possibly postictal generalized EEG suppression
- Risk reduction: Better seizure control, avoid nocturnal seizures, use of safety pillows
Non-Epileptic Attack Disorder (NEAD / PNES)
- Psychogenic non-epileptic seizures (PNES) - must be distinguished from epilepsy
- Often present with motor seizures but no EEG correlate
- Video-EEG monitoring is the gold standard for diagnosis
10. Exam High-Yield Summary
| Topic | Key Fact |
|---|---|
| ILAE 2014 definition | 2 unprovoked seizures, OR 1 seizure with ≥60% recurrence risk |
| Single seizure rule | "A single seizure does not epilepsy make" |
| 3 Hz spike-wave EEG | Childhood absence epilepsy |
| Hypsarrhythmia | West syndrome (infantile spasms) |
| Na⁺ channel blockers WORSEN | Dravet syndrome (SCN1A mutation) |
| 1st choice for absence only | Ethosuximide |
| 1st choice SE (IV) | Lorazepam |
| Teratogen with highest risk | Valproate |
| Drug-resistant epilepsy defined by | Failure of 2 adequate trials of ASMs |
| Most common adult focal epilepsy | Mesial temporal lobe epilepsy (hippocampal sclerosis) |
| JME characteristic time | Morning myoclonic jerks after waking |
| Vigabatrin irreversible toxicity | Visual field loss (bilateral) |
| Surgery for drug-resistant focal | Anterior temporal lobectomy |
Sources: Bradley and Daroff's Neurology in Clinical Practice; Eric Kandel, Principles of Neural Science, 6th Ed.; Adams and Victor's Principles of Neurology, 12th Ed.; AAN/AES Practice Guideline 2024 (PMID: 38748979)
This is a shared conversation. Sign in to Orris to start your own chat.